Article Text

Abstract
Antiplatelet therapy is one of the mainstays for secondary stroke prevention. This narrative review aimed to highlight the current evidence and recommendations of antiplatelet therapy for stroke prevention.
We conducted advanced literature search for antiplatelet therapy. Landmark studies and randomised controlled trials evaluating antiplatelet therapy for secondary stroke prevention are reviewed. Results from Cochrane systematic review, pooled data analysis and meta-analysis are discussed.
Single-antiplatelet therapy (SAPT) with aspirin, aspirin/extended-release dipyridamole or clopidogrel reduces the risk of recurrent ischaemic stroke in patients with non-cardioembolic ischaemic stroke or transient ischaemic attack (TIA). Dual-antiplatelet therapy (DAPT) with aspirin and clopidogrel or ticagrelor for 21–30 days is more effective than SAPT in patients with minor acute noncardioembolic ischaemic stroke or high-risk TIA. Prolonged use of DAPT is associated with higher risk of haemorrhage without reduction in stroke recurrence than SAPT. Compared with placebo, aspirin reduces the relative risk of recurrent stroke by approximately 22%. Aspirin/dipyridamole and cilostazol are superior to aspirin but associated with significant side effects. Cilostazol or ticagrelor might be more effective than aspirin or clopidogrel in patients with intracranial stenosis.
SAPT is indicated for secondary stroke prevention in patients with non-cardioembolic ischaemic stroke or TIA. DAPT with aspirin and clopidogrel or ticagrelor for 21–30 days followed by SAPT is recommended for patients with minor acute noncardioembolic stroke or high-risk TIA. Selection of appropriate antiplatelet therapy should also be based on compliance, drug tolerance or resistance.
- Atherosclerosis
- Cerebral Infarction
- Stroke
- Asprin
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
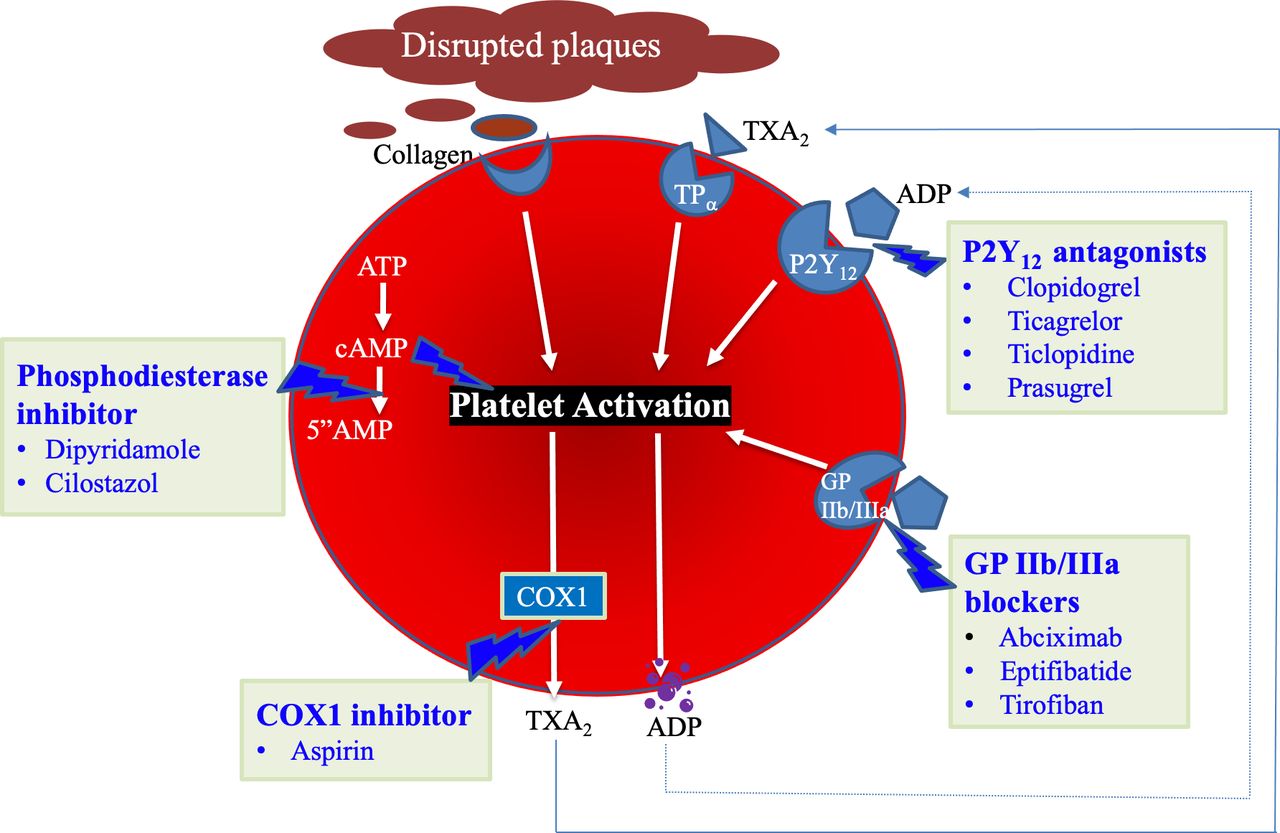
Stroke is the second-leading cause of death and the third-leading cause of death and disability combined in 2019 globally.1 Platelets are activated by collagen, ADP and arachnoid acid metabolite thromboxane A2. Activated platelets induce platelet aggregation and blood clot formation, resulting in acute ischaemic stroke (AIS) or transient ischaemic attack (TIA). Antiplatelet agents inhibit platelet aggregation and reduce the risk of AIS or TIA.2 Aspirin, clopidogrel, dipyridamole/aspirin, cilostazol and ticagrelor are commonly used antiplatelet agents. In recent years, numerous randomised controlled trials (RCTs), Cochrane systematic reviews and meta-analyses evaluated the efficacy and safety of antiplatelet therapy for secondary stroke prevention.3–9 Due to the complexity of stroke aetiology and diverse mechanisms of antiplatelet agents (figure 1), it is essential to select optimal antiplatelet therapy in the real-world practice. In this narrative review, we aimed to highlight current evidence and recommendations of the antiplatelet therapy for secondary stroke prevention.2–10

{kind=link}
The mechanisms of antiplatelet agents. Aspirin irreversibly inhibits cyclooxygenase 1 (COX1) activity. Clopidogrel and ticagrelor blocks ADP receptor. Dipyridamole and cilostazol inhibits phosphodiesterase, thereby increasing cAMP levels and preventing platelet activation. ADP, adenosine diphosphate; COX, cyclooxygenase; GP, glycoprotein; TXA2, thromboxane A2.
Methods and materials
We conducted a literature search of peer-reviewed English language articles in PubMed and Cochrane Library using the following keywords: antiplatelet therapy AND stroke, antiplatelet therapy AND ischaemic stroke, antiplatelet therapy AND transient ischaemic attack, antiplatelet agent AND stroke, antiplatelet agent AND ischaemic stroke, antiplatelet agent AND transient ischaemic attack. The search was performed for studies published between 1 January 1980 and 15 November 2021. Landmark studies, RCTs, Cochrane systematic review, pooled data analysis and meta-analysis were included for discussion.
Results
Single-antiplatelet therapy
Aspirin
Aspirin irreversibly inactivates cyclooxygenase 1 (COX1) and inhibits platelet aggregation. In 1994, the Antiplatelet Trialists’ Collaboration study evaluated 145 RCTs regarding aspirin in preventing ischaemic stroke, myocardial infarct or vascular death.11 Aspirin treatment was associated with a 22% relative risk reduction of vascular event in patients with history of AIS or TIA.
Table 1 lists the key RCTs of antiplatelet agents for stroke prevention. The International Stroke Trial (IST) randomised patients to aspirin 300 mg daily, subcutaneous heparin, both or neither within 48 hours of ischaemic stroke for up to 2 weeks.12 The aspirin group had significantly fewer recurrent ischaemic stroke (2.8% vs 3.9%, p<0.001) but equal rates of haemorrhage. The Chinese Acute Stroke Trial was similar in design except for a different aspirin dose (160 mg daily) and duration (4 weeks).13 There were significantly lower absolute risk of recurrent ischaemic stroke in the aspirin group (1.6% vs 2.1%, p=0.01). In a Cochrane systematic review of 8 RCTs with 41 483 participants on oral antiplatelet therapy for stroke prevention, aspirin 160–300 mg daily, started within 48 hours of stroke onset, reduced the risk of early recurrent ischaemic stroke without significant risk of haemorrhagic complications.5
Landmark randomised controlled trials evaluating antiplatelet therapy in secondary stroke prevention
Dipyridamole and aspirin/dipyridamole
Dipyridamole inhibits phosphodiesterase and platelet activation.14 European Stroke Prevention Study (ESPS) randomised patients with either stroke or TIA within 3 months to receive aspirin/dipyridamole (325 mg/75 mg) or placebo three times a day.15 The treatment group was associated with 33% relative risk reduction in stroke and death. ESPS-2 randomised patients with TIA or ischaemic stroke within 3 months to either aspirin 25 mg two times a day, dipyridamole 200 mg two times a day, aspirin/dipyridamole or placebo.16 Compared with placebo, relative stroke risk was significantly reduced by 18%, 16% and 37%, respectively, suggesting a synergistic effect from combination therapy.
There was no significant difference in risk of bleeding between aspirin and combination therapy group.
The main side effects of dipyridamole were headache and diarrhoea.
European Stroke Prevention in Reversible Ischaemia Trial randomised patients with TIA or minor stroke within 6 months to either aspirin/dipyridamole or aspirin.17 The dose of aspirin ranged from 30 to 325 mg, with majority receiving 30 mg daily. Aspirin/dipyridamole therapy was associated with an absolute risk reduction of 1% per year, corresponding to a number needed to treat of 104 to prevent 1 stroke, death or myocardial infarction. Of note, 34% of patients discontinued aspirin/dipyridamole due to side effects, mostly headache.
The Prevention Regimen for Effectively Avoiding Second Strokes trial randomised patients to either aspirin/dipyridamole or clopidogrel.18 At a mean 2.5 years follow-up, there was no significant difference in recurrent stroke (9% vs 8.8%) between the two groups.
Aspirin/dipyridamole has been rarely used due to high cost and significant side effect.
Cilostazol
Cilostazol also inhibits phosphodiesterase and platelet aggregation.19 CSPS randomised patients with recent stroke to cilostazol 100 mg two times daily or placebo.19 Cilostazol was associated with a relative stroke risk reduction by 41.7% (p=0.015). In CSPS-2 trial,20 2757 patients were randomised to receive cilostazol 100 mg two times daily (n=1379) or aspirin 81 mg daily (n=1378). At mean 29-month follow-up, cilostazol group had a 34% relative risk reduction in cerebral infarction than aspirin group (2.76% vs 3.71%, p=0.0357) and lower haemorrhagic events (0.77% vs 1.78%; p=0.0004).
CSPS.com (CSPS for antiplatelet Combination) evaluated the efficacy of cilostazol and either aspirin or clopidogrel versus either aspirin or clopidogrel monotherapy.21 Patients with ischaemic stroke within the previous 6 months were eligible for enrolment if at least two vascular risk factors were present and at least 50% stenosis of either an extracranial or intracranial artery. Dual-antiplatelet therapy (DAPT) was found to be superior to single-antiplatelet therapy (SAPT) in annual rate of ischaemic stroke (2.2% vs 4.5%, p=0.001). There was no significant difference in life-threatening bleeding between the two group. In a systemic review and meta-analysis of RCTs,22 cilostazol was shown to have lower rates of recurrent ischaemic stroke, haemorrhages or deaths, but higher rates of headache, palpitations and discontinuation than placebo, aspirin or clopidogrel.
Of note, essentially all clinical trials on cilostazol were conducted in Asia and results have not been replicated in other ethnic populations.22
Ticlopidine
Ticlopidine was the first developed ADP receptor (P2Y12) antagonist.23 However, due to serious adverse effects, including hepatotoxicity and bone marrow suppression, it is not used in clinical practice.
Clopidogrel
Clopidogrel is a thienopyridine that blocks ADP receptor P2Y12 and interferes with platelet cross-linking and aggregation.23 The Clopidogrel vs Aspirin in Patients at Risk of Ischaemic Events trial randomised patients with stroke, myocardial infarction or peripheral vascular disease to either aspirin 325 mg or clopidogrel 75 mg daily.24 The clopidogrel group had a significantly lower annual rate of vascular event than the aspirin group (5.32% vs 5.83%, p=0.043). Of note, the relative risk reduction in patients with prior stroke was 7.3% and not statistically significant. Haemorrhage risks were similar between the two groups. Therefore, clopidogrel is considered a good option for secondary stroke prevention.
Ticagrelor
Ticagrelor is a new generation P2Y12 receptor antagonist. It is not dependent on hepatic activation and has a more potent antiplatelet effect.25 The Acute Stroke or Transient Ischaemic Attack Treated with Aspirin or Ticagrelor and Patient Outcomes trial randomised patients with minor stroke (National Institutes of Health Stroke Scale (NIHSS) score <5) or high-risk TIA within 24 hours to either ticagrelor 90 mg two times a day or aspirin 100 mg daily for 90 days.25 There was no significant difference in the rate of stroke, myocardial infarction or death between the two groups (6.7% vs 7.5%; HR 0.89; p=0.07). Haemorrhage risk was also similar. Of note, ticagrelor had a 17.5% discontinuation rate primarily due to dyspnoea and bleeding. A subgroup analysis showed that ticagrelor was superior to aspirin in patients with ipsilateral atherosclerotic stenosis.26
Glycoprotein IIb/IIIa antagonists
Glycoprotein IIb/IIIa receptor antagonists, including abciximab, eptifibatide and tirofiban, represent a unique class of antiplatelet agents. Abciximab is a chimeric mouse/human monoclonal antibody with high affinity for the platelet glycoprotein IIb/IIIa receptor.27 It was used as an adjunct to thrombolysis or endovascular procedures. Abciximab in Emergency Treatment of Stroke Trial evaluated the efficacy and safety of abciximab in patients with AIS within 5 hours of symptoms onset. It was terminated early after 808 enrolments due to an unfavourable benefit–risk profile.28 There was significantly higher rate of symptomatic or fatal intracranial haemorrhage in the abciximab group (5.5% vs 0.5%; p=0.002) without significant outcome benefit (32% vs 33%; p=0.944). Therefore, glycoprotein IIb/IIIa antagonists for patients with AIS is harmful and should not be used for stroke prevention.10
Dual-antiplatelet therapy
The key RCTs investigating the efficacy of DAPT in secondary stroke prevention are listed in table 2. Management of Atherosclerosis with Clopidogrel in High-Risk Patients trial randomised patients with recent ischaemic stroke or TIA to either clopidogrel 75 mg or aspirin 75 mg and clopidogrel 75 mg daily for 18 months.29 There was a non-significant difference in primary outcomes (15.7% vs 16.7%) but a significantly higher risk of life-threatening bleeding in the DAPT group (2.6% vs 1.3%).
Randomised controlled trials evaluating dual-antiplatelet therapy (DAPT) in secondary stroke prevention
Subsequently, Clopidogrel for High Atherothrombotic Risk and Ischaemic Stabilisation, Management and Avoidance and SPS3 (Stoke Prevention of Small Subcortical Strokes) showed no difference in stroke recurrence but higher risk of bleeding in the DAPT group in patients with atherosclerotic risk factors or lacunar stroke, respectively.30 31
Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events (CHANCE) evaluated DAPT for 21 days in Chinese population with high-risk TIA or minor ischaemic stroke within 24 hours of symptom onset.32 A total of 5170 patients were randomised to either clopidogrel (300 mg on day 1, followed by 75 mg daily) for 90 days plus aspirin 75 mg daily for the first 21 days or placebo plus aspirin 75 mg daily for 90 days. DAPT group had a significantly lower rate of ischaemic or haemorrhagic stroke at 90 days than aspirin group (8.2% vs 11.7%, HR 0.68; p<0.001). The absolute risk reduction was 3.5%. There was no significant difference in the rate of haemorrhage between the two groups. The benefit persisted during 1-year follow-up.33
To determine if the results transcend to a broader population, POINT (Platelet-Oriented Inhibition in New TIA and Minor Ischaemic Stroke) trial was conducted in North America, Europe, Australia and New Zealand.34 It showed a significant risk reduction in recurrent ischaemic events (5.0% vs 6.5%, p=0.02 but increased rate of bleeding (0.9% vs 0.4%, p=0.02) with DAPT. Of note, there were some differences in the study design between POINT and CHANCE. The POINT trial included a higher loading dose of clopidogrel (600 mg) and longer DAPT duration (90 days). These differences may explain the increased risk of bleeding in the POINT trial.
The (Acute Stroke or Transient Ischaemic Attack Treated with Ticagrelor and ASA for Prevention of Stroke and Death) trial randomised patients with a mild-to-moderate acute noncardioembolic ischaemic stroke (NIHSS score ≤5) or TIA within 24 hours of symptom onset to either ticagrelor plus aspirin or placebo plus aspirin for 30 days.35 There were significant lower rates of stroke or death (5.5% vs 6.6%, HR, 0.83; 95% CI 0.71 to 0.96; p=0.02) and ischaemic stroke (5.0% vs 6.3%, HR, 0.79; 95% CI, 0.68 to 0.93; p=0.004), but higher rate of severe bleeding (0.5% vs 0.1%, p=0.001) in the DAPT group. Exploratory analysis showed that ticagrelor plus aspirin was associated with lower rate of disabling stroke or death than aspirin alone (4.0% vs 4.7%, p=0.001).36 For every 1000 patients, DAPT would prevent 11 strokes or deaths at the cost of four severe haemorrhages. The number needed to treat to benefit one patient is 143. In subgroup analysis of patients with ipsilateral atherosclerotic stenosis, ticagrelor plus aspirin was associated with lower rate of stroke or death than aspirin alone (8.1% vs 10.9%, p=0.023), resulting in a number needed to treat of 34 (95% CI 19 to 171).37
Stenting vs Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial compared medical therapy with intracranial stenting.38 Patients with a TIA or stroke attributed to 70%–99% stenosis of an intracranial artery were randomised to aggressive medical management with aspirin 325 mg and clopidogrel 75 mg daily for 3 months vs angioplasty and stenting plus aggressive medical management. The study was stopped early after enrolment of 450 patients due to a higher 30-day rate of stroke and death in the stenting group (14.7% vs 5.8%, p=0.002) primarily due to periprocedural complications. At a median follow-up of 32.4 months, the risk of stroke or death was 23% in the stenting group vs 15% in the medical group.39 These results supported the use of DAPT for 90 days in patients with symptomatic high-grade intracranial stenosis.10
CHANCE-2 trial randomised 6412 patients with a minor ischaemic stroke or TIA and CYP2C19 loss-of-function alleles to aspirin for 21 days plus ticagrelor or clopidogrel for 90 days.40 The risk of new stroke at 90 days was modestly lower in ticagrelor group (6.0% vs 7.6%, p=0.008). There was no difference in rate of severe or moderate bleeding between the two groups (0.3% vs 0.3%), but ticagrelor was associated with more total bleeding events (5.3% vs 2.5%).
The Antiplatelet Therapy with Aspirin, Clopidogrel and Dipyridamole vs Clopidogrel Alone or Aspirin-Dipyridamole in Patients with Acute Cerebral Ischaemia trial compared triple antiplatelet therapy versus SAPT.41 After randomising 3096 patients within 48 hours of AIS or TIA, the trial was stopped early due to significantly more bleeding in the triple therapy group (20% vs 9%, p<0.001) without a decrease in recurrent stroke or TIA within 90 days (6% vs 7%, p=0.47). Therefore, triple antiplatelet therapy is harmful and should not be used for stroke prevention.10 41
Cochrane systematic review, pooled data analysis and meta-analysis of RCTs demonstrated that DAPT with aspirin and clopidogrel or ticagrelor for 21–30 days is more effective than SAPT for secondary stroke prevention when initiated early after the onset of minor stroke or high-risk TIA.3 6–9 However, when initiated later and used longer than 90 days, DAPT increases the risk of bleeding without reduction of stroke recurrence than SAPT.7–9
Recommendations
The current evidence-based recommendations on antiplatelet therapy for secondary stroke prevention are summarised in table 3.3–10
Current guidelines on the use of antiplatelet therapy for secondary stroke prevention2 10
Special considerations
Antiplatelet therapy after intracerebral haemorrhage
Restart or Stop Antithrombotics Randomised Trial (RESTART) compared starting vs avoiding antiplatelet agent after intracerebral haemorrhage (ICH).42 At a median 3-year follow-up of 537 participants, there was no significant difference in recurrent ICH (8.2% vs 9.3%, p=0.64) or major vascular events (26.8% vs 32.5%, p=0.14) between two group.
Restarting antiplatelet therapy after ICH should be considered, particularly in patients with high-risk thromboembolic conditions.
Antiplatelet resistance
One-third of patients who had a stroke may develop recurrent stroke while on antiplatelet therapy, partly due to aspirin or clopidogrel resistance.43–45 In the laboratory studies, aspirin resistance is defined as a failure to achieve reduction in TXA2 formation.44 Clopidogrel resistance refers to the inability to inhibit ADP-mediated platelet aggregation.45
The most common cause of inadequate antiplatelet therapy is non-compliance.46 47 Approximately 50% of patients either stop taking medication or fail to adhere to the prescribed dose at 1 year.
Potential drug interactions may also result in reduced effect of antiplatelet therapy. Concomitant use of NSAIDs, particularly ibuprofen, offsets the clinical benefit of aspirin.48 Proton-pump inhibitors (PPIs) inactivates the hepatic enzyme that converts clopidogrel to its active metabolite. Therefore, concomitant use of PPIs may decrease clopidogrel’s effect.49
Clopidogrel resistance has also been linked to gene polymorphisms.50 Clopidogrel is a prodrug that requires conversion into active metabolite by hepatic CYP2C19. The prevalence of poor metabolisers (subjects carrying two loss-of-function alleles) is as high as 58.8% among Asians.51
Perspectives
Many challenges remain for the selection of optimal antiplatelet therapy in the real-world practice. Currently, we are still uncertain about the best antiplatelet therapy in different ethnic populations. For example, is cilostazol equally effective in blacks or whites as in Asians? We also need to know the best dose of medications, best combination and duration of DAPT among patients with diverse comorbidities, multiple vascular risk factors, high body mass index, CYP2C19 loss-of-function gene mutations or stroke recurrence while on antiplatelet therapy.
Ticagrelor does not need hepatic activation and was shown to be more effective than aspirin in patients with aortic arch and intracranial atherosclerotic disease.26 37 52 However, in patients with high risk of bleeding, cilostazol or aspirin-dipyridamole may be better option.17 21 22
A common clinical practice is increasing the dose of aspirin or choosing a different antiplatelet agent after a recurrent TIA or AIS while on aspirin.53 However, systematic review and meta-analysis did not show effectiveness of increasing the dose of aspirin or changing to another antiplatelet medication.54
Selecting of appropriate antiplatelet agent should also be based on compliance, drug tolerance or resistance.
In a systematic review and meta-analysis, CYP2C19 loss-of-function alleles were found in 25% of white patients and in 60% of Asian patients.55 Among 15 studies of 4762 patients with stroke or TIA treated with clopidogrel, carriers of CYP2C19 loss-of-function alleles were at greater risk of stroke in comparison with noncarriers (12.0% vs 5.8%; risk ratio, 1.92, 95% CI 1.57 to 2.35; p<0.001). Therefore, patients with ischaemic stroke or TIA may need CYP2C19 gene test. In carriers of CYP2C19 loss-of-function alleles, ticagrelor is preferred to clopidogrel for secondary stroke prevention.40
Additional RCTs are warranted to evaluate CYP2C19 gene testing-based antiplatelet therapy for stroke prevention: (1) Ticagrelor plus aspirin versus clopidogrel plus aspirin for patients with symptomatic intracranial stenosis and (2) Ticagrelor plus aspirin vs ticagrelor in patients with symptomatic intracranial stenosis or chronic large vessel occlusion.
Conclusion
SAPT is indicated for secondary stroke prevention in most patients with noncardioembolic ischaemic stroke or TIA. DAPT with aspirin and clopidogrel or ticagrelor for 21–30 days is more effective than SAPT for secondary stroke prevention when initiated early after minor noncardioembolic stroke or high-risk TIA. Aspirin is appropriate and cost-effective in antiplatelet naïve patients. Cilostazol, as off-label treatment, would be attractive alternative for patients with high risk for haemorrhage. In patients with intracranial stenosis, the addition of ticagrelor or cilostazol to aspirin for up to 30 days might reduce recurrent stroke risk. Ticagrelor might be preferred to clopidogrel in patients with CYP2C19 loss of function alleles.
Ethics statements
Patient consent for publication
Acknowledgments
We appreciate the generous support from the University of California Irvine Xiaoqi Cheng & Dongmei Liao International Stroke Research Scholarship.
References
Footnotes
Contributors JS contributed to drafting and revising the manuscript. SL contributed to literature review, data collection and revision of the draft. WY contributed to the conception, intellectual contents, revising the manuscript and final revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.