Article Text

Abstract
Background To evaluate the association between coexisting intracranial and extracranial carotid artery atherosclerotic diseases and ipsilateral acute cerebral infarct (ACI) in symptomatic patients by using magnetic resonance (MR) vessel wall imaging.
Methods Symptomatic patients were recruited from a cross-sectional, multicentre study of Chinese Atherosclerosis Risk Evaluation (CARE-II). All patients underwent MR imaging for extracranial carotid arterial wall, intracranial artery and brain. Coexisting intracranial stenosis ≥50% and extracranial carotid artery mean wall thickness (MWT) ≥1 mm and plaque compositions at the same side were evaluated and the ipsilateral ACI was identified. The association between coexisting atherosclerotic diseases and ACI was evaluated using logistic regression.
Results 351 patients were recruited. Patients with ipsilateral ACI had significantly greater prevalence of coexisting intracranial stenosis ≥50% and carotid MWT ≥1 mm (20.5% vs 4.9%, p<0.001), calcification (15.1% vs 4.4%, p=0.001) and lipid-rich necrotic core (LRNC) (19.2% vs 7.8%, p=0.002) compared with those without. Coexisting intracranial artery stenosis ≥50% and carotid MWT ≥1 mm (OR 5.043, 95% CI 2.378 to 10.694; p<0.001), calcification (OR 3.864, 95% CI 1.723 to 8.664; p=0.001) and LRNC (OR 2.803, 95% CI 1.455 to 5.401; p=0.002) were significantly associated with ipsilateral ACI. After adjusting for confounding factors, the aforementioned associations remained statistically significant (intracranial stenosis ≥50% coexisting with carotid MWT ≥1 mm: OR 4.313, 95% CI 1.937 to 9.601, p<0.001; calcification: OR 3.606, 95% CI 1.513 to 8.593, p=0.004; LRNC: OR 2.358, 95% CI 1.166 to 4.769, p=0.017).
Conclusions Coexistence of intracranial artery severe stenosis and extracranial carotid artery large burden and intraplaque components of calcification and LRNC are independently associated with ipsilateral ACI.
Trial registration number https://www.clinicaltrials.gov/. Unique identifier: NCT02017756.
- atherosclerosis
- stroke
- MRI
- vessel wall
Data availability statement
The datasets generated and/or analysed during the current study are not publicly available due to them containing information that could compromise research participant privacy/consent, but are available from the corresponding author (XZ) on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
It has been shown that atherosclerosis occurring in intracranial artery and extracranial carotid arteries is the major cause of ischaemic stroke. A number of studies demonstrated that intracranial artery atherosclerotic stenosis1–3 and carotid vulnerable plaques4–8 are separately associated with cerebrovascular events. As a systemic disease, however, atherosclerosis frequently involves multiple vascular beds and coexisting plaques in both intracranial and extracranial arteries are prevalent in symptomatic patients.3 9–11 Coexisting plaques in multiple vascular beds reflect the systemic burden of atherosclerotic disease and increasing evidences showed that multivascular coexisting plaques had higher risk of developing ischaemic events compared with single vascular atherosclerosis.12 13 The coexisting intracranial and extracranial carotid plaques are special clinical status; this status is different from patients with plaques either in intracranial artery alone or extracranial carotid artery alone. Patients with coexisting intracranial artery and extracranial carotid artery plaques may share similar risk factors with those who had plaques either in intracranial artery alone or extracranial carotid artery alone. However, patients with coexisting plaques in multiple vascular beds may have a special clinical profile. We assumed that the coexisting plaques may have independent relationship with ischaemic stroke. Previous studies have shown that coexisting intracranial and extracranial carotid plaques were associated with recurrent stroke,10 12 but those studies had either smaller sample size or the ischaemic lesions were not in the ipsilateral side with coexisting plaques which does not facilitate investigating the causal relationship between cerebrovascular coexisting atherosclerotic diseases and downstream cerebral ischaemia.
Magnetic resonance (MR) vessel wall imaging has been widely used to evaluate the vulnerability of carotid atherosclerotic plaques by measuring plaque burden and characterising plaque compositions, such as calcification, lipid-rich necrotic core (LRNC) and intraplaque haemorrhage (IPH).14 15 MR vessel wall imaging can directly depict the pathology of arterial wall with atherosclerosis and this technique is superior to angiographic approaches because angiography can only provide luminal narrowing information. This study aimed to investigate the relationship between coexisting intracranial stenosis and extracranial artery vulnerable plaque features at the same side determined by MR vessel wall imaging and the ipsilateral acute cerebrovascular events.
Methods
Study sample
Patients were recruited from a cross-sectional, multicentre study of Chinese Atherosclerosis Risk Evaluation (CARE-II) The design and rationale of the CARE-II study have been published.16 In brief, the objective of the CARE-II study was to determine the prevalence of high-risk plaques (HRPs) in carotid arteries of symptomatic patients. The inclusion criteria are (1) 18–80 years old, (2) recent transient ischaemic attack (TIA) or ischaemic stroke (within 14 days), and (3) atherosclerotic plaque in at least any side carotid artery determined by ultrasound imaging (intima–media thickness ≥1.5 mm). The exclusion criteria include (1) cardioembolic stroke, (2) haemorrhagic stroke, (3) radiation therapy in the neck, (4) claustrophobia and (5) contraindications to MR examination. For this study, only those patients with complete MR imaging for bilateral carotid arteries, intracranial arteries and brain in CARE-II were enrolled. The clinical data including gender, age, hypertension, body mass index (BMI), hyperlipidemia, smoking, diabetes mellitus, coronary heart disease, anti-hypertensive agent, statin therapy and the levels for blood pressure (systolic blood pressure (SBP) and diastolic blood pressure (DBP)) and lipoproteins (high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglycerides (TG) and total cholesterol (TC)) were collected from the medical record.
MR imaging
The MR imaging was conducted on 3.0 T MR scanners (Achieva TX; Philips Healthcare, Best, The Netherlands) with dedicated eight-channel carotid coils and head coils. The vessel wall of extracranial carotid arteries was imaged with multi-contrast imaging protocol including the three-dimensional (3D) time-of-flight (TOF), T1-weighted (T1W), T2-weighted (T2W) and magnetisation prepared rapid gradient echo (MP-RAGE) sequences. Intracranial artery and brain were imaged using routine imaging protocol including 3D TOF, T1W, T2-fluid attenuated inversion recovery and diffusion-weighted imaging (DWI) sequences. The imaging parameters have been published.16
Image analysis
Before the MR images were reviewed, identifiable information such as patient name, age, examination data, examination ID and subject ID were anonymised. The carotid MR images were interpreted before brain image review by two trained reviewers (XZ, CJ) with more than 3 years’ experience in neuroimaging obeyed the previous standards16 with consensus blinded to clinical information and MR imaging data of intracranial artery and brain. The MR images of index carotid artery were reviewed by using customdesigned software (CASCADE; University of Washington, Seattle, USA). The index carotid artery was defined as carotid artery responsible for the recent cerebrovascular symptoms or the more severe wall thickness bilaterally in patients without confirmed side of symptoms. The image quality of carotid arteries was rated with a 4-point scale: 1, poor; 2, marginal; 3, good; 4, excellent. The carotid images with image quality <2 were excluded. The mean wall thickness (MWT) of the index carotid arteries was measured. The presence of plaque compositions in index carotid arteries, such as calcification, LRNC and IPH, was determined using published criteria.17 18 The percentage of LRNC occupying vessel wall was calculated. The fibrous cap rupture (FCR) and HRP were also evaluated. The HRP was determined when plaques had IPH, FCR or large LRNC (percentage of LRNC occupying vessel wall >40%). The luminal stenosis of index carotid arteries was measured on the maximum intensity projection of 3D TOF images using North American Symptomatic Carotid Endarterectomy Trial (NASCET) criterion.19
The luminal stenosis of intracranial arteries in anterior circulation, including the M1 segment of middle cerebral artery and A1 segment of anterior cerebral artery at the ipsilateral side of index carotid artery, was measured using WASID (Warfarin-Aspirin Symptomatic Intracranial Disease) criterion20 by two radiologists (XW and JZ) who had >3 years’ experience in neuroimaging blinded to clinical information and carotid and brain imaging data with consensus. When multiple stenoses were present in intracranial arteries, the most severe lesion was selected for statistical analysis. Luminal stenosis ≥50% was considered as severe stenosis. Acute cerebral infarct (ACI) in the anterior circulation territories at the same side of the index carotid artery was identified on the diffusion-weighted images by a neuroradiologist (CJ, the same reviewer who interpreted the carotid MR image) blinded to clinical information and carotid and intracranial artery imaging data.
The presence of coexisting intracranial and extracranial atherosclerotic disease was identified which is defined as presence of both intracranial severe stenosis and MWT ≥1 mm or any plaque component or HRP in index carotid arteries at the same side.
Statistical analysis
The continuous variables were presented as mean value and SD. The binary variables were described as percentage. The clinical characteristics and index extracranial carotid artery and intracranial artery measurements of atherosclerosis were compared between patients with and without ipsilateral ACI using Mann-Whitney U test or χ2 test. Univariate and multivariate logistic regressions were used to calculate the OR and the corresponding 95% CI of coexisting intracranial and extracranial atherosclerotic diseases in discriminating presence of ipsilateral ACI at anterior circulation territories before and after adjusting for clinical confounding factors. Confounding factors were determined when their p values <0.1 during comparison between patients with and without ACI. The p value <0.05 was considered as statistically significant. All statistical analyses were conducted using SPSS V.20.0.
Results
Of the total 1047 patients from the CARE-II study, 351 patients were enrolled in this study. Six hundred ninety-six patients were excluded due to the following reasons: (1) no intracranial artery MR imaging data (n=477); (2) no brain diffusion-weighted imaging data (n=22); (3) no complete clinical data (n=189); (4) poor imaging quality (n=8). The flow chart of patient recruitment is presented in figure 1. Of the remaining 351 patients, 234 had a confirmed carotid artery which was responsible for the recent cerebrovascular symptoms, and 117 had non-confirmed side of symptoms and the index carotid artery was defined the more severe wall thickness in bilaterally carotid arteries in those patients. In the 351 patients, the mean age was 62.5±9.6 years old, 228 (65.0%) were men, 256 (72.9%) had hypertension, 191 (54.4%) had hyperlipidemia, 159 (45.3%) had history of smoking, 110 (31.3%) had diabetes and 54 (15.4%) had a history of coronary heart disease, respectively. Of all remaining 351 patients, 214 (61.0%) and 135 (38.5%) had taken anti-hypertension and statin agents, respectively. The clinical characteristics of this study population are detailed in table 1.
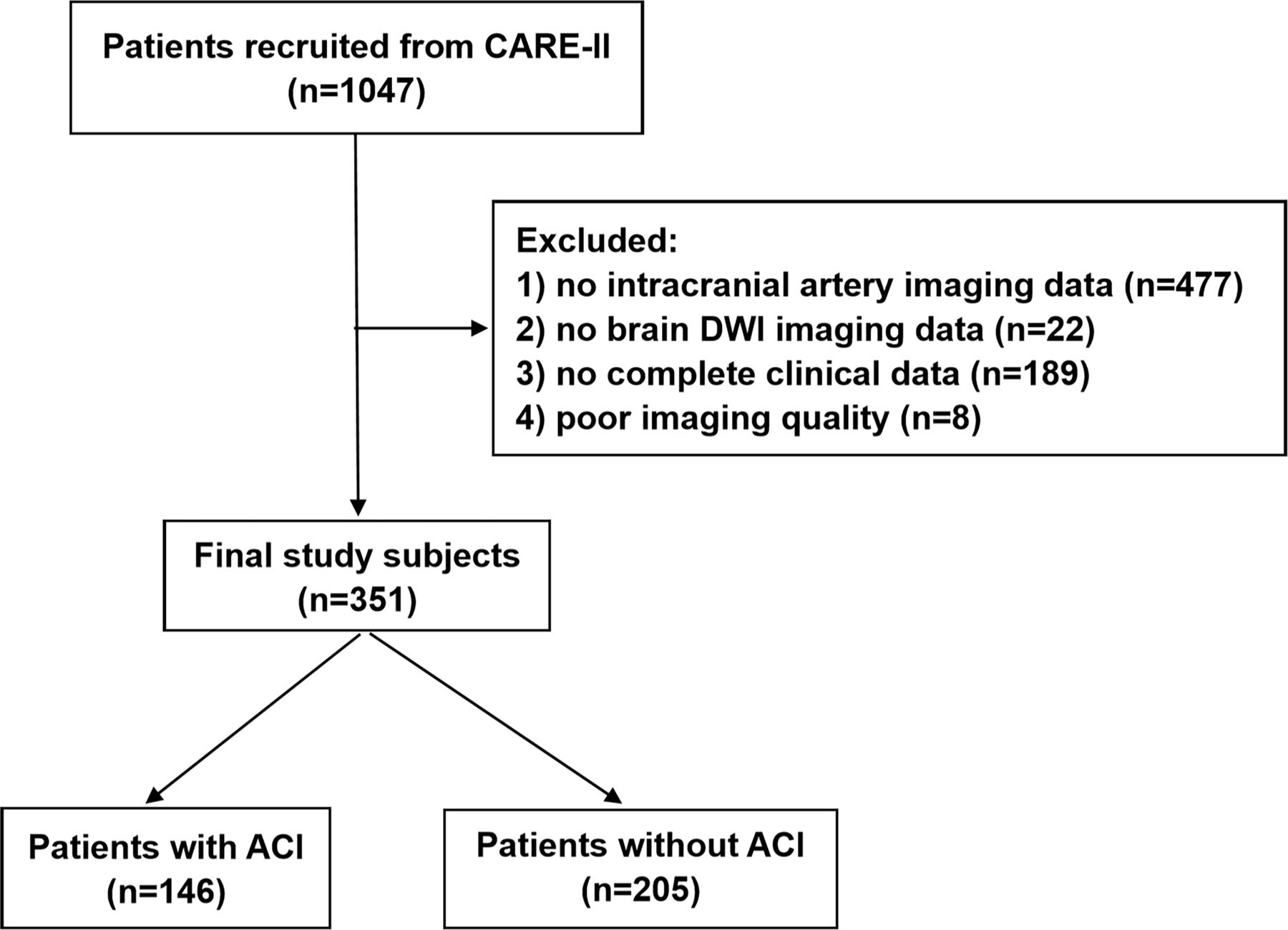
Flow chart of patient recruitment. ACI, acute cerebral infarct; DWI, diffusion-weighted imaging.
Clinical characteristics of study population (n=351)
Comparison of clinical characteristics between patients with and without ACI
Patients with ACI are more likely male (73.3% vs 59.0%, p=0.006) and had significantly higher prevalence of history of smoking (52.1% vs 40.5%, p=0.032) and diabetes (41.8% vs 23.9%, p<0.001) than those without ACI. Patients with ACI were significantly younger than those without ACI (61.2±9.2 years old vs 63.5±9.8 years old, p=0.047). The levels of DBP (90.0±15.6 mmHg vs 85.3±11.6 mmHg, p=0.020) and BMI (25.0±3.3 kg/m2 vs 23.8±3.2 kg/m2, p=0.001) in patients with ACI were significantly higher than those in patients without. Patients with ACI had significantly lower HDL (1.1±0.5 mmol/L vs 1.2±0.4 mmol/L, p=0.011) compared with those without ACI. No significant differences were found in other clinical characteristics between the two patient groups (all p>0.05, table 1).
Coexisting intracranial and extracranial carotid atherosclerotic diseases
Of 351 patients, the prevalence of coexisting intracranial stenosis ≥50% and carotid stenosis ≥50%, carotid MWT ≥1 mm, carotid calcification, carotid LRNC, carotid IPH, carotid FCR and carotid HRP was 3.4%, 11.4%, 8.8%, 12.5%, 2.0%, 0.9% and 2.8%, respectively. Compared with patients without ipsilateral ACI, those with ipsilateral ACI had significantly greater prevalence of coexisting intracranial stenosis ≥50% and carotid MWT ≥1 mm (20.5% vs 4.9%, p<0.001), coexisting intracranial stenosis ≥50% and carotid calcification (15.1% vs 4.4%, p=0.001), and coexisting intracranial stenosis ≥50% and carotid LRNC (19.2% vs 7.8%, p=0.002) (table 2). No significant differences were found in other coexisting intracranial and extracranial atherosclerotic diseases between patients with and without ipsilateral ACI (all p>0.05, table 2).
Coexisting intracranial and extracranial carotid atherosclerotic diseases
Association between intracranial artery or carotid artery atherosclerotic diseases and ipsilateral ACI
In discriminating presence of ipsilateral ACI, the OR values of intracranial artery stenosis ≥50%, carotid stenosis ≥50% and carotid MWT ≥1 mm was 3.090 (95% CI 1.757 to 5.432; p<0.001), 2.799 (95% CI 1.297 to 6.041; p=0.009) and 2.684 (95% CI 1.716 to 4.199; p<0.001) before adjusting for clinical confounding factors, respectively. After adjusting for clinical confounding factors, including age, gender, BMI, hypertension, DBP, smoking, HDL, TC and diabetes, intracranial artery stenosis ≥50% (OR 3.009; 95% CI 1.637 to 5.531; p<0.001), carotid stenosis ≥50% (OR 2.561; 95% CI 1.116 to 5.878; p=0.026) and carotid MWT ≥1 mm (OR 2.495; 95% CI 1.521 to 4.093; p<0.001) were still significantly associated with ipsilateral ACI. No significant associations were found between other carotid plaque features and ipsilateral ACI before and after adjusting for confounding factors (all p>0.05, table 3).
Association between intracranial artery or carotid artery atherosclerotic diseases and ipsilateral ACI
Association between coexisting atherosclerotic diseases and ipsilateral ACI
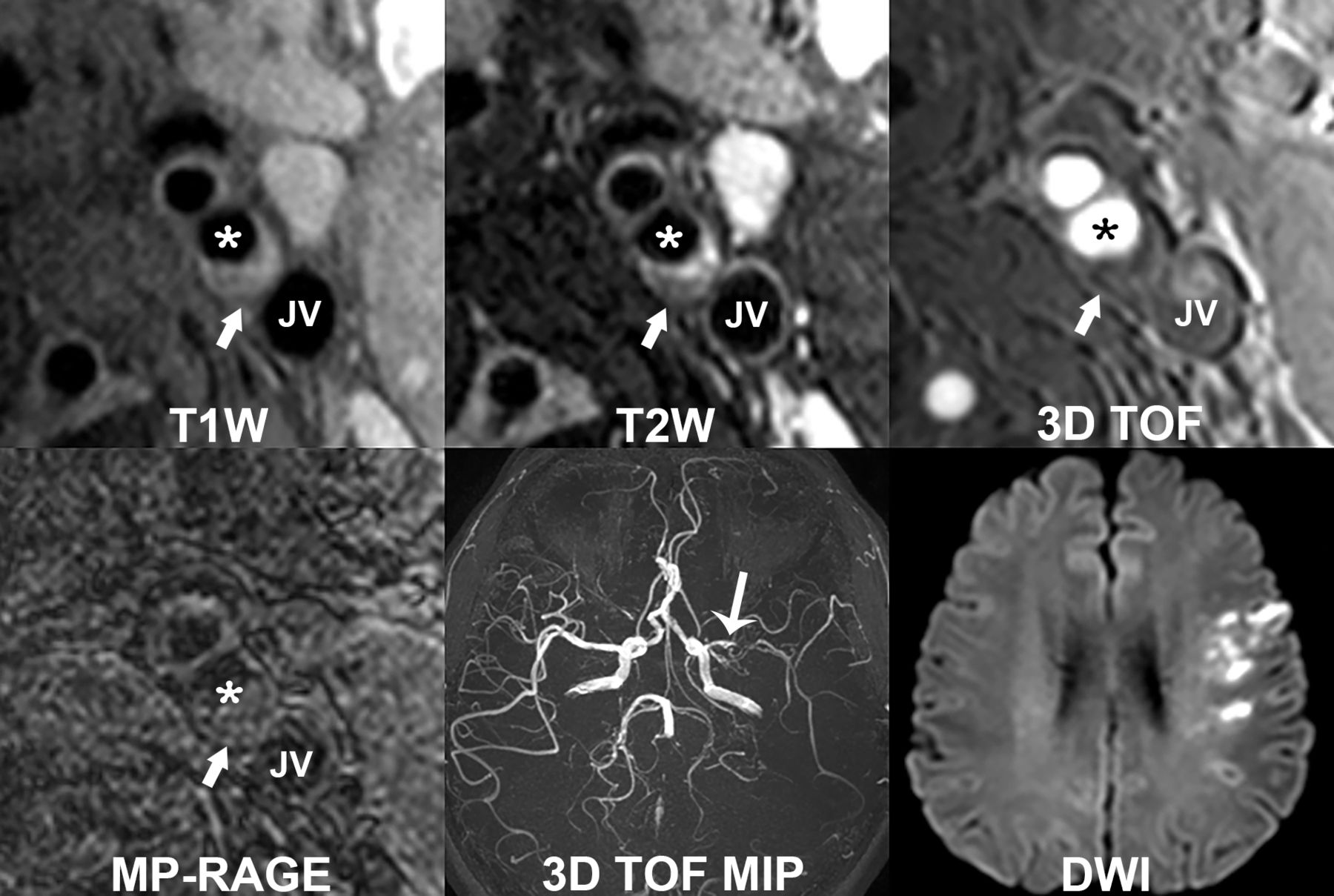
In discriminating presence of ipsilateral ACI, the OR value of coexisting intracranial artery stenosis ≥50% and carotid MWT ≥1 mm, coexisting intracranial artery stenosis ≥50% and carotid calcification, and coexisting intracranial artery stenosis ≥50% and carotid LRNC was 5.043 (95% CI 2.378 to 10.694; p<0.001), 3.864 (95% CI 1.723 to 8.664; p=0.001) and 2.803 (95% CI 1.455 to 5.401; p=0.002) before adjusting for clinical confounding factors, respectively. After adjusting for clinical confounding factors, including age, gender, BMI, hypertension, DBP, smoking, HDL, TC and diabetes, coexisting intracranial artery stenosis ≥50% and carotid MWT ≥1 mm (OR 4.313; 95% CI 1.937 to 9.601; p<0.001), coexisting intracranial artery stenosis ≥50% and carotid calcification (OR 3.606; 95% CI 1.513 to 8.593; p=0.004), and coexisting intracranial artery stenosis ≥50% and carotid LRNC (OR 2.358; 95% CI 1.166 to 4.769; p=0.017) were still significantly associated with ipsilateral ACI. No significant associations were found between coexisting intracranial artery stenosis ≥50% and other carotid plaque features and ipsilateral ACI before and after adjusting for confounding factors (all p>0.05, table 4). Figure 2 is an example showing a patient with ipsilateral coexisting intracranial artery stenosis ≥50% and carotid LRNC and ipsilateral ACI.
Association between coexisting atherosclerotic diseases and ipsilateral ACI

{kind=link}
{kind=link}
Coexisting intracranial artery stenosis ≥50% and carotid lipid-rich necrotic core with ipsilateral acute cerebral infarct. A patient who has eccentric atherosclerotic plaque with lipid-rich necrotic core (white arrow) in the left internal carotid artery (star). The lipid-rich necrotic core appeared iso-intense on T1W and TOF images and hypointense on T2W image. Severe luminal stenosis (stenosis ≥50%) in the left middle cerebral artery was found on 3D TOF MRA (MIP, maximum intensity projection) (white arrow). Multiple acute infarct lesions in left anterior circulation territory were observed on diffusion-weighted image. JV, jugular vein.
Discussion
The present study used MR imaging to investigate the association between coexisting intracranial and extracranial carotid atherosclerotic diseases and ipsilateral ACI in the Chinese population. We found that patients with ACI had significantly higher prevalence of coexisting intracranial stenosis ≥50% and carotid MWT ≥1 mm, carotid calcification and carotid LRNC than those without. Logistic regression analysis revealed that coexisting intracranial and extracranial carotid atherosclerotic diseases were independently associated with ipsilateral ACI. Our findings indicate that individuals with coexisting intracranial and extracranial artery atherosclerotic diseases may have higher risk of developing cerebrovascular events.
We found that a substantial number of symptomatic patients had coexisting intracranial and extracranial carotid artery atherosclerotic diseases, and these diseases were more prevalent in those with ipsilateral ACI. The high prevalence of coexisting intracranial and extracranial artery atherosclerotic diseases in symptomatic patients has been reported in previous studies. Angiographic studies showed that around 18% of symptomatic patients had coexisting intracranial and extracranial carotid stenosis.21 22 However, the prevalence of coexisting atherosclerotic diseases was found to be higher (from 32.7% to 77.6%) when vessel wall imaging was used in recent studies.10 12 13 23 The increase of such prevalence is expected because vessel wall imaging can detect atherosclerotic plaques with normal lumen size or mild stenosis which may not be depicted by traditional angiographic approaches. In the present study, we defined coexisting atherosclerotic diseases as lesions with high-risk plaque features of ≥50% stenosis intracranial artery and either large burden (MWT ≥1 mm) or presence of calcification or LRNC in extracranial carotid arteries at the same side. Our definition introduced high-risk plaque features which may enhance the predictive value of coexisting plaques for cerebrovascular events because a large number of studies demonstrated that carotid plaques with high-risk features are significantly associated with ischaemic stroke. In the present study, we considered the atherosclerotic plaques at the same side of intracranial and extracranial arteries as coexisting diseases. This consideration will be more reasonable when determining the predictive value of coexisting atherosclerotic diseases of upstream vascular beds at the same side for the ipsilateral cerebral infarction. In addition, most of the previous studies were from a single centre. In contrast, our study recruited patients from 13 clinical sites across China. Our findings suggest that both vascular beds of intracranial artery and extracranial carotid artery need to be examined when assessing atherosclerosis.
In our study, we found that coexisting intracranial stenosis ≥50% and carotid MWT ≥1 mm were significantly associated with ipsilateral ACI. It is well established that intracranial stenosis ≥50% is associated with ischaemic stroke. Carotid MWT is an important measurement for carotid plaque burden and the higher value of MWT may reflect the consequences of past exposure to risk factors. Previous studies have shown that atherosclerosis with larger MWT will be more vulnerable due to the positive relationship between MWT and the presence of IPH (OR 1.59; 95% CI 1.37 to 1.84; p<0.001) and surface disruption (OR 1.96; 95% CI 1.56 to 2.48; p<0.001).24 The wall thickness of carotid arteries was also found to be an effective indicator for cerebral events. A recent cross-sectional multicentre study of CARE-II that enrolled 687 patients who had carotid plaque demonstrated that carotid plaque burden of MWT was associated with the ipsilateral ACI (OR 1.315; 95% CI 1.103 to 1.568; p=0.002).25 In a prospective study by Takaya et al, carotid maximum wall thickness was found to be significantly associated with subsequent ipsilateral vascular events (OR 1.6; 95% CI 1.1 to 2.3; p=0.008).5 Another prospective study26 that enrolled 698 patients reported that the carotid MWT measured by MRI had predictive value for future stroke (HR 1.59; 95% CI 1.22 to 2.08). The coexisting intracranial and extracranial artery atherosclerotic diseases probably reflect a more advanced period of atherosclerotic disease,27 especially for the coexisting atherosclerosis with greater burden.
Our data showed that coexisting intracranial stenosis ≥50% and carotid calcification were independently associated with ipsilateral ACI. Although the role of calcification in plaque vulnerability is contradictory, increasing evidences have shown that the type, quantity and location of intraplaque calcifications play an important role in plaque vulnerability. Investigators found that, in the carotid artery, irregular superficial calcification was found to be more commonly accompanied with IPH as compared with the patchy type (73.8 vs 22.9%, p<0.0001), and marginal calcification showed a higher risk for the calcification accompanied with IPH as compared with the central type (72.9 vs 46.7%, p<0.05).28 A study by Lin et al reported that multiple calcifications (OR 10.1; 95% CI 3.3 to 30.4; p<0.001) and surface calcification (OR 29.4; 95% CI 4.1 to 210.8; p<0.001) were strongly associated with the presence of IPH.29 A recent basic study demonstrated that macrocalcification in carotid lesions correlated with a transcriptional profile typical for stable plaques.30 As a marker of systemic atherosclerotic disease, calcification is closely related to stroke. A study by Zhang et al revealed that spotty calcification at bilateral carotid bifurcation was significantly associated with stroke (OR 2.49; 95% CI 1.55 to 4.00; p<0.001).31 A Rotterdam study that recruited 2521 subjects showed that carotid artery calcification was independently associated with history of stroke (OR quartile 4 vs 1: 5.0; 95% CI 2.2 to 11.0; p<0.001).32 Since carotid calcification may indicate the probability of having advanced plaque, it can be expected that its coexistence with intracranial stenosis ≥50% will increase the risk of developing cerebrovascular events.
In the present study, the coexisting intracranial stenosis ≥50% and carotid LRNC were also found to be significantly associated with ipsilateral ACI. The LRNC is an important compositional feature of vulnerable plaque, particularly when LRNC >40% of wall area.33 34 A meta-analysis by Gupta et al 35 demonstrated that the presence of carotid plaques with LRNC was significantly associated with ipsilateral ischaemic events and the HR was 3.00 (95% CI 1.51 to 5.95; p=0.002). In addition, investigators found that the size of carotid LRNC was associated with the severity of acute cerebral infarction.36 Coexisting intracranial stenosis ≥50% and carotid LRNC may represent the presence of vulnerable plaques occurring in both intracranial artery and extracranial carotid artery. A most recent study by Li et al showed that coexisting intracranial stenosis and extracranial carotid LRNC were significantly correlated with future vascular events (HR 8.12; 95% CI 2.41 to 27.31; p=0.001),12 but these coexisting plaques were not necessary in the same side. In our study, the coexisting plaques were at the same side. Our findings suggest that coexisting plaques which were at the same side may further aggravate the atherosclerotic disease burden and risk of plaque rupture upstream of the ipsilateral hemisphere and increase its risk of ischaemic events. Our findings indicate that, in evaluating the risk of ischaemic stroke, neurovascular intraplaque components such as lipid-rich necrotic core are warranted to be characterised instead of determining stenosis or presence of plaque alone.
Several limitations need to be acknowledged. First, intracranial artery atherosclerosis was evaluated by 3D TOF MRA which cannot depict the vessel wall characteristics and may yield underestimation of atherosclerotic plaques. Recently, high-resolution MR vessel wall imaging has been successfully used to assess intracranial atherosclerosis. Future studies will perform vessel wall imaging for intracranial artery in determining coexisting intracranial and extracranial atherosclerotic diseases. Second, the intracranial segment of internal carotid artery was not evaluated due to the insufficient coverage or image quality in some cases. The TOF MRA image quality of intracranial segments of carotid artery, particularly siphon, will be decreased when there is calcification in the vessel wall or artefacts arising from sphenoid sinuses, the bony structures around this segment and intravoxel dephasing. Finally, this is a cross-sectional study lacking longitudinal data and the predictive value of coexisting plaques for future events could not be determined.
Conclusions
Coexistence of intracranial artery severe stenosis and extracranial carotid large burden and intraplaque components of calcification and LRNC are independently associated with ipsilateral ACI. Our findings suggest that patients with coexisting plaques, especially those with high-risk features, may have a higher risk of cerebrovascular events. Our study provides new insights in the target of medical intervention and prevention of stroke.
Data availability statement
The datasets generated and/or analysed during the current study are not publicly available due to them containing information that could compromise research participant privacy/consent, but are available from the corresponding author (XZ) on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the institutional review board of Tsinghua University School of Medicine. The number was 20110017.
Acknowledgments
We thank all participants of the CARE-II for their contributions to the patients’ recruitment.
References
Footnotes
CJ and JZ are joint first authors.
CJ and JZ contributed equally.
ZW and XZ contributed equally.
Contributors CJ and XZ interpreted the MR image and performed data analyses and wrote the manuscript. JingZ recruited patients and performed MR scan. JianZ and XW analysed MR image and provided technical support. ZW contributed substantially to the interpretation and technical assistance. XZ conceived and interpreted the study and revised the draft of the article. CY supervised this study.
Funding This study is funded by the grants of National Key R&D Program of China (No. 2017YFC1307900, 2017YFC1307904), National Natural Science Foundation of China (81771825), and Beijing Municipal Science and Technology Commission (D171100003017003).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.