Article Text

Abstract
OBJECTIVE To assess the treatment results of radiosurgery for brain stem arteriovenous malformations (AVMs) and to seek optimal dose and treatment volume prescription for these lesions.
METHODS The clinical and radiological data of 30 consecutive patients with brain stem AVM treated with gamma knife radiosurgery were retrospectively reviewed with a mean follow up period of 52.2 months. There were 26 patients with previous haemorrhages and 21 with neurological deficit. Seventeen AVMs were located in the midbrain, 11 in the pons, and two in the medulla oblongata. All of the lesions were small with the intra-axial component occupying less than one third of the area of brain stem parenchyma on axial section of multiplaner MRI or CT. The mean diameter of the nidus was 1.26 cm, and the nidus volume within the brain stem parenchyma ranged from 0.1 to 2.0 cm3. The mean radiation dose to the AVM margin was 18.4 Gy.
RESULTS The actuarial 3 year obliteration rate was 52.2%; 69.4% in cases treated with standard doses (minimum target dose, 18–20Gy), and 14.3% in cases treated with low doses (<18 Gy) (p<0.05). Two patients sustained symptomatic radiation injury, but there was no permanent neurological deficit caused by radiosurgery. Five patients had haemorrhage from the AVM after irradiation, including four fatal cases, resulting in a 4.0% annual rate of post-treatment bleeding.
CONCLUSIONS Radiosurgery is a viable treatment modality for patients with small deep parenchymal brain stem AVMs. A standard radiosurgical dose is safe and effective when directed to a small treatment volume. However, latent interval haemorrhage remains a significant problem until the nidus is obliterated completely.
- gamma knife
- radiosurgery
- arteriovenous malformation
- brain stem
Statistics from Altmetric.com
During the past two decades, stereotactic radiosurgery has been widely used for the treatment of cerebral arteriovenous malformations (AVMs). Several authors described successful radiosurgical results of AVMs located in the critical areas of the brain,1-5 but, as for the long term results in the brain stem AVMs, little information is available on this relatively new treatment modality.6 7Although radiosurgery is apparently considered as a valid treatment,8 9 it is also known to cause serious neurological deterioration when used for brain stem lesions,10-14 and at present, no widely accepted standard protocols of radiosurgery in this region have been established. To add to such still limited knowledge, we retrospectively reviewed 30 consecutive patients with radiosurgically treated AVMs in the brain stem for their clinical characteristics, treatment parameters, and outcomes. The main purpose of this study was to seek the specific dose and treatment volume prescription for safe and effective radiosurgery to brain stem AVMs.
Patients and methods
PATIENT POPULATION
From July 1990 to October 1997, 30 patients (18 males and 12 females) with angiographically proved brain stem AVMs underwent radiosurgical treatment at our institution. The patients' ages ranged from 7 to 66 years (mean 35.7 (SD 15.5)). The initial manifestation was haemorrhage in 24 patients, headache in three, seizure in one, obstructive hydrocephalus in one, and tinnitus in one. Before radiosurgery, 26 patients (86.7%) had 34 haemorrhages from AVMs. The mean interval between the last haemorrhage and irradiation was 9.7 (SD 11.7) months (range 2 to 46). Three had undergone transarterial embolisation, three had other surgical interventions (ventricle-peritoneal shunt placement in one, ventricular drainage in one, haematoma evacuation in one), and another three had conventional radiotherapy. At radiosurgery, 21 patients (70%) had a fixed neurological deficit. The most frequent symptom was the eye movement disturbances, followed by cerebellar and pyramidal signs. Most patients were ambulatory, and Karnofsky performance status score was 90 or greater in 20 (66.7%) patients (mean 86.7 (SD 15.6); range 30–100). The clinical features of treated patients are summarised in table1.
Patient characteristics (n=30)
CHARACTERISTICS OF AVMS
In all cases, the AVM characteristics were defined by cerebral angiography in combination with CT or MRI. Seventeen AVMs (56.7%) were located in the midbrain, 11 (36.7%) in the pons, and two (6.7%) in the medulla oblongata. In 15 patients (50%), the whole nidus was located within the brain stem parenchyma, and in the other 15, the nidus partially involved surrounding structures (galenic, quadrigeminal, or parapontine cisterns in 11, thalamus in four, fourth ventricle in three, and cerebellar vermis in one). Pial or subpial lesions were excluded from the study. All irradiated lesions were small (⩽2 cm in diameter). In all cases, the intra-axial component occupied less than one third of the area of brain stem parenchyma on axial section of multiplaner MRI or CT. The mean diameter of the nidus ranged from 0.57 to 2.00 cm (mean 1.26 (SD 0.44) cm), and the mean volume ranged from 0.10 to 3.92 cm3 (mean 1.35 (SD 1.27) cm3). The diameters of brain stem parenchymal components ranged from 0.35 to 1.62 cm (mean 0.89 (SD 0.33) cm), and the volumes ranged from 0.10 to 2.00 cm3 (mean 0.60 (SD 0.49) cm3). Most of the AVMs were supplied bilaterally by branches of the superior cerebellar artery (SCA; 15 cases), anterior inferior cerebellar artery (AICA; seven), posterior inferior cerebellar artery (PICA; five), lateral or medial posterior choroidal artery (PChA; eight), or the fine perforators from the basilar artery (BA; 11), and 13 of these had multiple feeders. In 20 cases, the AVM drained superiorly into the galenic system via lateral mesencephalic, basal, or superior cerebellar veins. In 11 cases it drained laterally into the petrosal vein. One had partial drainage to the vein of Labbe. The summary of neuroradiological findings of treated AVMs are described in table 2.
AVM characteristics (n=30)
RADIOSURGICAL TREATMENT
Radiosurgery was performed using a 201 source 60Co gamma unit (Elekta Instruments, Atlanta, GA, USA). Definition of the nidus and localisation of the irradiation target were done on biplane stereotactic cerebral angiography. After April 1992, stereotactic thin slice multiplaner CT or MRI was used in combination to obtain precise three dimensional configurations of the nidus. A MicroVAX computer system (Digital Equipment Corporation, Westminster, MA, USA) was used in complex dose planning. All patients had irradiation of the entire nidus in a single session encompassed by 30–80% (mean 53.0 (SD 8.9) isodose contour. The mean radiation dose to the AVM margin (minimum target dose) was 18.4 (SD 2.9) Gy (range 10–20.4). Initially, the lower doses of 10–17 Gy were used in seven patients, but the lack of adverse effect of the irradiation at the higher end of this range prompted us to scale up the doses in a stepwise fashion to the standard radiosurgical dose of 18–20.4 Gy. The mean dose to the centre of the AVM (maximum target dose) was 35.5 (SD 6.7) Gy (range 20–50 Gy). The number of isocentres used varied from one to 10 (mean 3.4 (SD 2.4) per patient). All patients were discharged from the hospital uneventfully on the next day.
STATISTICAL ANALYSIS
Cumulative rates of angiographical obliteration and post-treatment survival rate were calculated using the actuarial method of Kaplan-Meier, and log rank (Mantel-Cox) and Peto-Peto-Wilcoxon test were used for statistical analyses. For non-parametric variables, the Mann-Whitney rank test was used. The level of statistical significance was p<0.05.
Results
CLINICAL OUTCOME
The follow up data were available in 29 of 30 patients (96.7%) with only one patient lost to follow up. At the last follow up 6 to 96 months (mean 52.2 (SD 31.3)) after the treatment, nine remained and an additional eight improved to be symptom free. Four improved significantly but still had a focal neurological deficit. Three had fixed neurological deficit that had existed before radiosurgery. Five patients died; four from intracranial haemorrhage, and one from pneumonia. The 5 year survival rate after radiosurgery calculated by the Kaplan-Meier method was 87.5%. The mean Karnofsky performance status score at the last follow up in patients without post-treatment haemorrhage was significantly higher than that at the time of radiosurgery (93.3 (SD 15.5) v 86.7 (SD 15.6); p<0.05).
OBLITERATION RESULTS
Twenty seven patients underwent neuroradiological evaluation 6–96 months after radiosurgery. One patient refused any neuroradiological examination, one died shortly after radiosurgery without neuroradiological check up, and one was lost to follow up. At the last angiographical evaluation, complete obliteration was confirmed in 12 (44.4%) (fig 1), subtotal obliteration (no visualisation of nidus with persistent AV shunt) in three (11.1%), and partial obliteration in 12 (44.4%). The actuarial complete obliteration rate of all treated AVMs was 52.2% at 3 years (fig 2 A). When assessed separately, lesions receiving standard radiosurgical dose (18–20Gy at periphery) obliterated significantly better than lesions receiving low dose treatment (<18Gy), with the actuarial 3 year rates of 69.4% versus 14.3% (p<0.05; fig 2 B). No other clinical characteristics or treatment parameters influenced the obliteration rate.

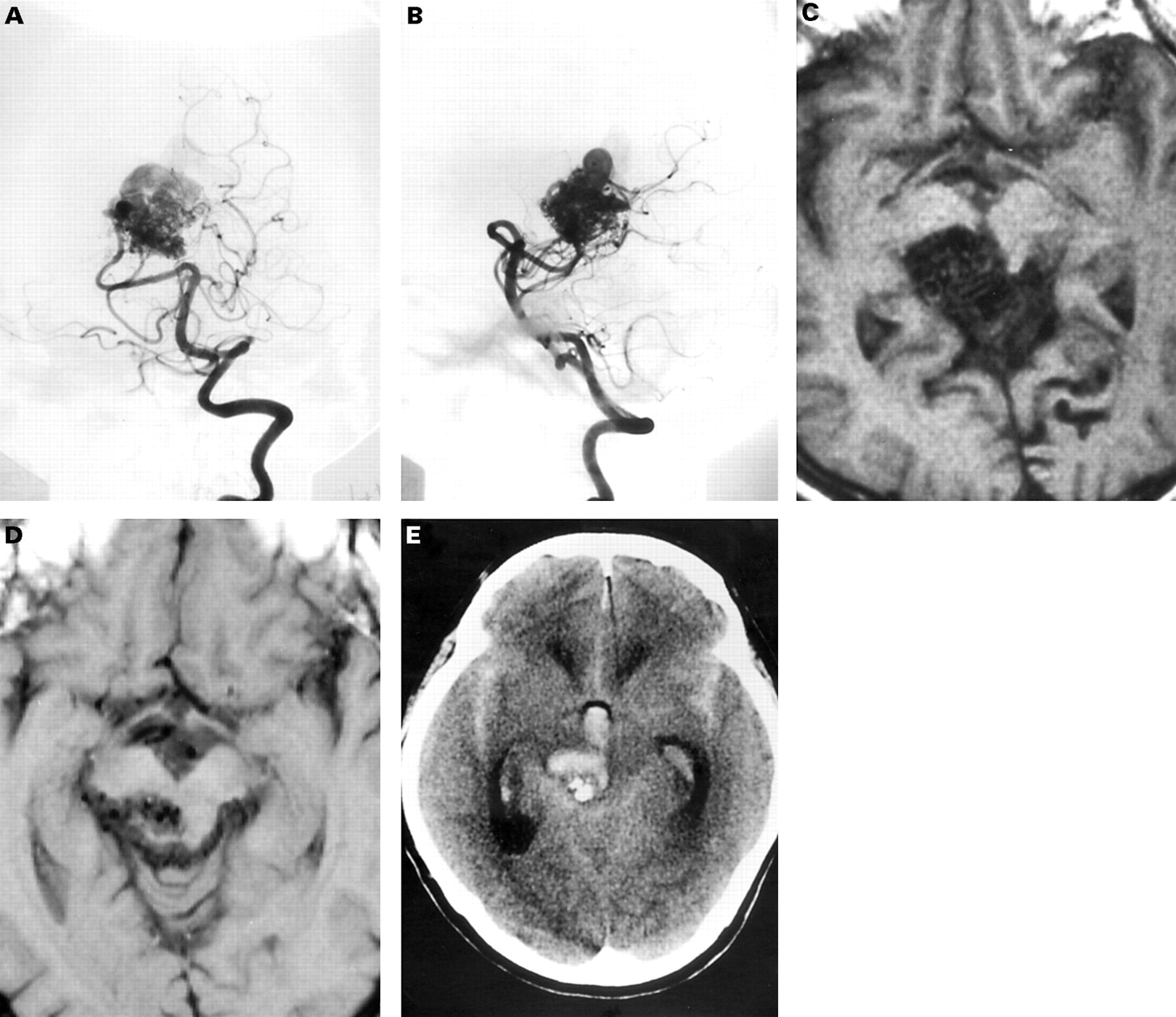
Neuroimages in a 39 year old woman with pontine haemorrhage. Left vertebral angiograms (A, B) and contrast enhanced CT (C) before radiosurgery show a ruptured pontine arteriovenous malformation (AVM). Left vertebral angiograms (D, E) and contrast CT (F) obtained 2 years after radiosurgery demonstratie total obliteration of the AVM.

(A) Kaplan-Meier curve showing cumulative rate of complete obliteration for the 27 patients followed up radiologically. Patients with complete AVM obliteration are indicated with closed circles, and patients without obliteration at the last observation, which are censored at that time point, are indicated with open squares. The cumulative complete obliteration rate was 52.2% at 3 years. (B) Plots stratified by minimal target dose. The solid line denotes patients treated with standard dose (⩾18 Gy, 20 patients), and the dotted line denotes patients treated with a low dose (<18Gy, seven patients). The actuarial obliteration rates of each category were 69.4% and 14.3%, respectively. The difference was significant (p<0.05).
COMPLICATIONS
Two patients (6.9%) with mid-brain AVM experienced symptomatic radiation injury seven and 24 months after irradiation; ptosis and ataxia in one, eye movement disorder in the other. Both patients were given oral corticosteroid, and the symptom resolved within a year. No patient had permanent deficit attributable to radiosurgery. Among 27 patients who underwent follow up neuroradiological examinations, radiation induced brain stem oedema was detected in five cases (18.5%) at 5–30 months after irradiation (fig 3). All these findings were reversible, and were asymptomatic in four, and transiently symptomatic in one. Another patient developed transient eye movement disorder without neuroradiologically detectable parenchymal change. Prescribed radiation dose to the AVM margin and volume of the AVM are shown in fig4. There were no significant correlations between clinical/radiological adverse effects and lesion size/dose.

Neuroimages in a 16 year old girl with intraventricular haemorrhage. Left vertebral angiograms (A, B) and T2 weighted MR image (C) before radiosurgery show ruptured AVM in the tectum. T2 weighted MR image (D) obtained 6 months after radiosurgery shows asymptomatic brain stem oedema. Left vertebral angiograms (E, F) and T2 weighted MR image (G) obtained a year after radiosurgery show total obliteration of the AVM and a reversal of the oedema.

Scatter plot of nidus volume v minimum target dose. (A) Patients developing surrounding parenchymal change are indicated with closed circles and patients without parenchymal imaging change are indicated with open squares. (B) Patients developing symptomatic radiation injury are indicated with closed circles and patients without neurological deterioration are indicated with open squares.
HAEMORRHAGE AFTER TREATMENT
During the 126.5 person-years of follow up, five of 29 patients (17.2%) had intracranial haemorrhage from irradiated AVMs (fig 5), yielding a post-treatment annual bleeding rate of 4.0% (95% confidence interval; 0.6%-7.4%). The intervals between the radiosurgery and the haemorrhagic event were 1–92 months (mean 29.4 (SD 40.0 months). Two haemorrhages were seen in the 1st year, one each in the 2nd, 4th, and 8th year after the treatment, resulting in annual bleeding rates of 5.9% for the first 2 years and 2.7% for 3 to 8 years. Among the patients with longer than 3 year follow up, those who received a standard dose had an annual bleeding risk of 1.9%, and those who received a low dose carried a higher rate of 3.2%. Of the five patients who had a haemorrhage, four had had a previous haemorrhage. The outcomes were grave: four patients died of the haemorrhage and one remained unchanged. The actuarial haemorrhage free survival rate was 93.1% in 1 year, 88.9% in 2 years, and 80.8% in 7 years (fig 6). The rate did not correlate with pretreatment haemorrhage, or any clinical characteristics. No patient experienced haemorrhage after total obliteration, with a mean follow up of 33.0 (SD 29.2) months. The overall treatment outcome is summarised in table3.
Neuroimages in a 56 year old man with headache. Left vertebral angiograms (A, B) and T1 weighted MR image (C) before radiosurgery show an AVM in the midbrain. T1 weighted MR image obtained 5 years after radiosurgery (D) shows the residual AVM nidus. CT obtained 8 years after radiosurgery (E) shows fatal bleeding from the AVM.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Probability of haemorrhage free survival after radiosurgery.
Treatment outcomes
Discussion
BRAIN STEM AVMS
Arteriovenous malformations of the brain stem represent only 2%-6% of all cerebral AVMs,6 15-19 but they pose a great management challenge. Several studies have indicated that these AVMs in fact have a high risk of bleeding. About 80%-90% of patients initially presented with an intracranial haemorrhage,6 16 19 20 and the risk of haemorrhage in untreated patients was estimated to be 60% in 10 years.20Unfortunately, there is no solid consensus on the optimal treatment protocols for these lesions at present.21
Many authors reported favourable results with direct surgical excision utilising modern microsurgical techniques, but most of these reports are based on small series involving highly selected cases4 6 11 15 16 or a single case report.22 23 Drake et al 16 reported the surgical results of 15 brain stem AVMs: successful extirpation was achieved in two pial lesions, and four died after surgery. Batjer and Samson15 successfully resected four brain stem AVMs, but one patient died. In the series of Solomon and Stein,6 nine of 12 patients were surgically treated and complete removal was achieved in eight, but the morbidity rate reached 22%. In the recent report of Lowtonet al,4 eight AVMs involving the brain stem were surgically extirpated without significant morbidity. Sisti et al 24reported successful total resection in eight of 11 brain stem AVMs, but the rate remained 50% (3/6) among the cases limited to the intraparenchymal lesions, and two such patients died. Yasargil19 stated in 1993 that parenchymal brain stem AVMs remain beyond the limits of the microsurgical technique. These reports indicate that although pial or subpial lesions can be safely extirpated by surgery, attempts to resect lesions with a parenchymal component lead to high rates of surgical morbidity and a low rate of complete removal. This would not be surprising as the dissection within the brain stem is potentially very hazardous16 and the arterial feeder of the AVMs often also supplies surrounding vital parenchyma as well.6 For similar reasons, state of the art endovascular techniques have not exerted major therapeutic influence either,4 6 19 with few exceptions.25
RADIOSURGERY OF BRAIN STEM AVMS
Currently, stereotactic radiosurgery seems to be the treatment of choice for brain stem AVMs located within the parenchyma. In fact, several gamma knife users have shown that a proportion of patients with “inoperable” brain stem AVM were successfully treated with radiosurgery.1 2 8-10 However, the safety and efficacy of radiosurgery for such AVMs would need further verification. Steineret al 8 briefly mentioned their experience of 57 brain stem AVMs and stated that complete obliteration was confirmed in 20 of 28 patients (71.4%) after a 2 year follow up. However, they did not give clinical characteristics and treatment parameters, or investigate adverse effects caused by the treatment. Duma et al 10 reported their preliminary results of radiosurgery for 28 cases of brain stem AVMs. In their series, the mean volume of the nidus and minimal target dose delivered were 5.4 cm3 and 20.6 Gy. Complete obliteration was attained in seven of eight patients (87.5%) on follow up angiography performed 2 years later. Four patients (14.3%) developed symptomatic radiation injury, of which two (7.1%) had permanent deficit and one (3.6%) died. The dose-volume prescription used in the affected patients was “standard”. Flickingeret al 26 reported that brain stem oedema was “symptomatic” in seven of eight cases (87.5%), and Kondziolka et al 9 stated that they would be hesitant to perform radiosurgery for brain stem AVMs larger than 2.5 cm in diameter. Similar cautions for brain stem radiosurgery have also been given for linac based radiosurgery13 14: in the series of Alexanderet al 13 symptomatic radiation injury was seen in five of six (83.3%) patients with brain stem AVMs; three of which were considered major. These reports suggests that brain stem AVMs have a higher risk of radiation injury than those in other locations, potentially resulting in serious neurological deterioration. Although several risk prediction models are currently available as a guideline for dose selection for AVM radiosurgery,27 28 precise dose-volume limits for brain stem AVMs have not been established.10
ANALYSIS OF PRESENT SERIES
Because the optimal dose is determined on the balance between expected obliteration rates and corresponding risks of radiation injury, knowledge on tolerable doses is essential in planning radiosurgical treatment, especially for lesions located in the eloquent area of the brain. We have shown here that carefully selected patients with small deep parenchymal brain stem AVMs with a parenchymal component less than 2 cm3 in volume could undergo safe and effective radiosurgery using a standard radiosurgical dose (18–20 Gy).
The overall AVM obliteration rate in our series (52.2% at 3 years) was lower than previously published numbers on larger radiosurgical series.1-3 29-31 The most likely reason is that lower doses delivered to the patients during the earlier period were insufficient. In fact, the only factor which affected the rate of obliteration was the minimum target dose, although the analysis of volume effect in our series is limited by the small treated volumes in most cases. This is in agreement with several other studies also showing that the minimum target dose is the most significant factor for the obliteration rate of AVMs.27 32 33 The risk for radiation injury, on the other hand, correlated both with doses and with irradiated volumes.27 28 34-37 Therefore, it is possible that the standard dose of 18–20 Gy could cause unacceptable complications if the volumes of AVMs are ignored, because radiation dose outside the prescribed target volume becomes significant in proportion to the treated volume. This could induce unacceptable symptomatic injury especially in central locations.12 38
In our series, five patients (17.2%) had post-treatment haemorrhages from irradiated but not yet obliterated AVM, four of whom died. This finding confirmed the general consensus that radiosurgery does not reduce the rate of bleeding when the AVMs remain partially obliterated.1 2 39-41 In addition, the significantly higher mortality rate after haemorrhage than found in previous reports probably reflected the critical location of the brain stem AVMs.1 2 9 31 39-41 With such a relatively high bleeding rate and mortality, our current series may still be short of demonstrating a clear benefit of radiosurgery on survival or functional survival. However, the significant rate of complete obliteration of the AVM after standard dose radiosurgery, in combination with the fact that no bleeding was seen from completely obliterated AVMs, should justify the radiosurgical treatment of brain stem AVMs. Although further studies with larger series and longer follow up are needed to confirm this more clearly, our present study adds a valuable contribution to the knowledge on the dose and treatment volume prescription for brain stem AVMs.
In summary, our results presented here are in favour of the notion that radiosurgery should be the treatment of choice for patients with intraparenchymal brain stem AVMs, in which standard radiosurgical doses can be delivered if the intraparenchymal nidus volume is sufficiently small. However, post-treatment haemorrhage remains a significant problem of this technique as this is associated with a high mortality rate.
Acknowledgments
We are grateful to Dr Hiroshi Abe, Department of Neurosurgery, Brain Research Institute, Niigata University, and Dr Takafumi Ide, Department of Neurosurgery, Tokyo Metropolitan Bokuto Hospital, for providing the radiographic data. This work was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Science, and Culture of Japan.
References
Linked Articles
- Editorial commentary