Article Text

Abstract
Brain–computer interface (BCI) technology translates brain activity into meaningful commands to establish a direct connection between the brain and the external world. Neuroscientific research in the past two decades has indicated a tremendous potential of BCI systems for the rehabilitation of patients suffering from poststroke impairments. By promoting the neuronal recovery of the damaged brain networks, BCI systems have achieved promising results for the recovery of poststroke motor, cognitive, and language impairments. Also, several assistive BCI systems that provide alternative means of communication and control to severely paralysed patients have been proposed to enhance patients’ quality of life. In this article, we present a perspective review of the recent advances and challenges in the BCI systems used in the poststroke rehabilitation of motor, cognitive, and communication impairments.
- stroke Rehabilitation
- brain
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Stroke is a leading cause of adult disabilities and is associated with a significant socioeconomic burden. The neurological damage caused by a stroke results in a multitude of functional impairments. Approximately 30% of stroke survivors suffer from some form of long-term motor, cognitive, language, and speech-related deficits.1 Hence, significant efforts are ongoing to develop innovative therapies that can improve stroke patients’ quality of life. In the last decade, the technology of brain–computer interfacing (BCI) has shown very promising results.
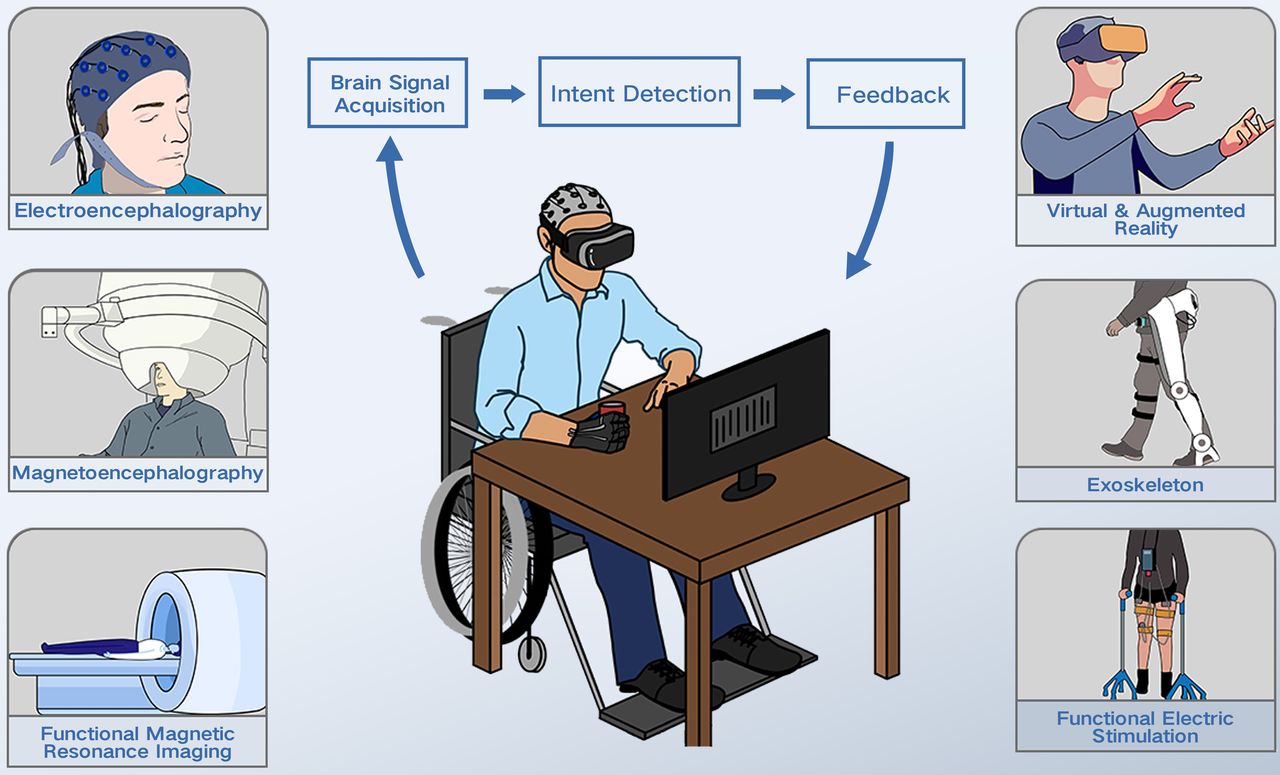
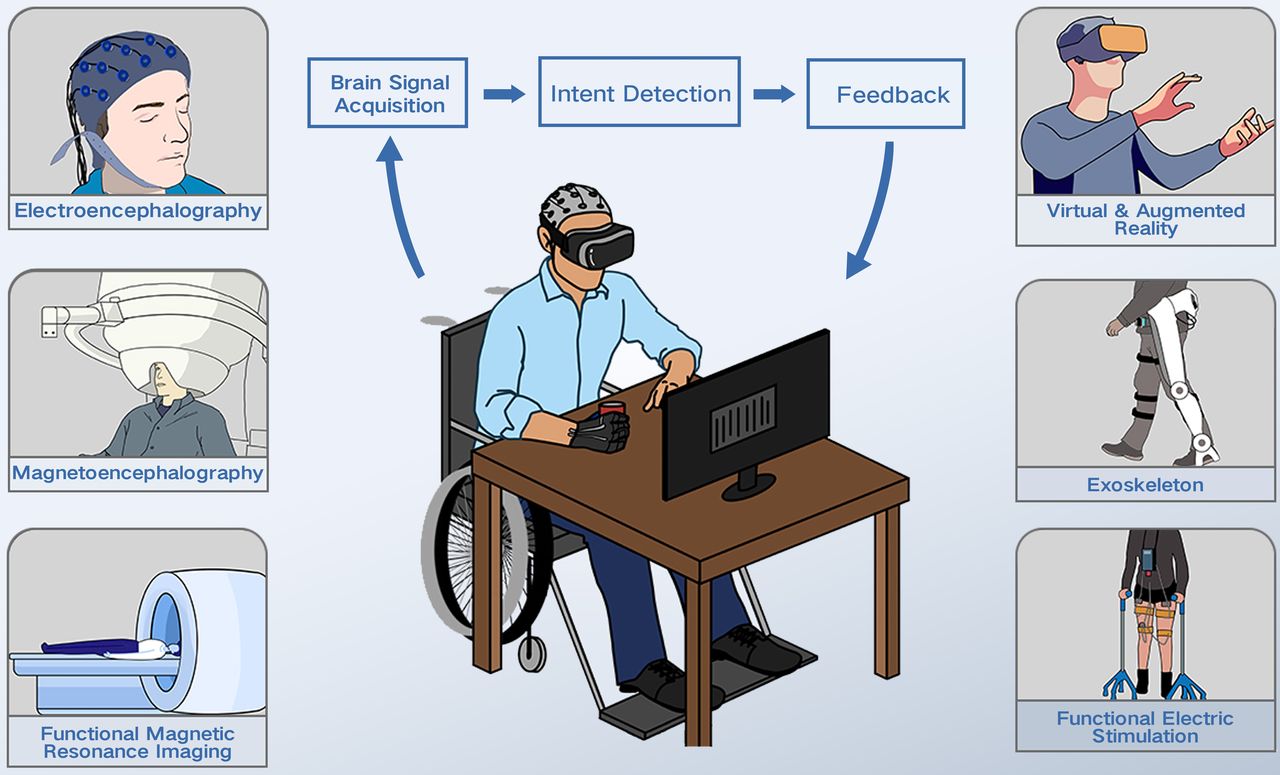
BCI systems establish a direct communication link between the brain and a computer by decoding users’ intentions from their brain activation patterns to control an external environment. As presented in figure 1, a typical BCI system consists of three components; a brain signal acquisition device that captures the brain dynamics, a signal decoding algorithm that translates the observed brain activation patterns into an actionable control signal as per the user’s intentions, and a feedback device that communicates the decoded user intensions in a user perceivable feedback.2 To improve the quality of life among patients who had a stroke, primarily two types of BCI systems have been studied. The rehabilitative BCIs aim to restore the stroke-induced loss of functions by stimulating the recovery of damaged neuronal circuits in the brain. The assistive BCIs aim to completely bypass the damaged pathways by using BCI as an alternative means of communication and control. References 2–4 have presented a thematic review of some of these BCI systems and their use in patients who had a stroke. This review focuses on the state-of-the-art BCI systems that have been employed to improve stroke patients’ quality of life and discusses the recent advances, challenges, and future research directions in this domain. We first focus on rehabilitative BCIs and present the neurological basis of BCI-stimulated brain restoration mechanisms. Next, we present recent advances in BCI systems used for motor rehabilitation. This is followed by a review of a significantly less explored topic of BCI-mediated poststroke cognitive and speech rehabilitation. Lastly, we review the latest advances in assistive BCI systems for patients who had a stroke.
{kind=link}
An overview of the brain-computer interface system (BCI) for stroke rehabilitation. Any BCI system is composed of primarily three components; a brain signal acquisition device, a signal decoding algorithm, and a feedback device.
Neuroplastic principles of rehabilitative BCIs
Rehabilitative BCIs aim for the recovery or relearning of lost functions from stroke by effective elicitation of functional and structural reorganisations in the brain. The ability of the brain to undergo experience-based structural and functional modification throughout its life is termed neuroplasticity and it forms the basis of all the poststroke restorative efforts.5 6 Several neuroimaging studies have shown evidence of significant structural and functional reorganisation in the brain following poststroke rehabilitative interventions.5 7 Therefore, the effectiveness of any rehabilitative intervention will depend on its ability to promote restorative neuroplasticity.
Promoting neuroplasticity follows a two-staged process. In the initial phase, functional plasticity, which is associated with the changes in synaptic efficacy takes place at a time scale of a few minutes to days. Changes in the synaptic strength in form of long-term potentiation/long-term depression have been observed to be strongly associated with the acquisition of new skills and formation of memory.8 These changes are derived from the experience stimulated embodiment of specific spatiotemporal activation of neuronal populations that lead to the changes in the strengths of the neuronal connections and possible activation of the previously silent synapses. In the later phase, over days and weeks, the functional plasticity promotes consolidation of learning in a form of structural changes in the brain. These changes can manifest in a form of modification of the connectivity patterns, formations of new synapses and axons, and changes in the branching of axons and dendrites and are indicative of the long-lasting modifications stimulated by any particular intervention.9
BCI uses four different mechanisms to stimulate the abovementioned neuroplastic changes and to improve patients' functional capabilities. The first is referred to as neurofeedback training, wherein patients volitionally modulate their brain activations in the desired way.10 Here, patients are presented with a visual or auditory representation of a brain signal of interest and are asked to up- or down-regulate these signals by consciously controlling their thought process. These systems usually select stroke-induced abnormal brain activations as the signal of interest.Reduced cortical activity, slowing of electroencephalography (EEG) rhythms, reduced sensorimotor rhythm (SMR) power and increased interhemispheric asymmetry are a few such abnormal brain activations that have been observed to be associated with poststroke motor and cognitive impairments.11–13 The patients are then asked to modulate these signals to their state observed in healthy people and this regulation has been postulated to result in functional restoration. Multiple BCI-based poststroke motor rehabilitation studies have used this method wherein patients were asked to increase the sensorimotor cortical activity in mu and beta bands to improve the arm motor functions.14 15 The sustained functional improvements observed in these studies have provided the experimental validation of the benefits of neurofeedback training. Although proved to be beneficial, identification of the most optimal brain signal of interest which can be targeted to realise the desired functional improvement is a difficult task and is one of the most important challenges faced by neurofeedback-based BCIs.
Reinforcement-based operant conditioning, wherein, the brain state and resultantly the human behaviour, is modified by modulating the reward associated with any action is the second mechanism of BCI-based neuroplasticity stimulation.16 In the operant conditioning mechanism, the BCI system is used to identify the compliance of the user in performing a specific mental task of interest, and a successful attempt of task performance is rewarded with positive feedback whereas failed attempt is presented with no or negative feedback. As an example, in motor rehabilitative BCI systems, successful imagination of motor movement by the user is rewarded with the actual movement of the affected limb whereas failed attempts do not produce any reward.17 Such reward-based conditioning has been thought to result in brain modification in the same manner as the human brain learns to interact with novel environments. Furthermore, this mechanism, as it focuses on a mental task instead of the particular brain rhythm, does not necessitate a prior identification of characteristic abnormal brain activations, which is the case with neurofeedback-based BCIs.
Repetitive engagement, wherein the patients repetitively perform actions like motor movements, and in turn, repeatedly engage all the associated neuronal circuits, is the third mechanism to stimulate neuroplasticity. Repetitive engagement of stroke-affected neuronal circuits may result in the strengthening of the existing connections and formation of new axonal connections and this may lead to functional improvements.5 As the coordination between multiple brain systems is essential for the successful completion of any task, task-focused repetitive engagement may improve not only individual brain systems but also the coordination and neuronal connections between them. In the BCI motor rehabilitation studies designed based on this paradigm,18 19 the neuroimaging analysis has shown improvements in communication highways in the brain like corpus callosum and corticospinal tract20 21 along with the improvements in the motor and the sensorimotor system.11 21
The principle of Hebbian learning which states that the contingent activation of neurons increases the synaptic strength between them is the fourth mechanism stimulated by BCI-based rehabilitative systems. Hebbian learning has most prominently been observed in motor rehabilitation studies. Lack of motor control following stroke results in a gap between motor intension and execution. This gap is created due to the absence of afferent sensory feedback arising as a result of movement execution. It has been observed that this afferent sensory feedback reduces the inhibitory drive on the motor system and hence is essential for effective upregulation of the motor neurons and functional recovery.22 Therefore, BCI systems stimulating this mechanism of neuroplasticity aim to complete the stroke-affected motor intention-action-feedback loop by providing the user with sensory feedback in a form of robotic,23 24 or haptic18 movement following a successful elicitation of motor imagery (MI) or movement execution. Contingent activation of outputs and inputs of the motor cortex can trigger the Hebbian plasticity and result in functional improvements.
Overall, depending on the design of the BCI system and the feedback modality, any rehabilitative BCI system may promote neuroplasticity by any or all the above-mentioned mechanisms.
BCI for poststroke motor rehabilitation
Rehabilitation of patients suffering from severe poststroke motor impairments was the initial motivation that prompted the exploration of the rehabilitative potential of BCI systems. Due to the lack of residual movement capabilities, these patients would be excluded from conventional rehabilitation therapies like physiotherapy or constrained induced movement therapy (CIMT). This necessitated the exploration of novel rehabilitative interventions. In healthy populations, the imagination of motor movements known as MI elicits brain activations that are similar to the actual movement execution, paved a way for BCI-based external control of upper limb motor movements. The first report on the ability of the patients who had a stroke to volitionally control the brain activation patterns, known as SMR, which are commonly associated with MI, was presented by Buch et al.14 In this study, eight patients who had a stroke with chronic upper limb hemiplegia successfully learnt to modulate the oscillatory power in the µ band (frequency 8–12 Hz), which was identified using the magnetoencephalography sensors placed over the sensorimotor area. Successful modulation of the µ rhythm was rewarded with the passive open-close movement of the fingers using a robotic orthosis. Despite the successful demonstration of the feasibility of BCI in patients who had a stroke, this study did not report lasting improvements in motor functions. Ang first reported the clinical improvements in upper limb motor functions using BCI rehabilitation.25 In this study, 8 patients who had a chronic stroke reported an average improvement of 4.9 points on the Fugl-Mayer Assessment scale (FMA) following 12 BCI-based rehabilitative sessions. To date, multiple feasibility and efficacy studies, as well as randomised controlled trials been conducted for BCI-based poststroke motor rehabilitation. In these studies, EEG has evolved as a preferred choice for the acquisition of brain signals due to its low cost, higher temporal resolution and portable nature, but a few studies have also explored the use of other modalities like magnetoencephalography,14 functional MRI26 and functional near-infrared spectroscopy.27 The BCI studies for upper extremity motor rehabilitation have been reviewed in references 2 28 and a systematic meta-analysis of the clinical benefits is presented in references 4 29–31.
Quantifying the clinical benefits of the BCI intervention, a meta-analysis reported by Cervera et al has observed that BCI intervention is associated with a standardised mean difference (SMD) of 0.79 on the upper extremity FMA scale. This effect size is comparable with other widely used therapies like CIMT (SMD=0.81), mirror therapy (SMD=0.61) and robotics (SMD=0.35).4 A more recent meta-analysis by Bai et al concluded that the BCI intervention shows a medium effect size (SMD=0.42) for post-intervention functional gains.30 Moreover, a significant variation has been observed in the clinical benefits of different BCI rehabilitation studies. This heterogeneity could be attributed to differences in the patient-specific characteristics like demographics, age, impairment levels, time poststroke, lesion properties and differences in the intervention design, like the type of the external feedback, accuracy of the decoder, session intensity and the total number of rehabilitation sessions.
The design of the feedback modality may have a significant impact on the BCI-mediated rehabilitation gains. In this regard, studies have traditionally explored the use of visual displays, orthotic devices, robotic mechanisms, hand exoskeletons, functional electric stimulation (FES) and combinations of them as a feedback mechanism (see reference 2 for an exhaustive list of the studies). Although, all these mechanisms have been observed to elicit functional recovery, how the design of the feedback paradigm affects clinical recovery is still not very well understood. Empirical evidence from meta-analyses, although statistically insignificant, suggest that the BCI-FES system, which produces controlled muscle movements by electrical stimulation, may lead to the best possible motor recovery.29 31 These higher gains could be partially attributed to the positive effect FES has on cortical excitability.32 Furthermore, the same meta-analyses, although statistically insignificant, indicate that realistic visual feedback may elicit the next best motor improvements with the robotic feedback being the least effective one. These empirical observations indicate that the muscle movements may not always be necessary and realistic visual feedback that imparts a sense of ownership/agency to the user may bring out a similar level of motor recovery using BCI paradigms. Consequently, virtual and augmented reality-based (VR and AR) feedback that maximises the sense of ownership within users may achieve excellent rehabilitation outcomes. Combining VR with BCI has shown very promising results.33 VR feedback can lead to a much more portable, simpler and affordable rehabilitation system that can be used at home, achieving an ultimate goal for the BCI technology.
Apart from VR, development in soft robotics may have a significant impact on the rehabilitation domain. In most of the previous BCI studies using robotic feedback, the motor movements have been typically provided by actuators with rigid links and joints that may feel unnatural or different from the typical hand movements. This may reduce the sense of ownership within the users, possibly affecting the rehabilitation gains. Therefore, the soft robotic devices which are designed to conform better to the human limbs may provide higher rehabilitation gains. One initial study has shown encouraging clinical gains following a BCI-controlled soft robotic glove-based rehabilitation.24 Collectively, FES, along with the VR and soft robotic devices appear to be the most promising feedback paradigms to explore in future BCI rehabilitation trials.
Most BCI-based motor rehabilitation studies can be observed to follow one of the two paradigms to identify MI or movement execution and to provide the corresponding feedback. The first kind of studies employ a neurofeedback-like approach wherein specific, known neuroscientific features, like power in SMR or power in ERD/ERS, are extracted to identify motor intentions of the patients and to provide appropriate feedback.23 Whereas, the second kind of studies take a data-driven approach and use algorithms like filter bank common special patterns to identify discriminatory brain activation patterns that are specific to the targeted task.24 Although multiple studies have been conducted with either of these two control strategies, the strategy that could elicit maximum clinical gains is still unknown. It has been postulated that BCIs that use known neuroscientific signatures as a rehabilitation target may reduce the stroke-induced abnormal brain activations and lead to better clinical gains. Data-driven BCI studies are motivated by findings that stroke may completely alter the brain dynamics of the patient thus invalidating the known signatures and necessitating the identification of the patient-specific brain signatures of MI or movement execution. Recent meta-analyses indicate that BCI systems based on known neuroscientific signatures as control signals may achieve better overall clinical gains.29 31 However, this conclusion needs to be further validated in controlled trials.
The inclusion of BCI in a mainstream stroke rehabilitation regime needs more understanding of the dose-response characteristics. Efforts are necessary to identify how the frequency, duration, and intensity of the BCI rehabilitation affect clinical gains. An initial study targeting this task has indicated that BCI intensity may affect the overall clinical gains.34 The impact of total BCI usage time on clinical gains is not clear. One study showed a positive association34 but the other did not.35 Furthermore, one recent study conducted on acute and patients who had a chronic stroke has indicated plateauing of clinical gains.23 In this cross-over study, patients participated in a month of standard rehabilitation and a month of BCI-mediated rehabilitation. Regardless of the rehabilitative intervention, the authors observed that the gains during the second arm of the study were significantly lower than the first one indicating a saturation in clinical gains. A similar observation was presented in a study by Ang et al.18 In this 6-week long BCI-robotic rehabilitation trial, recruiting acute and chronic stroke patients, the average clinical gains in the first, and the next 3 weeks were 5.8 FMA points and 1.8 FMA points, respectively. Although plateauing of clinical gains is evident, considering the inclusion of patients with relatively shorter time poststroke, further studies are necessary to investigate whether these observations are caused by plateauing of spontaneous recovery or intervention-induced recovery.
Lastly, compared with the upper extremity, rehabilitation of lower extremity (LE) motor impairments using BCI has been far less explored. The difficulty in LE rehabilitation using BCI primarily stems from the difficulty in decoding LE movement kinematics and kinetics parameters from the non-invasive recording methods.36 Furthermore, walking involves precise coordination of multiple muscle movements, and this translates into significant difficulty in designing appropriate feedback mechanisms for LE movements. Despite these difficulties, some initial studies have explored BCI-mediated rehabilitation for poststroke LE impairments. Chung et al reported the use of BCI-mediated LE motor function improvements in patients who had a stroke.37 In this study, patients received FES stimulation on detection of a successful ankle dorsiflexion attempt. The study reported significant clinical improvements in gait velocity and cadence. A few other studies have reported clinical improvements in lower limb motor functions38 39 and more focused efforts are necessary in this direction. These studies have exclusively used FES and visual feedback in the study design. However, moving forward, an exploration into lower-limb exoskeletons controlled using sophisticated gait decoding algorithms that can extract movement kinetic and kinematic parameters from brain signals40 is essential to achieve more natural lower limb motor rehabilitation with the BCI technology.
BCI for poststroke aphasia and cognitive rehabilitation
Aphasia and poststroke cognitive impairments are the second most common impairments following stroke. About 70% of stroke patients suffer from some degree of speech and cognitive impairments in the acute phase and 20% and 35.6% of them, would retain these impairments in the chronic phase.41 42 Within the domain of speech impairment, stroke survivors have difficulties in language understanding or synthesis or both. In addition, cognitive deficits including reduced attention, impaired long and short-term memory, deterioration in executive functions, reduced speed of information processing and degradation of semantics are present in many patients who had a chronic stroke.43
Cognitive impairments and aphasia have significant bidirectional interactions. Difficulty in language understanding has been noted to hamper the recovery of many executive cognitive functions.2 Lack of sustained attention and concentration can also significantly affect speech as well as motor rehabilitation efforts. In most interventions, including BCI-based interventions, patients are required to possess a certain degree of cognitive functions in order to comprehend and adhere to the rehabilitation paradigm. Patients with severe cognitive impairments are often excluded from these rehabilitative interventions. Therefore, focused efforts are essential towards poststroke cognitive and aphasia rehabilitation.
Speech and language therapy performed by a speech therapist, along with pharmacological interventions, has been the traditional way of treating poststroke aphasia. For improving cognitive functions, various methods are in use with the most prominent ones being cognitive-behavioural therapy, occupational therapy, pharmacotherapy, and computer-assisted cognitive rehabilitation paradigms.44 45 However, these paradigms have achieved limited success thereby necessitating the exploration of novel and more effective rehabilitation strategies.44 46
The field of BCI for poststroke cognitive and speech rehabilitation is still in its nascency and has received very limited attention from the research community. In this domain, all the studies have exclusively used the neurofeedback paradigm of BCI to realise cognitive and speech improvements. In this paradigm, patients are asked to voluntarily modulate certain abnormal brain activations with the goal of normalising them to a more healthy state by repetitive performance.2 This approach has not been explored much in stroke patients but has helped improve many cognitive functions in other brain disorders like attention deficit hyperactivity disorder,47 mild cognitive impairments48 and traumatic brain injury.49 An extensive list of BCI-mediated cognitive and speech rehabilitation studies in patients who had a stroke can be found in a recent review by Mane et al.2 Thus, from a behavioural perspective, encouraging results with neurofeedback training from patients suffering from other disorders and initial results from patients who had a stroke indicate that BCI could be a very promising technique to improve cognitive and language functions in patients who had a stroke.
Among the neuro feedback training studies, Mroczkowska et al reported improvements in the patient’s expressive speech following 10 sessions of neurofeedback training targeted to increase the beta/theta band power ratio at the C3 EEG electrode in 2014.50 In this study, the authors observed a reduction in phonemic paraphasias, increased speech fluency, faster and more accurate word retrieval, and improved understanding of syntactically complex utterances. Furthermore, in another study, neurofeedback training to increase the relative alpha power in the occipital region of the brain showed slight improvements in naming, images and colours identification, sentence completion and verbal fluency.51 These observations indicate that upregulation of brain oscillations in the high-frequency band may result in improved speech performance. The preliminary results presented in these studies need to be further validated in randomised controlled studies.
It is also essential to identify the exact brain locations for neurofeedback that might result in the most optimal gains in speech functions. A recent brain stimulation study has indicated that the contralesional inferior frontal gyrus can be one of the optimal locations to target poststroke aphasia.52 Therefore, more research along this direction may be beneficial for the advancement of aphasia rehabilitation with neurofeedback training.
In the domain of cognitive rehabilitation, instead of just one aspect, most neurofeedback studies have reported a holistic improvement in most components of cognition. Most of these studies have targeted modulation of the power spectral density in the EEG signals from either frontoparietal areas or motor and sensorimotor areas. As an example, a case study by Mroczkowska et al observed improvements in concentration, visual perception, categorising, regulation of affect and speech following neurofeedback training.50 Furthermore, cross-domain improvements in motor and cognitive domains, as well as reduced depression and anxiety were reported following the alpha band upregulation neurofeedback.51 Improvements in memory functions including declarative memory,53 long-term and short-term memory, and working memory have been reported. In all these studies, upregulation of the higher frequency oscillations including low and high alpha, low and high beta, and downregulation of delta and theta waves has been a central theme. Furthermore, a few studies have also explored the specific effects of each of these frequency bands on rehabilitation outcomes. Hofer et al observed that SMR-based neurofeedback training leads to improvements in declarative memory performance whereas theta/beta power-based neurofeedback leads to improvements in inhibition and cognitive flexibility.53 Similarly, Kober et al observed that SMR-based neurofeedback was associated with improvements in visuospatial short-term memory performance, and upper alpha upregulation was associated with improved working memory performance.54 These studies indicate that more investigation is necessary on the specific roles of these frequency bands and their benefits in the cognitive rehabilitation domain.
Collectively, the field of BCI-based poststroke aphasia and cognitive rehabilitation is at an exciting juncture and many more large, controlled studies are necessary in the near future to realise its true potential.
BCI for poststroke communication and control
Although the rehabilitative potential of the BCI system is of prominent interest in the stroke population, BCI assistive devices are also being explored to improve stroke patients’ quality of life. The patients experiencing complete tetraplegia due to diseases like amyotrophic lateral sclerosis, spinal cord injury, or severe brainstem stroke are the primary motivation behind the assistive use of BCI. These patients lack any form of muscle control and hence BCI becomes the only method that can enable communication with the external world and control of the surroundings. Most assistive devices in the stroke population have used non-invasive methods of brain signal recording such as EEG recordings. Within the EEG-BCIs, primarily three control and communication strategies have been explored; viz., P300 BCIs, steady-state evoked potential BCIs, and SMR BCIs. Also, communication with the BCI speller and control of computer cursor, wheelchair, external robotic devices and upper and lower limb exoskeletons have been some of the most explored applications of assistive BCIs.
P300 is an event-related potential observed at the midline locations of the brain in a form of a positive EEG peak 200–500 ms preceding the presentation of infrequent stimulation. This potential is observed in the brain when the person is presented with rarely occurring or unfamiliar visual stimulation. Many studies have used this neurological signature to create an application interface for the selection of a target from available options. As an example, in P300 based speller application, alphabets are presented in a grid of rows and columns with each being flashed in sequence. The subject is asked to focus on the alphabet that he/she wishes to select and P300 is observed when the row and column containing the alphabet gets flashed. Based on the observed P300, the target alphabet is identified. Operating on similar principles, the P300 paradigm has been used to control/communicate a multitude of other applications including control of a computer cursor in a two-dimensional (2D) space,55 control of a humanoid robot,56 control of a wheelchair57 and movement of the virtual hand in the VR settings.58 Moreover, a case study has reported successful communication with a P300 speller in a completely locked-in brainstem infarction patient.59 These results indicate that even patients who had a stroke could control and communicate using the P300 paradigm. High accuracy and short training time are the two most important advantages of P300-based BCIs. Moving forward, exploration of the techniques that can reduce fatigue arising due to the high level of attention and visual focus required to operate the P300 BCIs is necessary. Furthermore, exploratory studies should be performed to analyse the ability of patients with poststroke cognitive impairments to operate the P300 BCIs.
Steady-state evoked potentials, particularly, the steady-state visual evoked potential (SSVEP), is another most popular BCI-based communication paradigm. In the SSVEP paradigm, multiple targets flickering with different frequencies (1–100 Hz) are presented to the user and the user is asked to concentrate on the desired target. This concentration generates a specific frequency response in the occipital region of the brain and a strong peak in the EEG power spectrum is observed at the frequency which is correlated with the flickering frequency of the intended target. The user’s intended target is identified by correlating the observed EEG with the target’s flickering frequency. Being an exogenous stimulus, SSVEPs have been observed to achieve very high accuracies, that too, without the need for any subject training. Furthermore, simultaneous presentation of multiple targets with different flickering frequencies enables selection from many commands and significantly higher information transfer rates (100 bits/min or higher).60 Owing to the high information transfer rates and robust performance, the SSVEP paradigm has been used to control multiple applications even in the patient population including the control of a humanoid robot,61 a lower limb exoskeleton,62 and an electrical prosthesis.63 Despite the high accuracies, even SSVEP suffers from high fatigue rates and more studies, particularly in the stroke patient population, are necessary. Furthermore, some studies have explored the use of the SSVEP paradigm in VR settings and more such studies are essential.64
SMR-based BCIs that have been prominently used in motor rehabilitation studies have also been explored for control and communication applications. In particular, a few SMR-based BCIs have attempted to decode the limb movement kinetic and kinematic parameters from the brain signals which were further used to control an external robotic device, orthosis or exoskeleton. One recent study has demonstrated successful control of a 2D cursor and a three-dimensional (3D) robotic arm based on the SMR BCI paradigm.65 The SMR BCI uses endogenously generated brain activations to achieve control of the external environment. Although this results in a much more natural way of controlling the external devices, it also makes the task of detecting and decoding the SMR much more difficult. Therefore, SMR-based BCIs commonly suffer from low classification accuracies and future studies need to concentrate on techniques like deep learning66 to improve the decoding accuracies of SMR-BCI systems.
Lastly, although invasive techniques have not been very widely explored in the human population due to the high clinical risks, recent advances in sensor technologies and brain implantation methods have indicated the feasibility of invasive BCI systems in humans. BrainGate67 and Neuralink68 are among the two most prominent technological innovations, in the domain of invasive BCIs. Fine 3D robotic arm control69 and control of computer cursor67 have been already demonstrated using BrainGate implant in two completely paralysed patients. Considering the high information transfer rates offered by the invasive recording methods and continual technological improvement happening in the invasive sensor domain, invasive BCIs may receive significant attention from the research community in the future.
Future prospects and conclusions
In this manuscript, we presented a non-exhaustive, perspective review of BCI systems that can improve stroke patients’ quality of life either by augmenting or by promoting recovery of stroke-lost motor, cognitive and speech function impairments.
The field of motor rehabilitation has progressed at a tremendous pace in the last decade. The safety and efficacy of the BCI systems for motor rehabilitation, particularly upper limb motor rehabilitation, have been well established and BCI has emerged as one of the most promising technologies in this domain. In the last 5 years, the research in the motor rehabilitation domain has evolved to tackle much more complex questions with an aim to improve the clinical effectiveness of rehabilitative BCI systems. These works and their meta-analysis have hinted at solutions to some of the most long-standing questions in the field. The meta-analyses have indicated the use of FES or VR/visual feedback along with the SMR-based detection of MI signatures can provide marginally better clinical gains. Considering their paramount importance in the design of BCI systems, we think that a randomised controlled trial should be conducted in the future to provide conclusive remarks on the best choice of feedback and MI detection mechanisms. Fine-grained characterisation of dose-response characteristics is another domain that will affect the widespread adoption of BCI-based motor rehabilitation and hence significant efforts in this direction are essential in the near future. Furthermore, efforts in the direction of personalised rehabilitation whereby rehabilitation regimes can be tweaked according to the patients’ health, and lesion and neuronal profile can be the next forefront of stroke-BCI research. Lastly, the rehabilitation of LEs should receive significantly more attention in the coming 5 years.
The field of poststroke cognitive and speech rehabilitation using BCI is still in its nascency. Despite quite a few successful small-scale feasibility studies, this field is yet to gain attention from a wider research community. The understanding that bidirectional interactions exist between speech and cognitive function and cognitive functions can also impact motor restoration efforts indicates that effective rehabilitation of these functions can have cascading positive effects. Therefore, significant and immediate attention to establishing the efficacy of BCI-based cognitive rehabilitation is warranted. Furthermore, BCI-based rehabilitation of poststroke aphasia is one of the domains that has remained hidden from the purview of BCI researchers. Although many BCI-based cognitive rehabilitation studies have reported improvements in language and speech functions as a secondary outcome, no study has investigated the efficacy of the BCI system specifically designed for the purpose of aphasia rehabilitation. Hence, in light of the encouraging evidence, a serious exploration of poststroke aphasia rehabilitation using BCI is desired. Lastly, interactions between motor, cognitive, and speech impairments indicate a need for a comprehensive rehabilitation platform and BCI can be just the right fit for the realisation of such a platform. Therefore, an idea of a holistic stroke rehabilitation platform using BCI should be explored.
Finally, in the domain of assistive BCI, significant work has been done to indicate the feasibility, and practicality of BCI-based communication and real-time control. However, more exploration of these techniques in the stroke population, particularly those suffering from extremely severe paralysis and cognitive impairments is warranted.
In conclusion, BCI technology holds the potential to provide a comprehensive solution for the betterment of stroke patients’ quality of life.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors RM performed the literature review and prepared the manuscript. ZW and DW conceptualised and supervised the review and revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.