Article Text

Abstract
Backgrounds Increased blood pressure (BP) for patients who had an acute ischaemic stroke is associated with poor functional outcome, however the optimal timing of antihypertensive therapy is unknown.
Aims We aim to compare early antihypertensive treatment to delayed antihypertensive treatment for reducing the risk of composite major disability and mortality at 3 months in acute ischaemic stroke.
Design The China Antihypertensive Trial in Acute Ischemic Stroke II (CATIS-2) trial is a multicentre, randomised, open-label, blinded-endpoints trial that will be conducted in 100 hospitals in China. The primary outcome is the composite of death and major disability (modified Rankin Scale score ≥3) at 3 months of randomisation. Antihypertensive treatment will be received immediately after randomisation in the early treatment group, aimed at average systolic BP by 10%–20% reduction within the first 24 hours, and achieving an average BP level of <140/90 mm Hg within 5 days. Patients in the delayed treatment group will discontinue any antihypertension medications for the first 7 days of randomisation, and will receive antihypertensive therapy achieving a BP goal of <140/90 mm Hg after 7 days.
Conclusion The CATIS-2 trial will be testing the hypotheses that early BP lowering leads to improved functional outcome without any other harms, and developing clinical guidelines of the BP management for patients who had an acute ischaemic stroke.
Trial registration number NCT03479554.
- stroke
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction and rationale
Most of patients who had an ischaemic stroke (≥75%) experienced increased blood pressure (BP) at the acute phase.1 Meanwhile, high BP is strongly associated with poor functional outcome and recurrence of ischaemic stroke.2 3 However, whether and when to initiate the antihypertension therapy among patients who had an acute ischaemic stroke (AIS) remain unknown. A neutral effect of immediate BP lowering after ischaemic stroke on clinical outcomes has been reported in several clinical trials.4–6 In theory, moderate increased BP at acute stage of ischaemic stroke might be advantageous since higher BP may improve arterial perfusion of the ischaemic tissue. Otherwise, the initial hypertension phenomenon is self-limited and could resolve by few days after the onset. Therefore, avoiding hypertensive therapy in early days of stroke onset might be reasonable.7 Nevertheless, no clinical trials have tested the optimal time for starting antihypertensive therapy after ischaemic stroke. A subgroup analysis of the China Antihypertensive Trial in Acute Ischemic Stroke (CATIS)1 found that initiating antihypertensive treatment between 24 and 48 hours’ onset showed a beneficial effect on reducing death or major disability (OR 0.73, 95% CI 0.55 to 0.96, p=0.03) and recurrent stroke (OR 0.25, 95% CI 0.08 to 0.74, p=0.01) for patients who had an AIS.6 8 Thus, whether patients who had an AIS and high BP could benefit from antihypertensive therapy within 24–48 hours of onset warrants further studies.
In the proposed CATIS II (CATIS-2), the hypothesis testing that whether antihypertensive treatment starting within the first 24–48 hours of onset (early treatment group) in patients who had an AIS will be reducing the risk of composite case fatality and major disability (modified Rankin scale (mRS) score ≥3) at 3 months, compared with those who will receive the antihypertensive treatment starting on day 8 of stroke onset (delayed treatment group).
Methods
Design
The proposed CATIS-2 trial is a multicentre, randomised, open-label, blinded-endpoints trial. Patients are randomised 1:1 to early antihypertensive treatment group or delayed antihypertensive treatment group within 24–48 hours of stroke onset and followed up for 3 months. Patients in early antihypertensive treatment group will initiate their antihypertensive therapy immediately after randomisation. Patients in delayed treatment group will discontinue all of their family antihypertension medications within the first 7 days of stroke onset, and restart antihypertensive therapy on day 8 after stroke onset. BP measurements and relative data will be collected at the baseline, during the hospitalisation, on 21 and 90 days during the follow-up visit after randomisation. All study participants or their immediate family members will provide a written informed consent. The conduction, safety and efficacy of the study are supervised by an international independent Data and Safety Monitoring Board.
Patient population
In CATIS-2 trial, 4776 patients will be recruited from 100 participating centres within the China Stroke Clinical Research Network. The inclusion and exclusion criteria are shown in box 1. Patients with confirmed severe extracranial or intracranial artery stenosis (≥70%) before randomisation will be excluded from the trial. However, if the extracranial or intracranial arterial stenosis (≥70%) is detected after randomisation, the patients will be recommended to continue antihypertensive therapy and complete the follow-up visits.
Inclusion and exclusion criteria
Inclusion criteria
Men and women aged ≥40 years.
Acute ischaemic stroke confirmed by CT or MRI of the head.
Stroke onset within 24–48 hours.*
Systolic blood pressure between 140 and 200 mm Hg and diastolic blood pressure between 80 and 120 mm Hg.
Exclusion criteria
Haemorrhagic stroke confirmed by CT or MRI of the head.
CT or MRI-diagnosed vascular malformation, tumour, abscess or other major non-ischaemic brain disease (eg, multiple sclerosis).
Extracranial or intracranial artery stenosis (≥70%) in both sides or the affected side based on image study.
Stroke caused by arteritis, migraine, vasospasm or substance abuse.
Severe stroke (National Institutes of Health Stroke Scale score of ≥21).
Coma (Glasgow Coma Scale score <8).
Preceding moderate or severe dependency (modified Rankin scale score 3–5).
Planned or probable revascularisation (any angioplasty or vascular surgery) within 3 months after screening.
Intravenous thrombolytic therapy (such as intravenous alteplase) or mechanical thrombectomy.
Severe heart failure (New York Heart Association class III and IV) or left ventricular ejection fraction <35%.
Myocardial infarction or unstable angina within the past 3 months.
History of atrial fibrillation, aortic dissection or all-cause dementia.
Difficult-to-control hypertension (systolic blood pressure ≥170 mm Hg despite use of ≥4 antihypertensive medications for ≥6 months).
Acute renal failure or dialysis or estimated glomerular filtration rate <20 mL/min/1.73 m2.
Any clinical conditions judged by the clinical team to likely limit the adherence to study procedures.
Inability to understand and/or follow research procedures due to mental, cognitive or emotional disorders.
Unable to participate in the follow-up examination (eg, cannot travel to the participating hospital).
Participation in another clinical trial within 30 days.
Pregnant, currently trying to become pregnant, or of childbearing potential and not using birth control.
Failure to obtain informed consent from a participant.
*If stroke onset within 24 hours, patients will be asked to discontinue all home antihypertensive medications and will have their eligibility re-evaluated at 24 hours prior to randomisation.
Randomisation
Randomisation is via a central internet-based system and conducted at the Study and Data Coordinating Center, stratified by the use of antihypertensive medication and the participating hospitals. The block size will be random among 4, 6 and 8. The SAS PROC PLAN (SAS Institute, Cary, NC) will be used to generate the randomisation schedules. The trained investigators will log in to a password-protected website at site to obtain the randomisation assignment when an eligible case is screened.
Treatment
All home antihypertension medications will be discontinued at the screening/baseline examination among all eligible participants. All enrolled patients will receive treatment as follows:
Early antihypertensive treatment group: initiate antihypertensive therapy within 24–48 hours of stroke onset, lowering 10%–20% of systolic BP within the first 24 hours after randomisation and then achieve the target systolic BP below 140 mm Hg and diastolic BP below 90 mm Hg within 5 days, and to maintain this BP level afterwards.
Delayed antihypertensive treatment group: discontinue all home antihypertensive medications within the first 7 days after stroke. Initiate antihypertensive treatment on day 8 of onset and achieve systolic BP to <140 mm Hg and diastolic BP <90 mm Hg within 2 weeks, and maintain this BP level afterwards.
As for the therapy algorithm, in early treatment group, the first-line medication (ACE inhibitors (ACEIs) intravenous injection) could be selected alone, or in conjunctive use with other potential medications (second line of calcium channel blockers (CCBs), third line of diuretics) to achieve the systolic BP target within the first 24 hours (figure 1). The dosage of medications used will be titrated to achieve BP targets within 5 days and then maintain the same level afterwards. If the target BP level is achieved at any step mentioned above, the same dosages of medication will be continued to maintain the target BP level. But if the BP target is not reached by therapeutic algorithm, the maximum dosage of medications will be titrated up in the sequence of ACEIs, CCBs and diuretics before adding additional agent. A fourth agent will be recommended if necessary. This treatment algorithm and these antihypertensive medications are safe and effective in the CATIS trial.6 Above treatment strategies are recommended but not exclusive, any individual antihypertensive therapy to achieve BP targets is allowed.

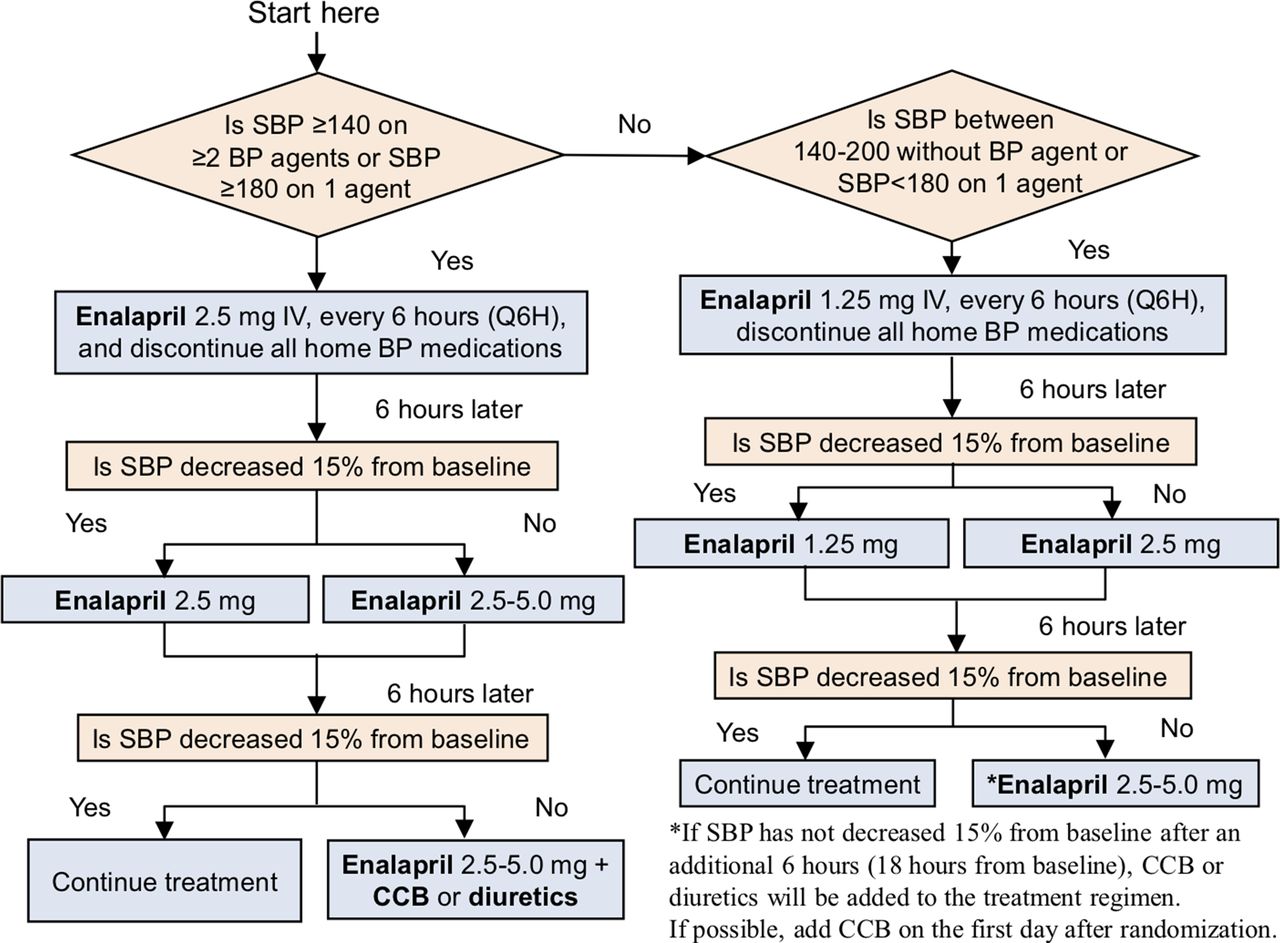{kind=link}
Treatment algorithm for early antihypertensive treatment group. BP, blood pressure; CCB, calcium channel blockers; SBP, systolic BP.
Besides antihypertensive therapy, the same standard management will be applied to both groups on the basis of current guidelines.9 10 For safety concerns, patients in the delayed antihypertensive treatment group can start immediately antihypertensive therapy if systolic BP >180 mm Hg. This treatment decision is decided by the treating physicians and needs to be recorded. Researchers are also allowed to decide on individual BP target during the first 7 days in patients with severe arterial stenosis discovered after randomisation.
BP measurements
BP will be measured every 3 hours within the first 24 hours and every 8 hours during day 2 to discharge or through day 14. All participants are required at least 7 days of hospital staying. At 21-day and 3-month follow-up visit, their BP will also be recorded. For each BP assessment, three brachial BP measurements are required 30 s apart by using an automated measurement device (Omron HBP-1300 Professional BP Monitor) with patients in the supine position. All three measures will be recorded.
Primary outcomes
The primary outcome is a composite of death and major disability (mRS ≥3) at 3 months.
Secondary outcomes
The major secondary outcome is the first recurrent stroke event (haemorrhagic or ischaemic) within 3 months of follow-up. The others include (1) shift in scores of mRS11 at 3 months; (2) all-cause death during 3 months; (3) major vascular disease events during 3 months of follow-up; (4) vascular cognitive impairment measured by the Montreal Cognitive Assessment (MoCA)12 in Chinese at 3 months and (5) health-related quality of life measured by the 12-item Short Form13 at 3 months.
Sample size
The estimated sample size is 4776 (2388 for each randomisation group). The sample size was calculated on the following: (1) significance level of 0.05 for a two-sided test; (2) statistical power of 85%; (3) 3-month event rate of primary outcome of 25% in control group based on the CATIS trial data6; (4) proportional risk reduction of 15% (rate ratio=0.85)14 and (5) 5% loss to follow-up over 3 months.6 Power analysis was implemented in the Power Analysis and Sample Size software (NCSS, Kaysville, Utah, USA).
Statistical analyses
Data will be analysed according to intention-to-treat principle. For the primary hypothesis, the difference in the proportion of a composite primary outcome of all-cause death and major disability at 3 months between treatment groups will be compared using χ2 tests. Relative risk regression will be used to obtain relative risks and 95% CIs associated with early treatment. Important covariables, including baseline age, gender, systolic BP, National Institutes of Health Stroke Scale (NIHSS) score, time of onset to randomisation, history of hypertension and use of antihypertension therapy will be adjusted in a sensitivity analysis. The same statistical analysis methods will be used for secondary endpoints of all-cause mortality and major vascular disease events.
For major secondary outcome hypothesis, time-to-event analysis will be used to compare the cumulative hazards of recurrent stroke between the early treatment group and the delayed treatment group. Kaplan-Meier curves on cumulative hazards by follow-up time will be examined and the group differences will be tested by log-rank test. Cox proportional hazards models, implemented in the SAS PHREG procedure, will be used to obtain HRs and 95% CIs. Neurological functional status assessed by the mRS at 3 months will be analysed as ordinal categorical variables. The treatment groups’ difference will be tested using a Wilcoxon rank-sum test. The effect of BP reduction in the full range of the mRS will be estimated by ordinal logistic regression. A Wilcoxon rank-sum test will be used to compare the average MoCA scores between groups because of potential outliers and abnormal distribution. Complete case analysis will be used for the primary analyses. Multiple imputation for missing data will be conducted using the Markov chain Monte Carlo method in a sensitivity analysis. Two-sided p<0.05 will be considered statistically significant.
Subgroup analyses
Analysis of the effects of early antihypertensive treatment on outcomes by prespecified subgroups will be conducted, including: (1) age (<65 vs ≥65 years); (2) gender (men vs women); (3) systolic BP at baseline (<160, 160–179 and ≥180 mm Hg); (4) NIHSS score at baseline (0–4, 5–15 and ≥16); (5) history of hypertension (yes vs no); (6) use of antihypertensive medications on admission (yes vs no) and (7) subtypes of ischaemic stroke15 (large artery atherosclerosis, cardioembolism, small vessel disease, stroke of the other or undetermined aetiology).
Discussion
BP management in AIS is always the focus of clinical practice and research. High BP is the leading risk factor of ischaemic stroke.16 Among all the risk factors for stroke, BP control emerges as one of the most important controllable factors, which may promote a better outcome if good management has been implemented.
A U-shaped association between functional outcome with admission BP level has been widely reported.2 17 18 Whether and when to lower BP among patients who had an AIS are critically important but controversial. Despite several large clinical trials4–6 19 showed neutral overall clinical effect of BP lowering at acute phase for patients who had an ischaemic stroke, starting or restarting antihypertensive treatment in patients with BP >140/90 mm Hg who are neurologically stable is safe unless contraindicated.9 10 However, the timing of starting antihypertensive treatment was not clear as no available clinical trials have offered any evidence. Initiation of antihypertension therapy within 24 hours of stroke onset was done among majority of participants in previous trials.4–6 19 However, these trials did not support a major benefit shift towards BP lowering in patients who had an AIS with or without intravenous alteplase therapy. Whereas, a subgroup of CATIS trial generated hypotheses that among patients who had an AIS, BP lowering initiated between 24 and 48 hours after stroke onset might reduce risk of death, major disability, recurrent stroke and vascular events.8 The specified mechanism of this hypothesis is unclear, thus it needs to be further detected. Generally, elevated BP in patients who had an AIS often reflects undiscovered or uncontrolled hypertension. However, due to acute psychological stress, potential compensatory cerebral perfusion or other non-specific reasons such as urine retention, an early hypertensive response is common in patients who had an AIS, which mostly spontaneously falls in the first few hours and resolves over days following the stroke onset.7 20 Thus, BP management within the first 24 hours should be careful to avoid hypoperfusion. Patients with high BP (>140 mm Hg) during 24–48 hours’ onset might be truly those who need and could benefit from antihypertensive therapy. To detect this, the proposed CATIS-2 trial is the first randomised clinical trial to compare the effect of early antihypertensive treatment within the first 24–48 hours after stroke onset and delayed treatment after 7 days of onset on major disability or deaths among patients who had an AIS. Since patients with atrial fibrillation and severe cranial arterial stenosis are not enrolled, the results will not apply to this group of patients. Besides, another limitation of our study is that there are no neuroimaging endpoints in the trial for cerebral oedema and haemorrhagic transformation might be closely associated with increased acute BP levels.21 22 Despite this, the cerebral imaging, for example, CT or MRI of every participant was routinely obtained as DICOM digital in China Stroke Clinical Research Center for further potential analysis when needed. Overall, CATIS-2 trial will provide important research data of clinical question, of when to initiate antihypertensive treatment and demonstrate important information for developing clinical guidelines for the early BP management among patients who had an AIS.
Ethics statements
Ethics approval
This study was evaluated and approved by the Institutional Review Board at Beijing Tiantan Hospital, Capital Medical University (ID: KY2017-021-04), as well as medical ethical committees at all 100 participating centres.
Acknowledgments
The authors thank all participating hospitals, their physicians, nurses and other personnel who participated in the study, and the CATIS-2 Steering Committee members.
References
Footnotes
Twitter @yilong
Contributors LL, YiW, YZ, JH and YoW conceived the study and oversaw all scientific aspects of its implementation. LL, XX, DL and DW drafted the manuscript. XX, DL, AW, PW, SS, CZ, YW, TX, YP, YJ and XM recruited hospitals and operated the CATIS-2 trial.
Funding This work was supported by grant from the Ministry of Science and Technology of the People’s Republic of China (2016YFC1307300, 2018YFC1312402) and National Natural Science Foundation of China (81820108012).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.