Article Text

Abstract
Background Orolingual angio-oedema is a recognised complication of tissue plasminogen activator (tPA) for ischaemic stroke. We investigated its incidence, clinical characteristics and relationship with other factors in patients receiving tPA at a UK centre.
Methods 530 consecutive patients (median age 70 years) receiving tPA treatment for confirmed ischaemic stroke were included. Cases were defined as those developing angio-oedema within 24 h of initiation of tPA. Angio-oedema was retrospectively classified as mild, moderate or severe using predefined criteria. The primary analysis was the association between prior ACE inhibitor (ACE-I) treatment and angio-oedema.
Results Orolingual angio-oedema was observed in 42 patients (7.9%; 95% CI 5.5% to 10.6%), ranging from 5 to 189 min after initiation of tPA (median 65 min). 12% of the angio-oedema cases were severe (1% of all patients treated with tPA), requiring urgent advanced airway management. 172 patients (33%) were taking ACE-I. In multifactorial analyses, only prior ACE-I treatment remained a significant independent predictor of angio-oedema (odds ratio (OR) 2.3; 95% CI 1.1 to 4.7).
Conclusions Angio-oedema occurs more frequently than previously reported and is associated with preceding ACE-I treatment. Angio-oedema may be delayed and progress to life-threatening airway compromise, which has implications for the assessment and delivery of thrombolysis.
- Stroke
- Cerebrovascular Disease
Statistics from Altmetric.com
Introduction
Angio-oedema, an immune-mediated subcutaneous and submucosal swelling caused by increased vascular permeability, is a recognised complication of recombinant tissue plasminogen activator (tPA, alteplase) therapy for ischaemic stroke. The incidence of angio-oedema in patients receiving alteplase for ischaemic stroke has been reported as 1.3–5.9%.1–6 It typically manifests as a mild, transient hemifacial swelling starting in the tongue, often contralateral to the ischaemic hemisphere, and usually resolves within 24 h.7 However, angio-oedema may rapidly progress to cause upper airway obstruction, which may be fatal. Available data from a small number of observational studies suggest that life-threatening airway compromise requiring anaesthetic intervention is rare, occurring in around 0.2–0.8% of all patients receiving tPA, or around 13% of those developing angio-oedema.1 ,2
The pathophysiological basis for angio-oedema complicating thrombolysis in ischaemic stroke is poorly understood. Existing treatment with ACE inhibitor (ACE-I) and signs of acute insula/frontal ischaemia on baseline CT of the brain were associated with the development of angio-oedema in one previous study.1 A better understanding of the clinical characteristics and factors associated with development of angio-oedema might help predict at-risk individuals, thereby optimising management. The aims of the present study were to investigate the incidence of angio-oedema, its clinical characteristics and relationship with baseline clinical factors in patients receiving tPA at a single UK centre.
Methods
We conducted retrospective analyses of data collected prospectively for consecutive patients receiving intravenous and/or intra-arterial thrombolysis with tPA at Salford Royal Foundation Trust (SRFT) between 20 December 2004 and 1 May 2012. Thrombolysis started at SRFT in 2004, and since 2009, SRFT has served a population of around 2.7 million at the Greater Manchester Comprehensive Stroke Centre (CSC). Intravenous thrombolysis is administered in accordance with regionally agreed protocols in agreement with National Clinical Guidelines for Stroke.8
Eligibility criteria
Patients aged ≥16 years treated with tPA (any dose, intravenous and/or intra-arterial), with a confirmed diagnosis of acute ischaemic stroke were included.
Data collection
Consecutive patients receiving treatment with intravenous tPA and/or intra-arterial intervention with tPA were prospectively identified and routine baseline demographic and clinical data were collected for an ongoing angio-oedema audit. This included age; sex; ethnicity; vascular risk factors; prior medication history (including ACE-I therapy) and allergies; stroke subtype using the Oxford Community Stroke Project (OCSP) classification9; baseline National Institutes of Health Stroke Scale (NIHSS) score10 and pretreatment blood pressure, pulse rate and venous glucose concentration. Selected patients underwent CT angiography and/or CT perfusion. Cases were defined as patients developing angio-oedema within 24 h of initiation of tPA. Angio-oedema was classified retrospectively as either mild: unilateral involvement, without progression to involve bilateral structures or airway compromise; moderate: bilateral involvement but without progression to impending or actual airway compromise; or severe: impending or actual airway compromise.
Statistical analyses
The baseline characteristics of angio-oedema cases and non-cases were compared using summary statistics. The primary analysis was to estimate the association between prior ACE-I treatment and the development of angio-oedema using multifactorial logistic regression analyses. As well as an indicator of prior ACE-I treatment, core, non-modifiable patient factors such as age, stroke severity (baseline NIHSS), vascular health (history of hypertension) and calendar time were included in all models. Further factors hypothesised to be influential in the pathophysiology of angio-oedema or related to ACE-I use were explored in the multifactorial analyses but eliminated if not statistically significant. These factors included smoking status, diabetes, coronary heart disease, previous stroke/transient ischaemic attack, stroke syndrome, affected hemisphere and route of tPA administration. The conventional threshold for significance (p=0.05) was used throughout. The sensitivity, specificity, and positive predictive and negative predictive values (NPV) of ACE-I for angio-oedema were also calculated.
Results
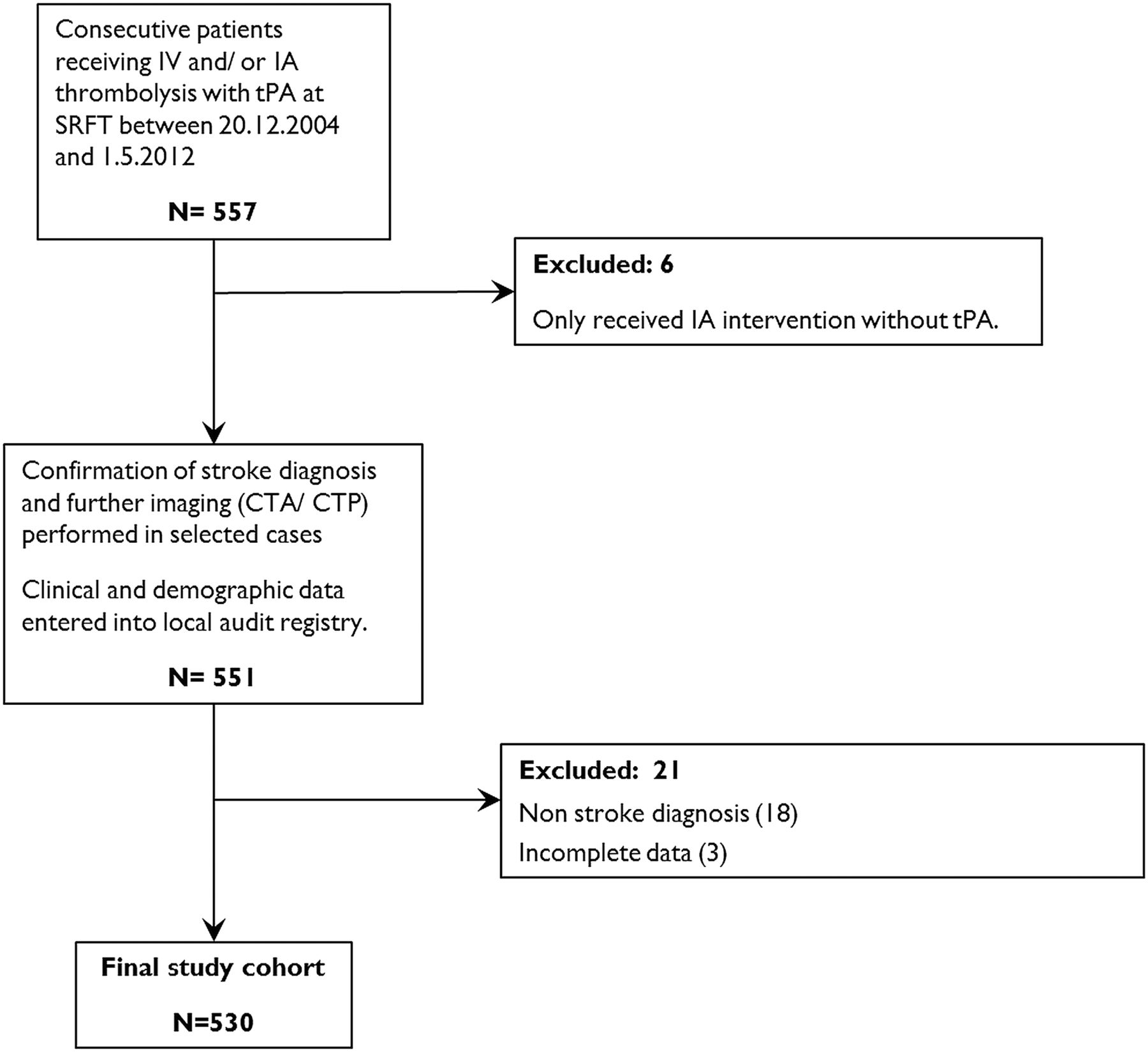
Five hundred and thirty consecutive patients who had confirmed ischaemic stroke and treated with tPA were included in the final analyses (figure 1). Table 1 shows the baseline characteristics. At presentation, 172 (33%) were taking ACE-I. Among these patients, 62% of those with diabetes and 49% of those with hypertension were taking an ACE-I. The median onset to needle time was 156 min (IQR 75 min) and the median door to needle time was 59 min (IQR 39 min). Twenty-two (4%) patients received either combined intravenous tPA+intra-arterial tPA±thrombectomy or stand-alone intra-arterial tPA±thrombectomy.
Baseline characteristics of all patients receiving intravenous±intra-arterial tPA, and stratified by presence of angio-oedema

{kind=link}
Flow diagram showing patient eligibility (IV, intravenous; IA, intra-arterial; tPA, tissue plasminogen activator; SRFT, Salford Royal Foundation Trust; CTA, CT angiography; CTP, CT perfusion imaging).
The incidence of angio-oedema was 7.9% (95% CI 5.5% to 10.6%). The onset of angio-oedema ranged from 5 to 189 min after initiation of tPA (median 65 min). In multifactorial analyses, prior treatment with an ACE-I remained a significant independent predictor of developing angio-oedema after tPA (OR 2.3; 95% CI 1.1 to 4.7; p=0.02; see online supplementary table S1). Predictive values for ACE-I are outlined in online supplementary table S2. Owing to the relatively small number of angio-oedema cases, the positive predictive values were low. The NPV for any angio-oedema severity was 95%, increasing with the severity of stroke and angio-oedema. The sensitivity for severe and moderate/severe cases was 75% and 80%, respectively.
In relation to the affected hemisphere, onset of angio-oedema was contralateral in 43%, ipsilateral in 14%, bilateral in 17% and not defined in 26%. Angio-oedema was predominantly mild in severity (see online supplementary table S3), but was severe in 12% of angio-oedema cases and 1% of all patients receiving tPA. Intravenous chlorphenamine, intravenous hydrocortisone and nebulised epinephrine were all used in the majority of cases. C1 esterase inhibitor and/or intramuscular epinephrine therapy was required in a minority of cases. In the five patients with severe angio-oedema, four required urgent endotracheal intubation and the other required emergency cricothyroidotomy. Two of the patients with severe angio-oedema (40%; or 5% of patients developing any angio-oedema) died within 48 h. Severe airway compromise secondary to angio-oedema contributed significantly to death in both cases.
Discussion
In our experience, angio-oedema complicating stroke thrombolysis in patients treated with tPA occurs more frequently than previously reported.1 ,2 ,6 Differences in the reported frequencies of angio-oedema may reflect over-reporting or under-reporting of milder, self-limiting cases; varying case mix (ethnicity, comorbidities) or prescribing (eg, ACE-I). We report a significant association between ACE-I and development of angio-oedema after adjustment for confounding factors, but the magnitude of this was considerably smaller than reported previously (OR 16.7; 95% CI 3.3 to 84.3).1 This may reflect the higher proportion of patients taking ACE-I in our study (33%) compared with 20% in the study reported by Hill et al.1 The sensitivity and specificity of ACE-I overall were limited, and the predictive values were influenced by the relatively low number of cases.
The aetiology of tPA-related angio-oedema is thought to be related to bradykinin production. tPA generates bradykinin via its hydrolysis of plasminogen to plasmin,1 ,11 which in turn activates the different components of the plasma contact system.11 Bradykinin is a member of the kinin family, a group of powerful vasodilator peptides, and has been implicated as the effector molecule in the process of tPA-related and ACE-I-related angio-oedema12 by activating the vascular bradykinin B2 receptors. Bradykinin is metabolised by three zinc metalloproteinases (kinase I, II and aminopeptidase P) into des-Arg9-bradykinin, a potent B1 receptor agonist.11 The occurrence of angio-oedema may be affected by genetic variation in kinase I and aminopeptidase P (APP) expression and the inhibition of ACE, a kinase II, by ACE-I.
The reported incidence of angio-oedema after tPA in myocardial infarction (0.02%)13 is much lower than that of ischaemic stroke. Bradykinin release has been reported in response to cerebral damage and B2 kinin receptors are upregulated in dying neurons and have been shown in experimental stroke models to mediate brain oedema.14 ,15 Therefore, cerebral ischaemia itself may contribute to the development of angio-oedema in susceptible individuals, such as those treated with ACE-I or receiving tPA, by accentuating bradykinin release.
Another hypothesis for this disparity proposes centrally mediated autonomic dysregulation as a consequence of insula infarction; indeed, the relative risk of angio-oedema post-tPA for insula infarction is approximately 4.8 (CI 1.2 to 18.4).1 While the vast majority of cases in our study presented clinically with middle cerebral artery (MCA) territory cortical infarction syndromes, we do not routinely record the ASPECTS (Alberta Stroke Program Early CT Score) and therefore did not investigate associations between MCA territory ischaemia and angio-oedema. However, a previous study reported angio-oedema in a patient with bilateral basilar artery territory infarction,6 and we observed angio-oedema in one patient with a proven proximal posterior cerebral artery occlusion prior to intravenous tPA administration.
Our findings have several implications for clinical practice. We show that angio-oedema may develop either within minutes after initiation of the tPA bolus, or after the infusion has completed, and while angio-oedema is generally mild and self-limiting, it may rapidly progress to life-threatening airway compromise. First, this highlights the importance of all thrombolysis-active units having well-defined pathways for assessment and urgent management of angio-oedema (see online supplementary figure S1 for an example developed in our centre), including locally agreed anaesthetic protocols. However, the optimal treatment of angio-oedema in this setting is unclear, and potential adverse effects of treating angio-oedema (eg, using corticosteroids) need to be borne in mind in individual cases. Second, the potential for life-threatening angio-oedema should be routinely included in the risk-benefit profile discussed with patients and their advocates prior to thrombolysis. However, this small risk should be discussed in the context of the overall benefits of thrombolysis; namely that t-PA given up to 4.5 h from onset confers lower risk of disability at 90 days, when compared with placebo (OR 1.42; 95% CI 1.02 to 1.98; p=0.04; number needed to treat (NNT)=14).16
Strengths of our study include prospective, consecutive data collection and complete ascertainment of patients receiving thrombolysis. Limitations include retrospective allocation of angio-oedema severity status in some instances, unavailability of baseline imaging ASPECTS to evaluate potential associations between insula ischaemia and angio-oedema and the restriction to a single UK centre with limited ethnic diversity (94% Caucasian).
In conclusion, angio-oedema is a potentially life-threatening consequence of tPA use in ischaemic stroke and its incidence may be higher than previously reported. This warrants increased vigilance for any developing signs of angio-oedema, and necessitates locally agreed protocols for observation and urgent management. Particular attention should be applied to patients with a history of ACE-I use as this may increase the risk of developing angio-oedema.
Acknowledgments
The authors are extremely grateful to all of the participating patients and the staff at the Greater Manchester Comprehensive Stroke Centre. They also gratefully acknowledge the assistance of Sharon Hulme, Senior Research Manager at the Stroke and Vascular Research Centre, and the support provided by Salford Royal NHS Foundation Trust and the University of Manchester.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors CJS, PJT and AV were involved in study concept and design. CJS, SR, MK and RH were involved in acquisition of data. RH, SR, MK, AV and AH were involved in statistical analysis. SR, RH, CJS and AV were involved in interpretation of data. RH and CJS were involved in drafting of the manuscript. All authors were involved in critical revision of the manuscript for important intellectual content. CJS was involved in study supervision.
-
Competing interests None.
-
Ethics approval National Research Ethics Committee North West.
-
Provenance and peer review Not commissioned; externally peer reviewed.