
Abstract
BACKGROUND: The efficacy of combined aspiration catheter and stent retriever compared with stent retriever alone for the treatment of large-vessel occlusion acute ischemic stroke is unclear.
PURPOSE: Our aim was to conduct a systematic literature review and meta-analysis on several metrics of efficacy comparing aspiration catheter and stent retriever with stent retriever alone.
DATA SOURCES: MEDLINE and the Cochrane Library Databases were searched. Randomized controlled trials and case-control and cohort studies were included.
STUDY SELECTION: Ten comparative studies were included detailing a combined 1495 patients with aspiration catheter and stent retriever and 1864 with stent retrievers alone.
DATA ANALYSIS: Data on first pass effect (TICI 2b/2c/3 after first pass), final successful reperfusion (modified TICI ≥2b), and 90-day functional independence (mRS ≤ 2) were collected. Meta-analysis was performed using a random-effects model.
DATA SYNTHESIS: There was a pooled composite first pass effect of 40.8% (611/1495) versus 32.6% (608/1864) for aspiration catheter and stent retriever and stent retriever alone, respectively (P < .0001). Similarly, on a meta-analysis, aspiration catheter and stent retriever were associated with a higher first pass effect compared with stent retriever alone (OR = 1.63; 95% CI, 1.20–2.21; P = .002; I2 = 72%). There was no significant difference in composite rates of successful reperfusion between aspiration catheter and stent retriever (72.8%, 867/1190) and stent retriever alone (70.8%, 931/1314) (P = .27) or on meta-analysis (OR = 1.31; CI, 0.81–2.12; P = .27; I2 = 82%). No difference was found between aspiration catheter and stent retriever and stent retriever alone on 90-day functional independence (OR = 1.02; 95% CI, 0.77–1.36; P = .88; I2 = 40%).
LIMITATIONS: This study is limited by high interstudy heterogeneity.
CONCLUSIONS: On meta-analysis, aspiration catheter and stent retriever are associated with a superior first pass effect compared with stent retriever alone, but they are not associated with statistically different final reperfusion or functional independence.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- ASR
- combined aspiration catheter and stent retriever
- BGC
- balloon-guide catheter
- eTICI
- expanded TICI
- mTICI
- modified TICI
- FPE
- first pass effect
- LVO
- large-vessel occlusion
- SR
- stent retriever
There are several different techniques used for the endovascular treatment of acute ischemic stroke (AIS) secondary to large-vessel occlusion (LVO), including mechanical thrombectomy via a stent retriever (SR), direct contact aspiration using a large-bore intermediate catheter, and a combined approach using a contact aspiration catheter with a stent retriever (ASR). SR is a well-established, safe technique for AIS and often results in high rates of successful recanalization.1 Similarly, contact aspiration is a commonly used technique. The Contact Aspiration vs Stent Retriever for Successful Revascularization (ASTER) trial compared contact aspiration with SR alone and found no significant difference in final reperfusion or first pass effect (FPE) between the 2 methods.2 FPE is an increasingly used metric, expressed as the achievement of complete recanalization with a single use/pass of a thrombectomy device.3
Recent studies have also investigated the efficacy of ASR, which theoretically should synergize the positive thromboembolic retrieval mechanisms of SR and contact aspiration. However, results have been mixed. While some studies have shown that ASR results in superior technical and clinical outcomes,4⇓-6 other studies have shown no such benefits.7⇓-9 The recently completed Combined Use of Contact Aspiration and the Stent Retriever Technique Versus Stent Retriever Alone for Recanalisation in Acute Cerebral Infarction (ASTER2) trial compared ASR with SR and found no difference in the final reperfusion, but multiple secondary reperfusion end points favored ASR.9 Thus, the efficacy of ASR compared with SR alone is unclear. The aim of this study was to complete a systematic literature review and meta-analysis to better evaluate how ASR compares with SR in LVO AIS.
MATERIALS AND METHODS
Literature Search and Eligibility Criteria
A Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA)–guided systematic literature review and meta-analysis was conducted to investigate the efficacy of primary ASR verses SR alone for the treatment of LVO AIS. Institutional review board approval was not required because the data were obtained from already published studies and are publicly obtainable.
The MEDLINE and Cochrane Databases were searched up to September 2021 using the following search terms: “Aspiration Catheter” AND “Mechanical Thrombectomy” AND “Stroke,” “Aspiration Catheter” AND “Stent Retriever” AND “Stroke,” “Aspiration” AND “Stent Retriever” AND “Stroke,” “Aspiration” AND “Mechanical Thrombectomy” AND “Stroke.” The MEDLINE software removed duplicated studies between queries; results from the Cochrane Database were cross-referenced with the MEDLINE results, and duplicates were excluded. Only comparative studies with internal controls were included in this analysis (eg, directly compared efficacy metrics of ASR and SR within same study cohort). Each study from the literature search was screened on the basis of the title alone or abstract, with further reading of the article if there was uncertainty about preliminary inclusion. Studies had to be written in English for inclusion and to include >18 patients within the cohort. Both randomized controlled trials and observational studies were included in the quantitative synthesis. For inclusion, studies had to describe the use of primary combined aspiration catheter and stent retriever as a treatment technique; those that used adjunct aspiration/or SR as a rescue therapy were not included in this analysis. Similarly, for the SR studies, SR had to be used as a primary technique. After the initial screening process, all of the studies were more rigorously assessed for possible final inclusion by 2 independent reviewers for confirmation of data with disagreements settled by consensus. Inclusion of at least one of the main outcome measures described below was an additional requirement for inclusion in the meta-analysis.
Outcome Measures
Three primary outcome measures were evaluated to compare the efficacy of ASR and SR alone for ischemic stroke of the anterior circulation. FPE was measured on the basis of the internal metric for a successful first pass as dictated for each individual study, which included expanded TICI (eTICI) ≥2b, eTICI ≥2c, or modified TICI (mTICI) 3 only. For the sake of this study, FPE also included modified FPE (eg, achieved mTICI 2b after the first pass) if that was what was reported as FPE in the study. In other words, some studies described modified FPE or the equivalent (eg, “successful reperfusion”) as an eTICI ≥2b, while in other studies, only mTICI 2c/3 cases were considered a successful first pass. However, because they were internally controlled, both types were included in the FPE analysis. The final TICI score following endovascular intervention was used as a surrogate for successful reperfusion. Studies had to describe a final TICI score of either eTICI ≥2c or mTICI ≥2b, and both were grouped and included in the successful reperfusion analysis. All studies had to delineate the exact TICI score for inclusion in this analysis and the FPE analysis. Ninety-day functional independence (mRS 0–2) was also investigated as a primary outcome. A study had to detail at least one of these outcome measures to be included in the quantitative synthesis. Subgroup analyses based on the TICI definition of the primary outcome measures of FPE and successful reperfusion were also completed. Studies that defined an outcome measure by TICI 3 and mTICI 2c/3 scores were grouped together, whereas those that defined an outcome with mTICI ≥2b were grouped together. Last, a secondary composite outcome measure included the 90-day mortality rate.
Results Synthesis and Statistical Analysis
Forest plots for each of the primary outcome measures of FPE, successful reperfusion, and 90-day functional independence were constructed with corresponding ORs. A random-effects model was used to calculate the pooled OR for each analysis using a Mantel and Haenszel method. All forest plots and corresponding statistical analyses including tests of heterogeneity were calculated using Review Manager (RevMan computer program, Version 5.4; https://review-manager.software.informer.com/5.4/). A χ2 test (completed using GraphPad Prism 9 software; GraphPad Software) was used to assess statistical significance for overall composite differences in efficacy rates and secondary outcome measures.
Bias and Heterogeneity Assessments
Statistical heterogeneity was assessed using the Cochran Q statistic and described using the I2 measure and P value. An I2 of >50% and >75% was used as a benchmark for moderate and considerable heterogeneity, respectively. A heterogeneity P value > .10 was used to indicate statistically nonsignificant heterogeneity. An assessment of potential publication bias was also completed for each analysis using funnel plots and the Egger test, implemented using MedCalc statistical software (https://www.medcalc.org). An Egger test P value < .10 was used to indicate significant publication bias.
RESULTS
Systematic Literature Search
From MEDLINE and Cochrane Databases, 484 studies resulted from our search after the removal of duplicates. Two articles were found on the basis of screening references based on a supplementary literature review. Fourteen articles that potentially met the full inclusion criteria were more rigorously assessed. Four of these articles were eventually not included for the following reasons: One study did not adequately specify the TICI score from those treated, 2 studies had <18 patients in each treatment arm, and 1 study described only M2 occlusions and not LVO. As a result, 10 studies describing a total of 1495 patients having undergone ASR and 1864 having undergone SR met the final inclusion criteria for the quantitative synthesis (Fig 1).4⇓⇓⇓⇓⇓⇓⇓⇓-13 Of these studies, 1 was a multicenter randomized controlled trial, 1 was a multicenter prospective registry study, 4 were single-center retrospective studies, 1 was a single-center prospective study, and 3 were multicenter retrospective studies. A review of the characteristics of the included studies can be seen in the Table.
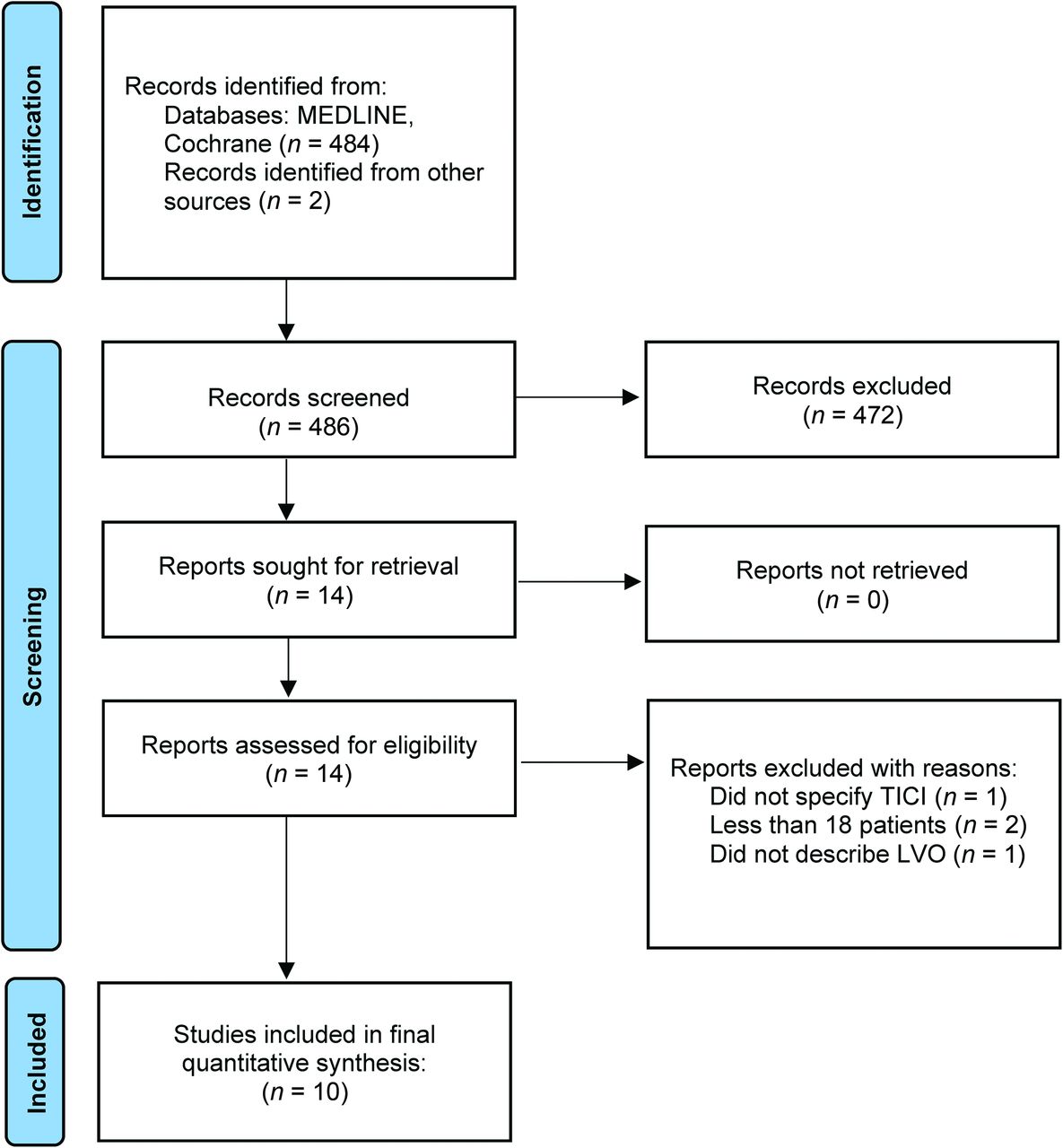
PRISMA literature review flow diagram.
Characteristics of studies included within quantitative synthesis
Meta-analysis
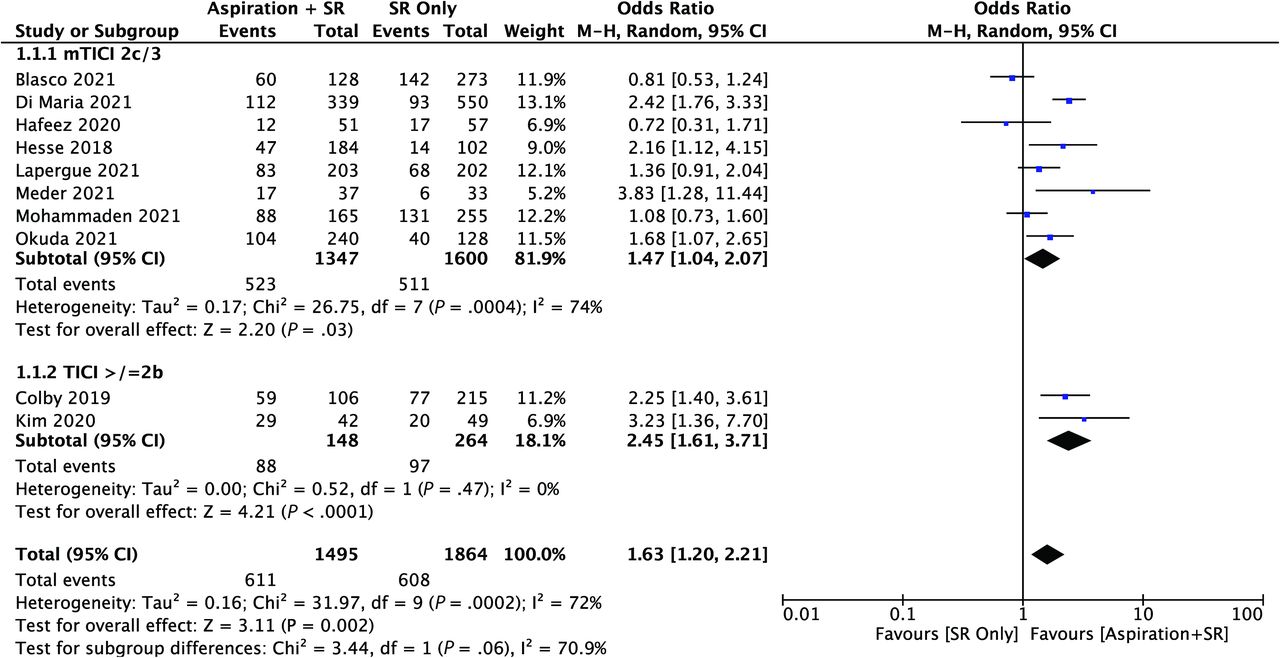
From the 10 included comparative studies, there were 1495 patients having undergone ASR and 1864 having undergone SR. The criteria for FPE were achievement of mTICI 2c/3 in 8 studies, and in 2 studies, it was defined as TICI ≥2b. Regarding FPE results, the pooled composite rates were 40.8% (611/1495) versus 32.6% (608/1864) for ASR and SR, respectively (P < .0001). On meta-analysis, primary ASR was also associated with a higher FPE compared with primary SR (OR = 1.63; 95% CI, 1.20–2.21; P = .002) (Fig 2). A subgroup analysis was completed on the basis of TICI criteria and the FPE definition. Both the mTICI 2c/3 subgroup (8 studies, 2947 patients) and the TICI ≥2b subgroup (2 studies, 412 patients) significantly favored ASR over SR with an OR of 1.47 (95% CI, 1.04–2.07; P = .03) and 1.63 (95% CI, 1.20–2.21; P < .0001), respectively (Fig 2).
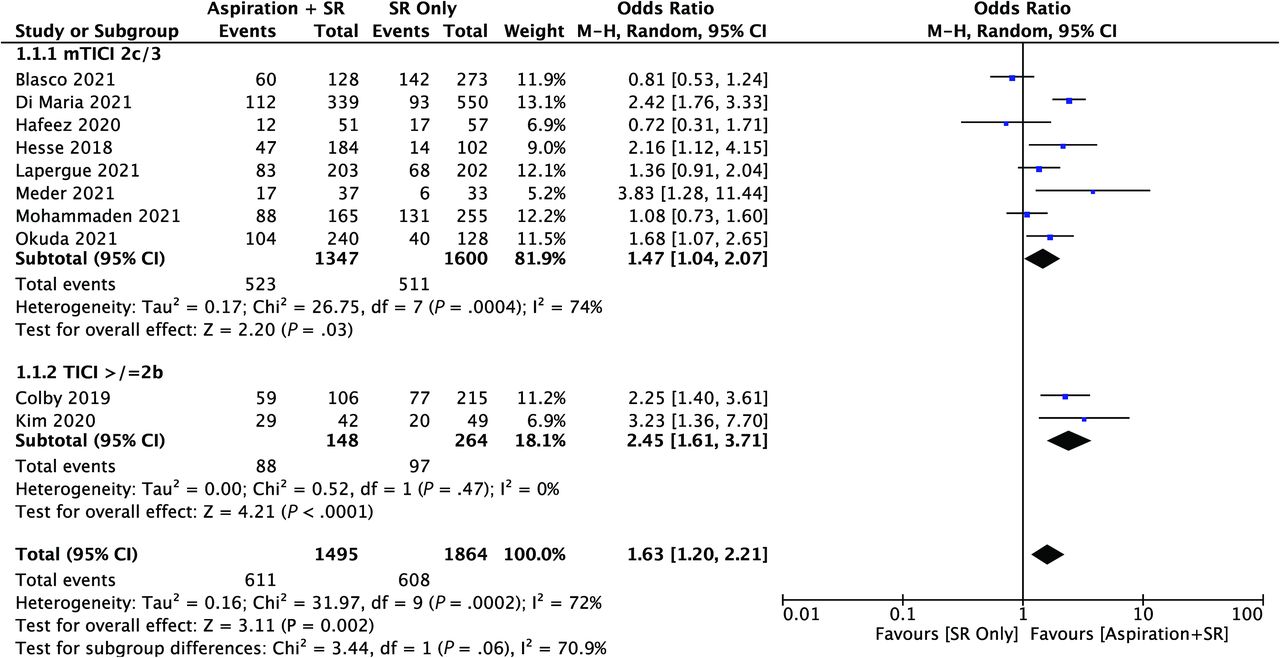
Forest plot for FPE analysis. M-H indicates Mantel and Haenszel.
Successful final reperfusion was defined as mTICI ≥2b in 7/9 (1698 patients) of the included studies, and as mTICI 2c/3 in the other 2/9 studies (806 patients). There was no significant difference in composite rates between ASR (72.8%, 867/1190) and SR (70.8%, 931/1314) (P = .27) regarding successful reperfusion. This was similarly the case on a meta-analysis comparing ASR and SR (OR = 1.31; 95% CI, 0.81–2.12; P = .27) (Fig 3). However, on subgroup analysis based on the TICI score reperfusion definition, ASR had a significantly higher odds of achieving successful final reperfusion when defined as mTICI ≥2b compared with SR alone (OR = 1.64; 95% CI, 1.04–2.50; P = .03), whereas in studies that defined reperfusion as mTICI 2c/3, there was no difference between ASR and SR (OR = 0.72; 95% CI, 0.22–2.39; P = .59) (Fig 3).
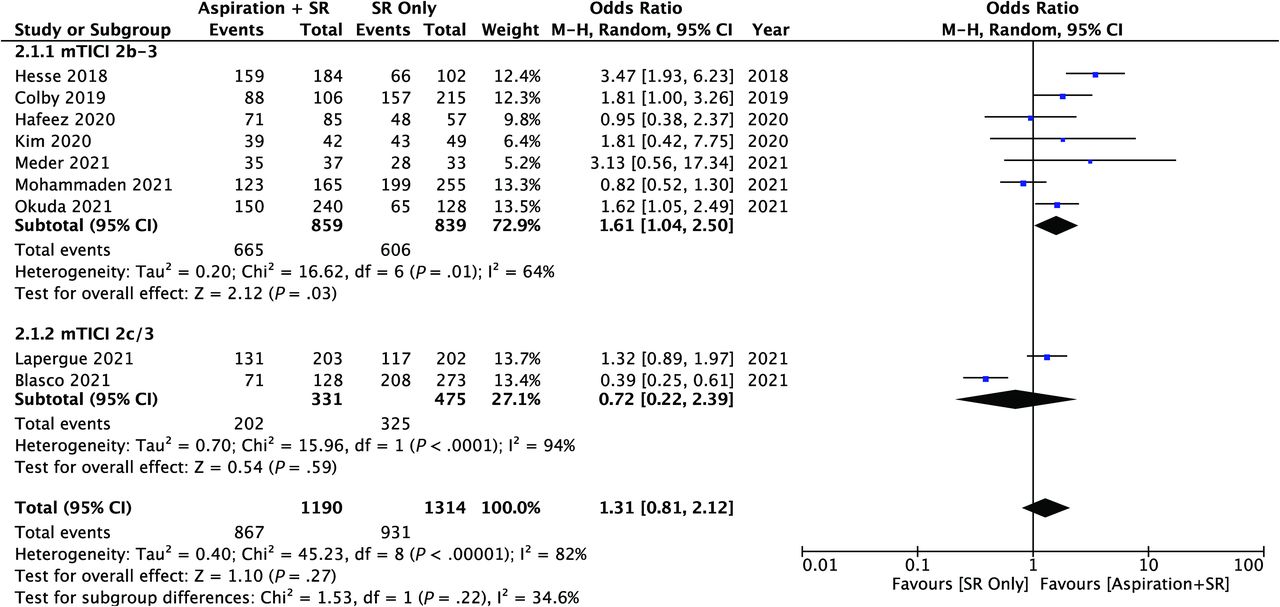
Forest plot for final reperfusion analysis. M-H indicates Mantel and Haenszel.
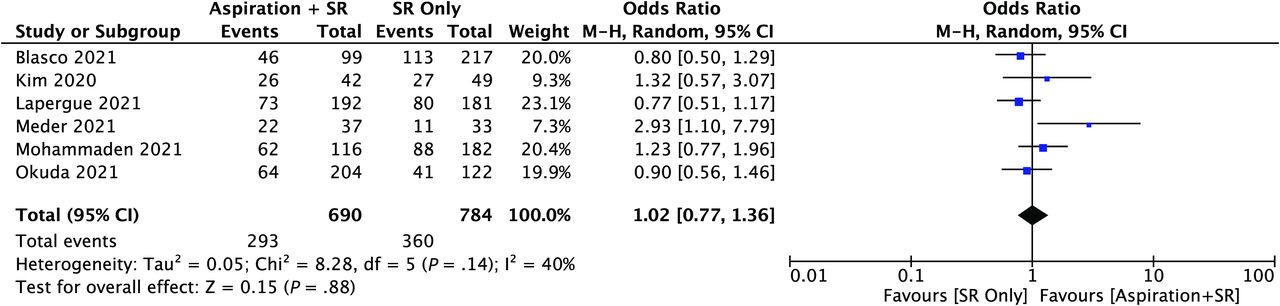
For the last main outcome measure of functional independence (ie, 90-day mRS of 0–2), there was no significant difference in reported composite rates between ASR (42.5%, 293/690) and SR (45.9%, 360/784) (P = .19), which was also the same on the meta-analysis (OR = 1.02; 95% CI, 0.77–1.36; P = .88; I2 = 40%) (Fig 4). The 90-day mortality rates from those studies that reported it were also investigated. Overall, the composite mortality rates between ASR and SR were not significant at 17.9% (117/651) verses 16.8% (132/787), respectively (P = .58).
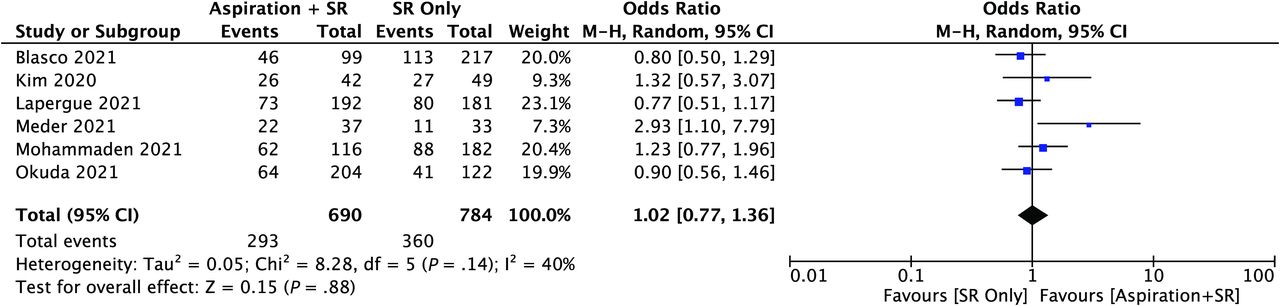
Forest plot for functional independence (90-day mRS of 0–2). M-H indicates Mantel and Haenszel.
Assessment of Heterogeneity and Bias
An assessment of interstudy heterogeneity among the included studies was completed and described using the I2 and heterogeneity P values. For the primary FPE analysis, there was moderate heterogeneity among the included studies (I2 = 72%, P = .0002). Regarding the successful recanalization analysis, there was considerable interstudy heterogeneity (I2 = 82%, P < .001). There was nonsignificant low heterogeneity among the studies included in the functional outcome analysis (I2 = 40%, P = .88). The Egger test was used to assess potential publication bias for the primary outcome measures. Significant publication bias was found in the functional independence analysis (P = .05). There was no significant publication bias in the FPE analysis (P = .75) or the reperfusion analysis (P = .68).
DISCUSSION
This was the first meta-analysis to evaluate the efficacy between ASR compared with SR alone for the treatment of AIS. The current literature comprises retrospective studies and a single randomized controlled trial. On pooled quantitative synthesis, ASR was associated with a superior first pass success rate (OR = 1.63, P = .002). However, there was no significant difference between ASR and SR regarding final reperfusion, functional independence, or 90-day mortality.
The headlines emerging from randomized trials suggest similar final reperfusion with varying technical approaches to endovascular thrombectomy. The ASTER randomized clinical trial compared primary contact aspiration with primary SR and found no difference in final successful revascularization rates.2 The recent ASTER2 randomized controlled trial similarly investigated the efficacy of ASR verses SR alone and also found no difference in final reperfusion rates of eTICI ≥2c (64.5% versus 57.9%, P = .17).9 However, the absolute difference of 6.6% in ASTER2 did exceed the minimal clinically important differences, believed to be between 3.1% and 5%.14 The authors acknowledged that a treatment effect of 15% was expected, so ASTER2 may have simply been underpowered.
Although the primary end point did not, several relevant secondary end points in ASTER2 favored ASR over SR alone. ASR was superior at achieving eTICI 2b/2c/3 (86.2% versus 72.3%, P < .001) and eTICI 2c/3 (59.6% versus 49.5%, P = .04) after the assigned initial intervention alone, which could be repeated up to 3 times.9 There was a trend toward improved FPE with ASR (40.9% versus 33.7% eTICI 2c/3, P = .12; 53.7% versus 44.6% eTICI 2b50/2c/3, P = .06), though this did not reach statistical significance. An additional study of 1832 patients found that combined thrombectomy and thromboaspiration resulted in a superior FPE compared with SR alone, and in those patients in whom FPE was achieved, a significantly better outcome and 90-day mortality result was observed.4 In the present meta-analysis, no difference in final reperfusion was observed (P = .27), but achievement of TICI 2b/2c/3 after first pass was superior in the ASR group (OR = 1.63, Fig 2). However, while there was no significant difference in final reperfusion overall, subgroup analysis based on the reperfusion definition revealed that ASR was superior at achieving mTICI 2b/3 (OR = 1.61, P = .03). Given that there was no significant difference in mTICI 2c/3 (Fig 3), this finding seems to suggest that the mTICI 2b/3 subgroup result was likely due to a higher proportion of mTICI 2b final reperfusion.
There has been a movement toward making FPE the primary outcome of trials of endovascular thrombectomy. This has largely been on the basis of reduced complications associated with fewer passes15 and superior outcomes if complete reperfusion is achieved after the first pass.16 FPE also has statistical advantages: Outcomes that are evenly distributed between good and bad are more sensitive in demonstrating the salutary and detrimental effects of procedural variation. A previous meta-analysis showed that FPE and modified FPE rates after endovascular thrombectomy generally were 28% and 45%, respectively.17 Final reperfusion in most LVO series was ≥80%, which may limit the ability to detect differences resulting from technical variation.18 Moreover, final reperfusion is necessarily reported as intention-to-treat, given the technical crossover that occurs in second, third, and subsequent passes. FPE, by contrast, more closely represents the results of a single embolectomy technique. ASTER2 required 3 attempts with identical techniques,9 though in retrospective series crossover occurs in as high as 30%–45% of cases.5,7
Given that ASR is associated with superior FPE and that FPE is associated with better outcomes, it was surprising that ASR was not also associated with superior clinical results on the meta-analysis. A possible explanation is that many studies, including ASTER2, required the use of a balloon-guide catheter (BGC) in both treatment arms.5,9 BGCs arrest flow, reducing clot fragmentation and distal emboli.19 Mechanistic overlap was observed from the introduction of intermediate aspiration catheters: Kurre et al20 reported a reduction (14.6% to 3.3%) of distal emboli by adding an intermediate aspiration catheter to the SR without the use of a BGC. Bourcier et al21 showed that a BGC does not confer better reperfusion and clinical outcomes compared with no BGC when used with combined SR and contact aspiration. Given the overlapping mechanism of a BGC and distal aspiration, it is plausible that the requirement of BGCs in studies comparing ASR and SR functionally diluted the effect of the intermediate aspiration catheter. This possibility could explain why the ASTER2 trial did not achieve a significant difference in final reperfusion, and why it may have been underpowered. Additionally, the outcome measure we investigated was 90-day mRS, but it is possible that the outcome differences between ASR and SR are more granular—that is, they may be limited to short-term issues and complications that resolve by day 90: temporary physical deficits, prolonged hospital stay, increased discharge to rehabilitation facilities, and/or higher procedural costs because rescue techniques may be required. These possibilities are an avenue for future studies and should be considered in future trial design.
This study has several limitations. First, there is a degree of heterogeneity in regard to the embolectomy technique, including the required use of a BGC, which may function as a confounding variable. Most studies in the analysis required or primarily used a BGC with their technique,5⇓⇓⇓-9,11 whereas in some studies, it was more variable or did not necessitate a BGC for inclusion in the analysis.4,10,13 Additionally, there has been only 1 randomized controlled trial to date; thus, the data in the literature are limited to single or multicenter retrospective/prospective analyses, which are prone to biases inherent to their study design. Furthermore, the definition of FPE and final reperfusion varied among studies: Some defined them as achievement of mTICI 2c/3, and others, as reaching eTICI ≥2b. Although we included only comparative studies with internal controls and completed subgroup analysis based on outcome definition to compensate for this difference, the results should still be interpreted within this context.
An additional limitation is that this study compared only 2 techniques without association with any other variables that could alter their efficacy. For example, clot composition was not considered but has been shown to influence FPE in thrombectomy.22 Similarly, this study did not account for the presence of a positive susceptibility vessel sign, which has also been shown to predict and influence the success of thrombectomy.23 In fact, the ongoing Vesair Balloon Confirmatory Trial (VECTOR) is investigating how positive susceptibility vessel sign occlusions might influence the efficacy of a first-line SR combined with contact aspiration versus contact aspiration alone.24 Moreover, thrombus positioning was also not considered even though thromboaspiration success has been shown to be influenced by the interface angle between the clot and thrombectomy device.25 Last, we also observed a moderate-to-considerable degree of interstudy heterogeneity within the FPE and recanalization analyses, likely, in part, due to the aforementioned limitations. Thus, the results described here should be interpreted with these considerations.
CONCLUSIONS
The current literature indicates that ASR results in a superior FPE compared with SR alone. Despite no significant difference in final recanalization overall, subgroup analysis suggests that ASR may result in superior final reperfusion when defined as mTICI ≥2b. Nonetheless, there was no significant difference in functional outcomes between the 2 techniques. Further research should focus on variables that account for differences between ASR and SR, such as the use of a BGC, among others.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received November 9, 2021.
- Accepted after revision January 11, 2022.
- © 2022 by American Journal of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clot composition and recanalization outcomes in mechanical thrombectomy
- Impact of aspiration catheter size on clinical outcomes in aspiration thrombectomy
- Mechanical thrombectomy with combined stent retriever and contact aspiration versus stent retriever alone for acute large vessel occlusion: data from ANGEL-ACT registry