Article Text

Abstract
Objectives Intracranial arteriosclerotic disease is a relevant cause of ischemic stroke worldwide with a high recurrence rate despite best medical treatment. Following the SAMMPRIS trial, endovascular treatment has remained a second-line therapy. Meanwhile, there has been significant advances in device technology. SeQuent Please NEO is a novel polymer-free, drug-coated (paclitaxel/iopromide) balloon (DCB) primarily designed for cardiology. Because of its high flexibility and pushability, it may also be suitable for intracranial use. The aim of this study was to assess the feasibility and safety of SeQuent Please NEO DCB in symptomatic intracranial severe stenosis.
Methods A single-center retrospective cohort study of patients with symptomatic intracranial severe stenosis treated with SeQuent Please NEO DCB was performed at a tertiary stroke center.
Results Ten patients (all men, median age 73 years (IQR 69–77)) were included. Median pre-treatment stenosis grade was 78% (IQR 75–80%) with four internal carotid artery, two mid-basilar artery, and four vertebral artery lesions. Median post-treatment stenosis grade was 50% (IQR 45–53%). Successful angioplasty was achieved in all cases without technical failure. There were no cases of peri-procedural reocclusion and no deaths at median follow-up of 3 months (IQR 2–3).
Conclusion In this pilot study, SeQuent Please NEO DCB was feasible and safe in the treatment of symptomatic intracranial severe stenosis. It might represent a promising alternative to medical treatment in selected cases.
- angioplasty
- atherosclerosis
- balloon
- stroke
Statistics from Altmetric.com
Introduction
Intracranial atherosclerotic disease (ICAD) is responsible for 10% of all acute ischemic strokes worldwide. This differs among ethnicities, with the lowest prevalence in Caucasian people (9%) and the highest in Asian populations (33–37%).1–3 Since the SAMMPRIS trial,4 best medical therapy represents first-line treatment for symptomatic ICAD. However, the SAMMPRIS study design may not have resulted in a representative conclusion and there is growing evidence that not all patients with ICAD benefit from best medical treatment alone. In particular, patients with unstable plaque and hemodynamic ischemic events are at a higher risk for recurrent events (up to 35%) despite medical treatment.5 6 In these cases an interventional approach might be suitable.7 To date, different interventional techniques with mostly good technical success and varying outcome rates have been described, ranging from angioplasty alone to complex stent-angioplasty systems.4 8 9 The phenomenon of restenosis caused by neointimal hyperplasia that frequently lowers the mid- and long-term results of ICAD treatment is well recognized. Angioplasty with a drug-coated balloon (DCB) is already well established and frequently used in cardiology, with DCB-PTA recently demonstrating non-inferiority to the current standard DES-PTA.10 Antiproliferative agents, such as the highly lipophilic microtubular stabilizer paclitaxel, prevent neointimal hyperplasia by inhibiting migration and cell division (figure 1). 11 A recent retrospective study of 19 patients with symptomatic ICAD showed promising results for a paclitaxel-coated DCB compared with the Wingspan stent system, with a lower recurrence rate.12

Artistic drawing depicting the concept of the drug-coated balloon (DCB) technique. (A) Pre-interventional symptomatic intracranial severe stenosis. (B) In the monorail technique, a DCB is navigated over the lesion and deposited exactly. The balloon is sub-maximally inflated. (C) During dilatation for 30 s the drug-coated surface (paclitaxel) comes into close contact with the vessel wall with homogenous distribution of the drug. (D) Post-interventionally, there is a reduction of the stenosis coated with drug that will avoid restenosis by an antiproliferative effect on the intimal cells.
SeQuent Please NEO (B Braun, Melsungen, Germany) belongs to the latest generation of coronary DCBs, with a specific matrix coating (iopromide/paclitaxel) for homogenous and effective drug delivery as well as improved flexibility and pushability.13 These are all features which make this DCB suitable for intracranial use.
The aim of this study was to evaluate the feasibility and safety of the SeQuent Please NEO DCB in patients with symptomatic ICAD with severe stenosis.
Methods
Patient selection
This retrospective single-center, open-label, single-arm cohort study was performed at a tertiary stroke center between September 2016 and January 2018. The study was approved by the local ethics committee. Patients had to be aged >18 years with clinically symptomatic ICAD of a severe stenosis (70–99%) confirmed by at least one diagnostic imaging modality (MRI, CT, digital subtraction angiography (DSA)). Prior to the intervention, an interdisciplinary team of neurologists and neurointerventionalists evaluated each case for the indication.
Procedure
All procedures (n=10) were performed under general anesthesia. All patients received dual antiplatelet therapy (DAT) with aspirin and clopidogrel in standard dosage prior to the intervention. In one case ticagrelor was used instead of clopidogrel due to cardiological indication. In all cases, an additional heparin bolus (median 5000 IE, IQR 5000–5000) adjusted for body weight, according to activated clotting time blood test, was administered prior to the intervention. For prevention of vasospasm, nimodipine (2 mg/L) was administered. All procedures were performed on a biplane angiography system (Allura Xper, Phillips, the Netherlands).
In brief, a right femoral access with a 7F sheath was used. A four-vessel angiogram was performed and the degree of stenosis was assessed according to WASID Study Group criteria14. Usually a 6F guiding catheter (0.053 inch Neuron; Penumbra, Alameda, California, USA or 0.07 inch Envoy; Codman, Raynham, Massachusetts, USA) was used for device delivery. Under roadmap guidance, a 0.014 inch micro guidewire (Synchro2 wire; Stryker Neurovascular, Fremont, California, USA) crossed the stenosis. The tip of the wire was placed distal to the lesion. A properly sized balloon was centered across the stenosis using the over-the-wire technique and slowly inflated to sub-nominal pressure (median 6 bar, IQR 4–8), with pressure above the nominal pressure only in case of rigid stenosis. Balloon size was selected according to the minimum diameter of the target vessel with respect to the submaximal angioplasty technique. The length should at least cover the plaque. DCBs were kept inflated on average for 30 s to facilitate drug delivery. After deflation and withdrawal of the DCB, a post-interventional angiogram was done to exclude perforation, vessel dissection, or distal embolization as well as to confirm the result. In all cases, Sequent Please NEO was used as the DCB. Belonging to the latest coronary DCB generation, Sequent Please NEO has a specific polymer-free matrix coating with paclitaxel and iopromide. The smaller balloon profile offers homogenous drug delivery as well as improved flexibility and pushability.13 We used DCB balloon diameter and length from 2.0 mm x 10 mm to 4.0 mm x 20 mm.
At the end of the intervention, all patients received an Xper-CT to immediately rule out any bleeding or ischemic complication. Additionally, within 24 hours after the procedure, all patients were monitored with intracranial ultrasound for immediate restenosis and hyperperfusion syndrome, as well as serving as a measurement starting point for follow-up control.
Post-interventionally, six patients (60%) were kept under DAT with aspirin and clopidogrel or ticagrelor for 3 months. In four cases (40%), DAT was reduced to single antiplatelet therapy within the first 3 months after intervention. In addition, all patients received lipid-lowering medication and cerebrovascular risk factors such as hypertension were controlled and medically treated.
Follow-up at a median of 3 months (IQR 2–3) was done with ultrasound and clinical examination performed by a stroke neurologist.
Imaging
The pre- and post-interventional degree of stenosis was assessed by WASID Study Group criteria using DSA.14 Follow-up degree of stenosis was determined by ultrasonography. Moreover, we added the Mori classification to characterize stenosis.15
Outcome measures
Clinical outcome measures were favorable outcome defined as modified Rankin Scale (mRS) score ≤2 at follow-up (median 3 months, IQR 2–3). Furthermore, peri-interventional and post-interventional recurrent ischemic events, defined as stroke in the respective vascular territory of the treated stenosis, were assessed. Technical and safety outcome measures were technical failure such as problem with balloon placement, as well as the post-interventional degree of stenosis and restenosis at follow-up. Restenosis at follow-up was assessed by ultrasound, comparing the ultrasonography findings with those obtained within 24 hours after the intervention.
Regarding safety issues, intracranial complications such as vessel perforation, dissection, intracranial hemorrhage as well as ischemic events were assessed.
Statistical analysis
All epidemiological, clinical, and imaging data were retrieved from the medical records and anonymized.
Descriptive statistics were performed using STATA 14.2 (StataCorp, Texas, USA).
Results
Patient population and lesion characteristics
All patients (n=10) were men with a median age of 73 years (IQR 69–77). The prevalence of the vascular risk factors hypertension and dyslipidemia were high (80%, n=8 each). Most patients presented with a transient ischemic attack (TIA) (80%, n=8) with a median NIH Stroke Scale (NIHSS) score on admission of 1 (IQR 0–1). Symptomatic stenoses were mostly located in the posterior cerebral circulation (60%, n=6), with four in the V4 segment of the vertebral artery and two in the mid-basilar segment. In addition, stenoses of the anterior circulation were located in the lacerum, cavernous, or ophthalmic segments of the internal carotid artery (40%, n=4). None of the treated lesions were located in the middle cerebral arteries. Commonly, additional stenoses with ≥50% degree (30%, n=3) or single occlusion (30%, n=3) or dual occlusion (10%, n=1) of the cerebrovascular circulation system were found. The median pre-procedure degree of stenosis was 78% (IQR 75–80%) with a median length of 9 mm (IQR 7–12 mm). The most common stenosis type according to the Mori classification was Type B (70%; n=7). Median time from symptom onset to treatment was 25 days (IQR 15–49 days)(table 1).
Population and stenosis characteristics
Clinical and technical outcome
All patients showed a favorable clinical outcome with a median mRS score of 1 (IQR 0–1) at follow-up. Median post-procedure residual stenosis degree was 50% (IQR 45–53%). At follow-up, no clinical ischemic incident was reported (table 2).
Clinical and technical outcome
Only one asymptomatic snow-plough effect occurred during balloon dilatation in a symptomatic ophthalmic segment ICA stenosis with occlusion of the origin of the ophthalmic artery, since there was an angiographically-proven external ophthalmic reconstitution.
No peri-procedural complications such as dissection, vasospasm, embolic ischemic events, or intracranial hemorrhage occurred. One patient developed a symptomatic arteriovenous fistula at the femoral puncture site which required surgical intervention. None of the patients died.
In terms of technical success, all treated stenoses remained stable during the sonographic 3-month follow-up. During one procedure the initially chosen DCB had to be changed to a smaller DCB, but no technical failure rate was observed.
Discussion
Our pilot study demonstrates that the use of a DCB is feasible and safe in selected patients with symptomatic ICAD of intracranial high-grade stenosis (70–99%) (figure 2).
{kind=link}
{kind=link}
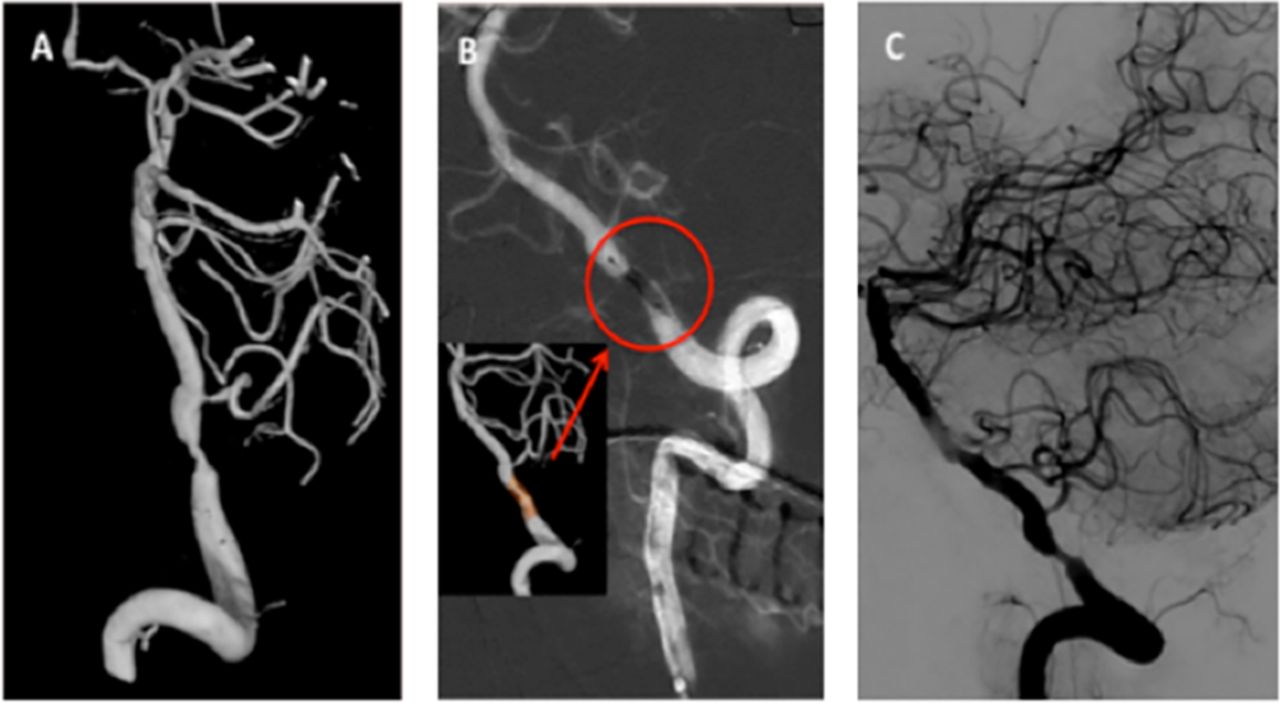
A patient with crescendo vertigo over a week due to a symptomatic vertebral artery stenosis on the right side. Medical history revealed previous transient ischemic attack in the vertebrobasilar system. (A) Pre-interventional 3D reformatted conventional angiogram showed a concentric high-grade V4-segment stenosis of the right-sided vertebral artery (75%). (B) SeQuent Please NEO (2.5 mm x10 mm) was successfully deployed over the lesion (red circle) and submaximally inflated (2x) with 10 bar. (C) Post-interventional control angiogram showed a residual stenosis (50%).
There is growing interest in interventional ICAD treatment. Undoubtedly, there is a need for a revascularization technique, and there is ongoing research about re-establishing intracranial stenting as a therapy option.16
Conversely, since the SAMMPRIS trial,4 there is still reluctance to use interventional procedures, particularly due to the high peri-procedure complication rates. Furthermore, mid- and long-term sequels with neointimal hyperplasia due to an inflammatory process after vascular damage from stenting and angioplasty occurred frequently,17 and were reported to be 5–30% in angioplasty alone.18 19 However, due to the high rate of recurrent stroke in patients with symptomatic intracranial high-grade stenosis despite best medical treatment, there is still a significant need for alternative treatment strategies. Accurate patient and interventionalist selection16 as well as innovative strategies such as the development of drug-eluting stents (DESs) or DCBs might serve to overcome previously reported challenges. DESs were used with a good technical success rate and low peri-procedural complications. Of note, they showed low symptomatic neointimal hyperplasia rates of around 5% compared with bare metal stents with rates of 14%.20–22 All DESs were designed for cardiological use and therefore they are relatively rigid and stiff, often not suitable for navigation in intracranial vessels. Thus, in one study a combined technique consisting of deployment of a DCB followed by a bare metal stent was described with promising results.23
Since its first intracranial use in 1980,24 primary angioplasty has shown promising results with low stroke and death rates of 5.8% within 30 days in a large single-arm cohort study of 116 patients with ICAD.8 Furthermore, primary angioplasty was comparable to stent placement with regard to peri-procedural stroke (7.4% and 7.1%, respectively), as reported in a large retrospective study of 190 patients.25 Thus, primary angioplasty might be an alternative to stenting, and combined with drug coating as a promising future option.7 12
A study of ICAD patients with in-stent restenosis used a former type of Sequent Please NEO and reported a low peri-procedural complication rate of 1.6% with a DCB failure rate of 8%.26 The relatively high deployment failure may be attributed to the fact that this DCB was not optimized for intracranial use.
A recent study showed that Neuro Elutax SV, a specifically dedicated DCB for intracranial use, had similar effectiveness and lower restenosis rates than Wingspan stents in patients with symptomatic high-grade stenosis.12 In addition, no complications with DCB-PTA occurred in that study.12 The results of the present study using the SeQuent Please NEO DCB system further support these observations.
To avoid dangerous peri-procedural complications such as dissections of the parent vessel, vessel perforation, and perforator occlusions, the submaximal angioplasty technique has been developed since its first description in the late 1990s.27 Recent data of a prospective phase I study demonstrated convincing results without stroke, hemorrhage, or death within 30 days after submaximal angioplasty.28 In our cohort we always used submaximal angioplasty, accepting somewhat higher median post-interventional degrees of stenosis compared with earlier studies with 2.5–23.9%,20 26 29 but paralleling the results with recent studies with a median post-procedural stenosis degree of up to 55%.12 28 This technique might offer the great advantage of non-traumatic vessel treatment with very low peri-procedural complications such as vessel perforation, snow-ploughing effect with consecutive perforator ischemia as well as distant embolic events. Since we have observed one snow-ploughing effect in our cohort, caution is needed regarding side branches adjacent to parental stenotic segments. Nevertheless, we support previous observations that patients with symptomatic ICAD will profit from submaximal angioplasty even with marginal restoration of blood flow.28
One limitation of this study is the rather small sample size. However, feasibility, functional outcome, and safety appear to be promising. A randomized controlled multicenter trial is required for further evaluation. Second, assessment of the degree of stenosis at the end of the procedure by DSA and at 3-month follow-up by neurovascular ultrasound only allows for a rough comparison. However, despite this methodological limitation, the degree of post-interventional stenosis largely remains stable.
Conclusion
Recent technical advances in the neurovascular field render endovascular recanalization a serious treatment option for selected patients with symptomatic ICAD. In particular, DCB-PTA with submaximal angioplasty using SeQuent Please NEO is feasible and safe. This might supplement the future armamentarium in the treatment of symptomatic ICAD. Long-term efficacy and benefits compared with best medical treatment need to be addressed in further studies.
References
Footnotes
Contributors PG: substantial contributions to the conception and design of the work; acquisition, analysis, and interpretation of data, and writing the manuscript. CB: acquisition of data and revising it critically for important intellectual content. JB, TK, JA: substantial contributions to the conception and design of the work and revising it critically for important intellectual content. MH, MD, KN: revising the work critically for important intellectual content. LR: conception and design of the work, revising it critically for important intellectual content, and final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval EKNZ.
Provenance and peer review Not commissioned; externally peer reviewed.