Article Text

Abstract
Early neurological deterioration (END) following ischaemic stroke is a serious event with manageable causes in only a fraction of patients. The incidence, causes and predictors of END occurring within 24 h of acute ischaemic stroke (END24) have not been systematically reviewed. We systematically reviewed Medline and Embase from January 1990 to April 2013 for all studies on END24 following acute ischaemic stroke (<8 h from onset). We recorded the incidence and presumed causes of and factors associated with END24. Thirty-six studies were included. Depending on the definition used, the incidence of END24 markedly varied among studies. Using the most widely used change in National Institutes of Health Stroke Scale ≥4 definition, the pooled incidence was 13.8% following thrombolysis, ascribed to intracranial haemorrhage and malignant oedema each in ∼20% of these. As other mechanisms were rarely reported, in the majority no clear cause was identified. Few data on END24 occurring in non-thrombolysed patients were available. Across thrombolysed and non-thrombolysed samples, the strongest and most consistent admission predictors were hyperglycaemia, no prior aspirin use, prior transient ischaemic attacks, proximal arterial occlusion and presence of early CT changes, and the most consistent 24 h follow-up associated factors were no recanalisation/reocclusion, large infarcts and intracranial haemorrhage. Finally, END24 was strongly predictive of poor outcome. The above findings are discussed with emphasis on END without a clear mechanism. Data on incidence and predictors of the latter subtype is scarce, and future studies using systematic imaging protocols should address its underlying pathophysiology. This may in turn lead to rational preventative and therapeutic measures for this ominous event.
- Stroke
- Systematic Reviews
- MRI
Statistics from Altmetric.com
Introduction
Following licensing of intravenous recombinant tissue-type plasminogen activator (IV-rtPA), the management of acute ischaemic stroke (AIS) has experienced a shift towards the hyperacute stage, and patients increasingly undergo reperfusion therapy. Currently, most patients with AIS, whether they receive IV-rtPA or not, are admitted to acute stroke units for prevention and monitoring of early complications. Although the majority of patients tends to improve over the subsequent 24–72 h, a sizeable fraction does not substantially recover or even deteriorates, so-called early neurological deterioration (END).1 Current estimates of incidence of END after AIS vary widely, from 5% to 40%,2–8 depending on the definition used (ie, type of stroke scales and time frame used for the deterioration), but regardless of the definition used END is consistently associated with poor 3-month clinical outcome.9 Major causes of END include symptomatic intracranial haemorrhage (sICH) and malignant vasogenic oedema.9 Therefore, preventing END and, if it occurs, treating its underlying mechanism, is an important challenge towards improving stroke outcome.
Apart from sICH, malignant oedema and some additional unusual causes leading to specific management according to published—though not always standardised—guidelines, around a half of all ENDs may have no clear mechanism and are often referred to as ‘stroke progression’.10 Accordingly, no specific management is recommended in this situation, and no clear action is usually taken to try and revert the deficit and hence prevent poor outcomes. Despite the rapidly growing literature on END in general, with the number of articles on END more than doubling every decade since 1990, its exact incidence and the mechanisms underlying END without clear cause, particularly when occurring soon after IV-rtPA, are still largely unknown.
We present here a systematic review on the incidence and mechanisms of, and factors associated with END in AIS candidates for IV-rtPA. Given the current emphasis on the first 24 h1 and the rapidly increasing use of reperfusion therapies, we will restrict the present review to END occurring within this timeframe (to be referred to as END24 below). Malignant oedema, which tends to develop later,11 is consequently largely outside the focus of this review. The few studies following endovascular therapy are also excluded from this review, given that in this situation the END may be related to the procedure itself. Despite the high clinical relevance of END, currently available reviews on END following AIS are not systematic and have not focussed on END24.12–14
Following presentation of the data derived from this systematic review, the discussion will address some pathophysiological implications, with particular emphasis on the putative mechanisms underlying END without clear cause.
Methods
Selection criteria and search strategy
Studies were eligible for this review if they: (1) included patients with ischaemic stroke in the hyperacute phase (<8 h from onset), regardless of vascular territory or underlying mechanism; (2) considered END as any degree of deterioration during the first 24 h following hospital admission; and (3) were published in English language. Studies that reported only on patients treated endovascularly or did not separate intravenously treated and endovascularly treated groups were excluded, as were also those exclusively focused on sICH. Using MEDLINE and EMBASE, we sought articles published between 1 January 1990 and 14 April 2013, using the terms detailed in online supplementary table S1. We also hand-searched the reference lists of all included articles and reviews. The flow diagram, numbers of studies screened, assessed for eligibility, and included in the review, was performed according to Preferred Reporting Items for Systematic reviews and Meta- Analyses (PRISMA) guidelines (see online supplementary figure S1).15
Data extraction and statistical analysis
Using a standardised form, one reader (PS) extracted all relevant data from the selected articles. For each study, incidence estimate of END24 was calculated using raw data, and the 95% CI around this estimate was calculated using the Wald (asymptotic) method. Heterogeneity across studies was assessed using Cochran's Q and the I2 statistics. As appropriate, fixed-effects or random-effects pooled prevalence of END24 were separately calculated in studies of thrombolysed and non-thrombolysed patients.16 ,17 Publication bias regarding the meta-analysis of END24 in IV-rtPA treated patients was investigated using a funnel plot, with END24 incidence as y axis and sample size as x axis. OR and 95% CI of factors associated with END24 were recorded (or calculated from tables), when available. When a study provided unadjusted and adjusted OR, we recorded the adjusted OR. When two or more articles from the same group evidently used the same or expanded cohort (‘overlapping studies’), we considered for further analysis only the article reporting the largest sample; for the sake of completeness, however, the studies are all listed in our tables. Statistical analysis was performed using SAS V.9.3 (SAS, Cary, North Carolina, USA).
Results
Among 2870 records identified through database searching, 36 were included in this review (see online supplementary figure S1).1 ,18–52 The characteristics of the included studies are summarised in online supplementary table S2. Twenty-six studies focused on IV-rtPA treated patients, five on non-thrombolysed patients, and five were randomised controlled trials of IV-rtPA versus placebo. Of these 36 studies, 6 appeared in the 1990 s, 20 in the 2000s and 10 since 2010.
Incidence of END24
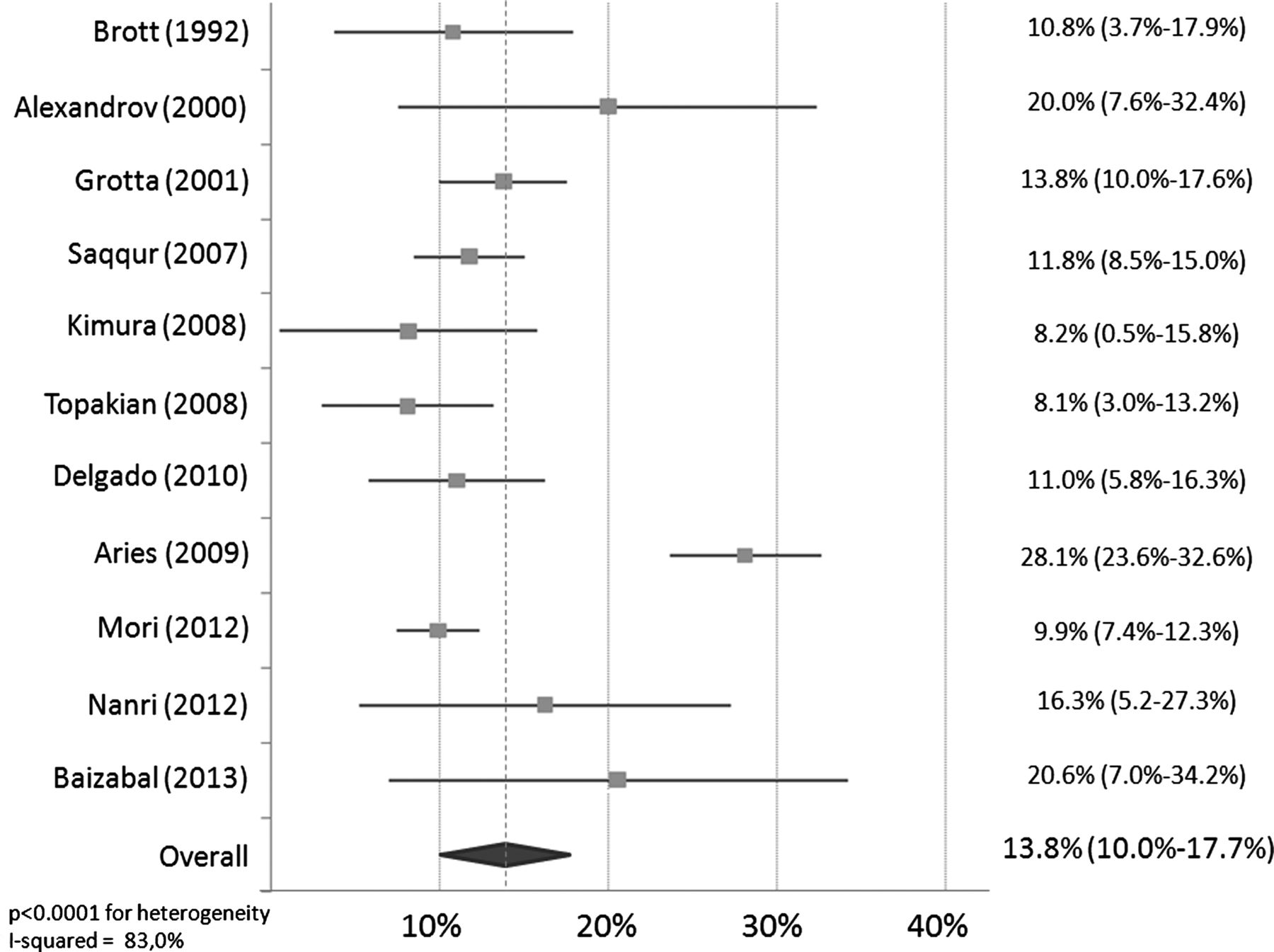
Across studies, nine different definitions of END24 were used, applying variable neurological scale and degree of deterioration (see online supplementary table S2). The reported incidence of END24 also varied widely, from 2.2% to 37.5%. However, the majority of studies (24/36) on END24 used a deterioration of four points on National Institutes of Health Stroke Scale (ΔNIHSS ≥4), particularly in recent years. Considering the 11 studies on IV-rtPA treated patients that used this definition (and excluding overlapping studies), the random-effects pooled incidence of END24 was 13.8% (95% CI 10.0% to 17.7%, I2=83%, Q=59.0, p<0.0001 for heterogeneity; table 1 and figure 1). The funnel plot did not suggest evidence of publication bias regarding this meta-analysis (see online supplementary figure S2). Regarding non-thrombolysed AIS, only six studies were available (table 2), and the definition of END24 used varied widely. Accordingly, the incidence of END24 ranged from 13.3% to 36.8%. However, its incidence was similar in the two studies that used the ΔNIHSS ≥4 definition (16.3% and 17.6%, respectively).
Incidence of END24 in non-overlapping studies of AIS treated by IV-rtPA, using ΔNIHSS ≥4 definition
Incidence of END24 in non-thrombolysed patients with AIS
{kind=link}
Random-effects pooled incidence of END24 in IV-rtPA treated patients, using ΔNIHSS ≥4 definition. END24, early neurological deterioration within 24 h of acute ischaemic stroke; IV-rtPA, intravenous recombinant tissue-type plasminogen activator; NIHSS, National Institutes of Health Stroke Scale.
Reported causes of END24
In the 11 studies on IV-rtPA treated patients, the cause for the deterioration was rarely specified, except for sICH which was specified in 8 studies. The fixed-effects pooled incidence of sICH among patients with END24 was 21.4% (95% CI 15.6% to 27.1%, I2=22%, Q=9.0, p=0.25 for heterogeneity). Only few of the included studies reported causes other than sICH. Of these, the most frequently cited were malignant oedema, accounting from 14% to 27% of all END24 causes,23 ,45 ,48 ,52 and early recurrent ischaemic stroke (so-called ERIS35 ,47), which accounted from 0.6% to 1.8% of all patients with acute strokes in two large studies (228–341 patients),35 ,47 excluding one potential outlier of 2.9% in a very small study of 34 patients.52 Thus, even after taking into account sICH, malignant oedema and ERIS, a large fraction of END24 had no reported cause.
Regarding the underlying cause of END24 in non-thrombolysed patients, apart from one early study that used heparin therapy, the incidence of sICH in the two studies where it is reported was 3.6% and 7.1% of patients with END24. There is no data on other potential causes of END24.
Associated factors
Eighteen studies found at least one baseline or post-treatment variable significantly associated with END24 (table 3). Main admission clinical and radiological factors predicting END24 included high blood glucose level, older age, higher or lower NIHSS score, a history of diabetes, coronary heart disease, transient ischaemic attack or non-use of aspirin, longer admission delay, evidence of proximal arterial occlusion on CT or magnetic resonance angiography (MRA), presence of early ischaemic changes on CT, and larger diffusion-weighted imaging (DWI) lesion volume. Radiological factors associated with END24 at 24-h follow-up imaging included evidence of no-recanalisation, reocclusion, sICH, brain swelling, and presence of infarction >1/3 of the middle cerebral artery (MCA) territory.
Baseline and 24-h factors associated with END24
Regardless of the definition used for END24, death or dependency at 3 months was >fourfold higher in patients with END24 than in non-END24 in all three articles reporting this association (table 4). One study reported that END24 independently predicted poor outcome in multivariate analysis.50
Association between END24 and 3 month outcome
Discussion
The main findings from this review that focused on END24 following AIS will be addressed first, including definition, incidence and causes, and relationships with outcome. The main clinical, laboratory and radiological factors found to be significantly associated with END24 will then be addressed in sequence, together with some of the pathophysiological implications.
Definition of END24
Across the reviewed studies, the definition used for END24 has been inconsistent with respect to severity and time frame of the deterioration, which likely in part explains the wide range in reported incidence. An appropriate definition of END should allow one to detect functionally meaningful changes in neurological status at the bedside, in an easy and reliable fashion. The ΔNIHSS ≥4 criterion has been used in most studies so far, particularly in recent publications, and almost exclusively so for early (ie, ≤24 h) deterioration, because it seems clinically relevant and because the NIHSS is the most widely used neurological scale in the acute stroke setting.54 However, some limitations of this scale need to be raised regarding the clinical relevance of END assessment. First, although the intrarater and inter-rater reliability for individual NIHSS items is good, the overall score may have more substantial variability.55 Therefore, a small change in total NIHSS score (eg, ΔNIHSS ≥2) might reflect inadequate reliability rather than true END, notably with high scores (ie, severe stroke). Second, the NIHSS is highly skewed in its functional significance, and a lower than 4 points deterioration could still be functionally meaningful, for example, in the context of minor stroke.9 ,56 Thus, using relative or normalised instead of absolute deterioration,1 such as percentage change from admission NIHSS, might have increased clinical relevance, since an event qualifying as END would refer to larger NIHSS increases for high than for low baseline scores. However, these approaches have been scarcely used and might have their own limitations, including poor bedside practicality. Third, and lastly, the NIHSS is considerably weighted to motor dysfunction, while some non-motor yet important functions such as neglect are underweighted.57 For instance, a functionally severe worsening of neglect may be counted as 2 points only, which would not qualify as END using the ΔNIHSS ≥4 definition.
Incidence of END24
Across studies, and not unexpectedly given the various definitions used, the incidence of END24 varies widely, from 2.2% to 37.5%. When focusing on the most widely used ΔNIHSS ≥4 definition, the reported incidence is much narrower, specifically 8.1–28.1% and 16.3–17.6% after IV-rtPA and in non-thrombolysed patients, respectively. Overall, therefore, END24 does not seem to be a rare event, occurring in about one in seven thrombolysed patients, and one in six non-thrombolysed patients.
Causes of END24
Symptomatic intracranial haemorrhage
Apart from sICH, few studies have reported on other causes of END24. Overall, based on the studies reviewed here, which included two large phase III trials testing IV-rtPA versus placebo, sICH explained about 20% of END24 in thrombolysed patients, and about 5% in non-thrombolysed patients. Despite this expected much lower incidence of sICH in non-thrombolysed patients, the overall incidence of END24 appears higher than in thrombolysed patients, suggesting that other causes may be more frequent in this setting.
Malignant oedema
Malignant oedema as a cause of END24 was reported in a few studies only. Its reported incidence among all END24 ranged from 14% to 27%, representing ∼2–3% of the total AIS sample. Considering its time course,11 this complication is expected to account for more later-occurrence END. This assumption would be supported by the reported total incidence of 6.5% fatal brain swelling in a large cohort of anterior circulation strokes.58
Early recurrent ischaemic stroke
ERIS is defined as clinical and imaging evidence of ischaemic stroke in an independent arterial territory (ie, new deficits explainable by arterial reocclusion or thrombus extension are excluded from this definition).35 ,47 It appears to be a rare cause of END24, occurring in 0.6% and 1.8% patients only in two large cohorts of thrombolysed AIS.35 ,47 Its assumed pathophysiology is a new embolic event due to IV-tPA-induced fragmentation of pre-existing intracardiac or arterial thrombus. This interpretation is consistent with its exclusive occurrence during or in the early minutes following IV-rtPA in the above large studies. Although this hypothesis remains unproven since echocardiography prior to IV-rtPA infusion was not performed in these studies, atrial fibrillation was effectively considered the cause of the stroke in several patients. It is important to emphasise the ominous significance of ERIS since in the above studies death occurred in 100% of the cases within days following the deterioration.
Early seizures
Although no study identified by this review reported early seizures as the cause of END24, this event is likely under-reported. In a large cohort of patients with AIS treated with endovascular therapy, the incidence of seizures within 24 h was 3.2% and independently predicted poor outcome.59 However, the actual occurrence of END was not reported.
END without clear mechanism
Based on the above estimates of sICH, malignant oedema, ERIS and early seizures, around half of END24 occurring after IV-rtPA—and perhaps even more in non-thrombolysed patients—seem to have no immediately identifiable mechanism. Although this END subtype is sometimes referred to as ‘stroke progression’,10 this default clinical category does not imply a definable mechanism. No clear management guidelines are currently available regarding patients falling into this category, nor regarding how to prevent this complication.
One likely hypothesis to account for END without clear mechanism is an extension of symptomatic ischaemic tissue (infarct core or ischaemic penumbra) into ‘asymptomatic tissue’ (ie, oligaemia or non-hypoperfused tissue).12 This hypothesis is supported by a recent study showing that infarction of ‘non-core-non-penumbral’ tissue occurs not infrequently following AIS, being of substantial volume in ∼10% of patients, and is associated with reduced 1-month clinical recovery.60 Although the authors discussed the potential relevance of their observation to END, the actual relation to END was not reported. Two recent studies pointed to the occurrence of ‘new DWI lesions’ at day 7 post stroke, involving areas initially affected by only mild (non-penumbral) hypoperfusion61 or ‘outside the area of hypoperfusion’ (no further detail provided).62 However, neither study even mentioned END.
Admission factors associated with END24
Clinical admission factors
Hyperglycaemia was found associated with END24 in three studies,23 ,30 ,50 whereas four did not find this association (although there was a trend in one).27 ,37 ,40 ,48 In the three studies reporting an association, two adjusted for history of diabetes mellitus, and higher glucose level still predicted END24 in one of these.50 It therefore seems likely that hyperglycaemia facilitates, albeit does not directly cause, END24. One potential mechanism could be that it increases blood-brain barrier disruption and promotes sICH.63 ,64 However, hyperglycaemia might also facilitate neuronal damage. For instance, in one study acute hyperglycaemia increased brain lactate production and appeared to facilitate conversion of severely hypoperfused at-risk tissue into infarction, which may adversely affect stroke outcome.65 In turn, it could also facilitate conversion of asymptomatic into symptomatic tissue, and even potentially infarction, without necessarily reducing perfusion. Against this scenario, in a randomised trial insulin therapy did not hamper infarct growth relative to placebo, even though it significantly reduced blood glucose and attenuated brain lactate increases.66 In addition, that lactate itself is toxic to the ischaemic brain remains debated, with contrary evidence suggesting it is used as alternative energetic fuel and may in fact be beneficial.67 Hyperglycaemia also has prothrombotic effects,68 and could therefore facilitate thrombus extension, which is a strong underlying hypothesis for END24. In addition, diabetic microangiopathy may alter cerebral autoregulation and affect the collateral circulation,69 making affected patients more sensitive to variations in blood pressure and thereby increasing the risk of deepening and extension of hypoperfusion. Finally, even though not mentioned in the studies on END24 identified in this review, episodes of hypoglycaemia following insulin therapy for hyperglycaemic state may contribute to END24 via neuronal death in the penumbra and oligaemia. Two trials reported larger infarct growth in intensive insulin compared with placebo-treated or standard care groups, mainly in patients with proximal occlusion66 or no-recanalisation,70 and in both studies, episodes of hypoglycaemia were more frequent in insulin-treated patients.66 ,70 Moreover, there is preclinical evidence of greater infarct growth with hypoglycaemia <3 mmol/L.71
Prior use of aspirin (before stroke onset) was found in one large study to independently protect against occurrence of END24.27 However, this association was not found in another study,40 nor in a third that considered all antithrombotics together.50 Interestingly, in the former study,27 sICH explained 14% of all END24 cases. That sICH is facilitated by aspirin therapy72 further strengthens the link between prior use of aspirin and reduced risk of END24 from other causes. Prior use of aspirin was also a strong independent predictor of non-occurrence of END in one study using a wider time frame for the deterioration.73 Possible mechanisms underlying this protective effect include prevention from thrombus extension and/or new embolisation (eg, from an unstable plaque). In support of this hypothesis, progression of occlusion or new occlusion of collateral pathways was found in 12/15 patients with END (not restricted to the first 24 h),74 although aspirin is not reported in this early study. Another possible mechanism to explain the protective role of aspirin could be via prevention of reocclusion following initial recanalisation, an event documented by transcranial Doppler (TCD) in subjects who deteriorate following initial improvement.29 ,34 However, depending on the amount of initial improvement, this scenario may,37 or not, cause proper END24.
Admission blood pressure,23 ,27 ,33 ,37 ,40 ,48 ,50 its variation over the first 24 h23 ,27 or the intravenous use of antihypertensives before22 ,50 or after22 ,27 thrombolysis have not been found to significantly predict END24. Although blood pressure drops may play an important role in the specific situation of END24 without clear cause, particularly in patients with extensive oligaemia due to proximal occlusion,12 this hypothesis has not been directly tested so far.
Only one study included in this review assessed the association between body temperature and END24, and found none.23 This finding from a single report contrasts with numerous previous reports of a strong association between admission hyperthermia or proinflammatory markers and END occurring beyond 24 h, whose underlying mechanisms might however be partly different.14 Regarding oxygen saturation, another physiological variable that may play a role in END by increasing neuronal death in the oligaemia,12 we found no study that assessed its relationship with END24.
Severe neurological impairment at admission was a significant predictor of END24 in two studies.41 ,49 However, both used a liberal definition of END24 (worsening of Scandinavian Stroke Scale, which might be more sensitive than NIHSS,75 and ΔNIHSS ≥1, respectively). Furthermore, since a severe neurological deficit strongly predicts sICH72 and malignant oedema,76 these causes of END24 may explain this finding. In contrast, a third study50 using a more conservative definition (namely, ΔNIHSS ≥4) found the inverse association, that is, less severe deficits predicted END24, which may be explained by a ‘ceiling effect’ such that higher admission scores are less likely to further increase. Thus, the risk of END24 associated with admission NIHSS may depend on the definition of END, including whether absolute or relative changes are considered.
Stroke aetiology has never been reported as a significant predictor of END24.25 ,37 ,50 However, in one study only proximal arterial occlusions on TCD were studied,37 and in another the patients were only categorised as ‘cardioembolic’ versus the rest. In the third,25 which focused on non-thrombolysed mild strokes, the incidence of END24 was 9% in lacunar infarcts as compared with 31% and 23% in large atherosclerosis and cardioembolic strokes, respectively, a non-significant difference. This may appear to contradict the widely held belief that lacunar strokes are more prone to develop END24, and the information available regarding END occurring at later time points does not support this idea either.3 ,7 ,77–79 Since this stroke subtype is mainly caused by single perforator disease, the mechanisms of underlying END may differ from other subtypes, yet remain largely unknown.80
Admission radiological factors
Proximal arterial occlusion was observed more frequently in patients with END24 in three studies of thrombolysed AIS,23 ,36 ,50 and any arterial occlusion/stenosis in one study on non-thrombolysed patients,25 whereas this association was not found in another.37 One possible explanation for this association would posit that proximal occlusion predicts stroke severity, and therefore also END24 through its association with sICH and malignant oedema.72 ,76 However, since this association was also observed in three studies on minor stroke4 ,7 ,25 (assessing END in a >24 h time frame for two of them4 ,7), an alternative or additional explanation could be that proximal occlusion increases the risk of further extension of penumbral tissue and hence infarction. This idea would be supported by the fact that proximal occlusions entail a larger volume of symptomatic and asymptomatic hypoperfused tissue.81
Regarding early ischaemic signs, they were reported as predictors of END24 in three CT studies including the NINDS IV-rtPA study23 ,27 ,43 as well as one DWI study,41 possibly reflecting their association with malignant oedema and sICH.72 ,76 However, reanalysis of the NINDS imaging dataset did not reproduce the original finding,28 perhaps because the hyperdense MCA sign was lumped together with parenchymal early signs in the initial analysis.
Although collateral status might be another independent predictor of END24, this association has not been looked at so far. Two studies using wider time frames for END found an association with poor collaterals,5 ,21 and another reported that impaired cerebral haemodynamic reserve on TCD predicted END.82 However, it is possible that in the earlier time frame, better collaterals are associated with increased risk of unexplained END24, through larger volumes of oligaemia.83
Radiological factors at 24 h
Among the 24-h follow-up imaging factors studied, no-recanalisation, arterial reocclusion, sICH, brain swelling and large MCA infarcts were found to be associated with END24, but the latter three directly reflect sICH and malignant oedema. No-recanalisation23 ,39 was significantly associated with END24 in two studies, although not in an independent fashion, except in another study on reocclusion.37 This association would be explained by the persistence of tissue hypoperfusion in turn favouring END without clear cause.
Conclusion
END occurring within 24 h of AIS is not rare, is predictive of poor 3-month outcome and has no clear cause in the majority of patients. Although the reported associated factors detailed above point to specific underlying mechanisms for END without clear cause, the available data is too scarce to make any definitive statement. Further work using rigorous operational and clinically relevant definitions is required to further determine the exact incidence, apparent mechanisms and underlying pathophysiology of END without clear cause, in thrombolysed and non-thrombolysed patients. These studies will also need to prospectively assess the vascular as well as perfusional status at baseline and at time of neurological worsening. This may in turn lead to accurate prediction as well as rational preventative and therapeutic measures for this category of END, particularly in the post-IV t-PA setting, such as earlier introduction of antiplatelet agents than currently recommended (namely, 24 h), and evaluation of early ‘bridging’ endovascular therapy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
- Data supplement 2 - Online tables
Footnotes
-
Contributors PS: conception, data retrieval, data analysis, manuscript writing. GT: conception, data analysis, manuscript writing. CO: manuscript editing. J-CB: conception, manuscript writing.
-
Funding PS is funded by la Fondation pour la Recherche Médicale (FRM).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.