Article Text

Abstract
Background Age, neurologic deficits, core volume (CV), and clinical core or radiographic mismatch are considered in selection for endovascular therapy (ET) in anterior circulation emergent large vessel occlusion (aELVO). Semiquantitative CV estimation by Alberta Stroke Programme Early CT Score (CT ASPECTS) and quantitative CV estimation by CT perfusion (CTP) are both used in selection paradigms.
Objective To compare the prognostic value of CTP CV with CT ASPECTS in aELVO.
Methods Patients in an institutional endovascular registry who had aELVO, pre-ET National Institutes of Health Stroke Scale (NIHSS) score, non-contrast CT head and CTP imaging, and prospectively collected 3-month modified Rankin Scale (mRS) score were included. Age- and NIHSS-adjusted models, including either CT ASPECTS or CTP volumes (relative cerebral blood flow <30% of normal tissue, total hypoperfusion, and radiographic mismatch), were compared using receiver operator characteristic analyses.
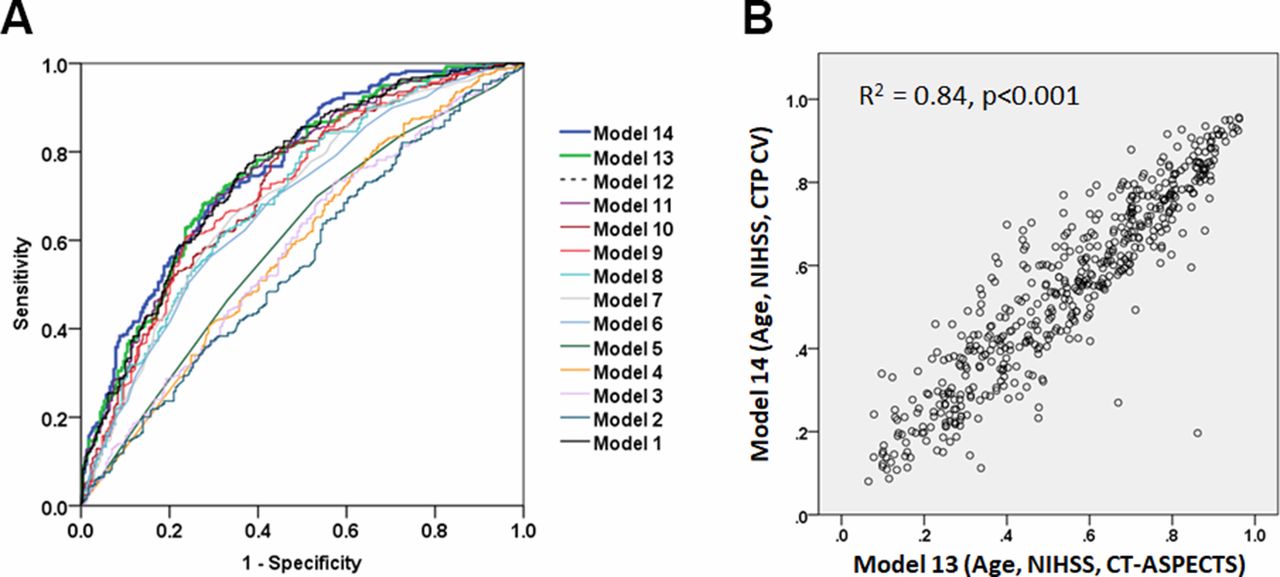
Results We included 508 patients with aELVO (60.8% M1 middle cerebral artery, 34% internal carotid artery, mean age 64.1±15.3 years, median baseline NIHSS score 16 (12–20), median baseline CT ASPECTS 8 (7–9), mean CV 16.7±24.8 mL). Age, pre-ET NIHSS, CT ASPECTS, CV, hypoperfusion, and perfusion imaging mismatch volumes were predictors of good outcome (mRS score 0–2). There were no differences in prognostic accuracies between reference (age, baseline NIHSS, CT ASPECTS; area under the curve (AUC)=0.76) and additional models incorporating combinations of age, NIHSS, and CTP metrics including CV, total hypoperfusion or mismatch volume (AUCs 0.72–0.75). Predicted outcomes from CT ASPECTS or CTP CV-based models had excellent agreement (R2=0.84, p<0.001).
Conclusions Incorporating CTP measures of core or penumbral volume, instead of CT ASPECTS, did not improve prognostication of 3-month outcomes, suggesting prognostic equivalence of CT ASPECTS and CTP CV.
- ct perfusion
- thrombectomy
- stroke
Statistics from Altmetric.com
Introduction
Endovascular therapy (ET) has been found to be better than medical therapy alone in patients with proximal anterior emergent large vessel occlusion (aELVO),1 presenting within the first 6 hours, and in selected patients seen up to 24 hours from time last seen well.2–5 Patient selection for ET involves a careful assessment of patient factors (age, baseline functional status), clinical stroke severity (typically measured by the National Institutes of Health Stroke Scale (NIHSS)), established core volume (by non-contrast CT Alberta Stroke Programme Early CT Score (ASPECTS) or CT perfusion (CTP)) as well as mismatch (clinical imaging or perfusion imaging mismatch).6–9 CT ASPECTS provides a semiquantitative estimation of established core volume (CV) using visible hypodensity as a surrogate for CV.10 11 CTP or magnetic resonance perfusion imaging, coupled with automated image processing (RAPID), enables a rapid quantitative assessment of established CV, total hypoperfused volume, and penumbral tissue at risk of core infarction. CTP CV and CT ASPECT scores are only modestly correlated12 and inter-rater reliability of CT ASPECTS has been found to vary from fair to substantial.13 14 While perfusion-based CV assessment overcomes these limitations of CT ASPECTS, obtaining additional perfusion imaging after non-contrast CT may also potentially contribute to treatment delays.15
Prognostic scores incorporating age, NIHSS, and CT ASPECTS as well as other critical variables such as pre-stroke functional status and collateral status, have been developed and validated for patient selection for ET7–9 but do not incorporate CTP metrics. Further improvement in the prognostic accuracy of preintervention models may be achieved by incorporating more objective and quantitative CTP data instead of CT ASPECTS.6–8 Therefore, we hypothesized that incorporation of CTP-based measures of CV and perfusion imaging might improve the prognostic performance of preintervention models that incorporate patient age, pretreatment NIHSS scores as compared with models containing CT ASPECTS.
Materials and methods
Study population
In this retrospective review of a prospectively collected interventional registry of patients with large vessel occlusion stroke from a tertiary care academic institution, data of consecutive patients from September 2010 through October 2017 with aELVO (middle cerebral artery (MCA) segments M1 and M2, internal carotid artery (ICA) terminus and extracranial ICA), baseline non-contrast CT, baseline NIHSS score, a technically adequate pretreatment CTP and/or pretreatment non-contrast CT head examination, and 90-day functional outcomes (modified Rankin Scale (mRS) score) were analyzed. Institutional review board approval was obtained for the maintenance of this registry. At this institution, selection for ET is based on multiple factors including clinical examination, imaging parameters, degree of clinical imaging mismatch or perfusion imaging mismatch, and a careful discussion between treating physicians and the patients/families.16
Clinical and imaging measures
Baseline non-contrast CT was used to determine CT ASPECTS by vascular neurologists. Imaging acquisition parameters were the same for all patients included in the study. CTP data from 8 cm of brain coverage were evaluated in a fully automated software environment using RAPID (version 4.5.0, iSchemaView, USA). Irreversibly damaged brain tissue—ischemic core (CV)—was defined by reduction in relative cerebral blood flow to <30% of that in normal tissue.17 Hypoperfused tissue was determined as a region of perfusion delay of >6 s (Tmax >6.0 s) and the mismatch volumes estimated henceforth.2 The primary cohort for this study included patients with CTP imaging performed before ET. To assess inter-rater reliability of CT ASPECTS ratings, we calculated the intraclass correlation between two independent raters of ASPECTS in a subset of 300 patients with ICA, M1 and M2 occlusions who had CTP imaging performed. In both instances, raters were board-certified neurologists. In a secondary analysis to validate findings in patients who underwent ET without CTP imaging, a second cohort of patients from the same institution treated during the same time was also included.
Statistical analyses
Continuous variables are reported as either mean±SD or median (IQR). Categorical variables are represented as proportions. Univariable logistic regression was performed to model good outcomes using known prognostic variables such as age, NIHSS score, CT ASPECTS, CV, and Penumbra (p<0.05 considered statistically significant). Multivariable regression models were developed to model good 3-month functional outcomes (see table 2) using age, NIHSS and either CT ASPECTS or CTP metrics. Models with only CT ASPECTS or CTP CV as well as those with only age, NIHSS, total hypoperfusion, and mismatch volumes were also tested. Receiver operating characteristic curve analyses were performed to determine prognostic accuracies (area under the curve (AUC)) in predicting 3-month good outcome (mRS score 0–2). Ordinal regression analysis was performed in which the mRS score was considered an ordinal dependent variable while age, NIHSS and CT ASPECTS or CTP CV were included as covariates. The pseudo-R2 (Nagelkerke) was used to determine overall predictive accuracy. SPSS version 23 was used for all statistical analyses. AUCs were compared using the Hanley and McNeil method.18
Results
Of 587 patients with aELVO and CTP before ET in our endovascular registry, 508 met the inclusion criteria (80 excluded owing to missing 3-month mRS score because they were lost to follow-up). This primary study cohort had a mean age of 64.1±15.3 years, median ASPECTS of 8 (IQR 7–9) and median baseline NIHSS score of 16 (IQR 12–20). A total of 60.8% had M1 MCA occlusions, 20.9% had M2 MCA occlusions, and 34% had ICA occlusions. Median time to ET from time last- seen-well was 350 (IQR 240–610) min and 218 (42.9 %) patients were treated beyond 6 hours from time last-seen-well. In 300 patients in the CTP cohort, we confirmed that the intraclass correlation between two independent raters across the entire range of CT ASPECTS was 0.55 (95% CI 0.46 to 0.62), suggesting a moderate level of inter-rater reliability.
The means of CV, hypoperfusion, and mismatch volumes were 16.7 (SD 24.8), 157.2 (SD 111.9), and 140.2 (SD 110.2) mL, respectively (table 1). Successful reperfusion (modified Thrombolysis in Cerebral Infarction (mTICI) 2b/3) was achieved in 94% of the patients (TICI2b: 38.6%, TICI2c/3: 55.7%) and the rate of good 3-month functional outcome (mRS 0–2) was 54.9% (table 1).
Baseline characteristics
Consistent with previous findings,7 univariable predictors of good outcome included age in years (OR=0.96, CI 0.942 to 0.967; p<0.0001), baseline NIHSS (OR=0.89, CI 0.858 to 0.920; p<0.0001), CT ASPECTS (OR=1.20, CI 1.082 to 1.323; p<0.0001), CV in mL (OR=0.989, CI 0.980 to 0.997; p=0.007), and hypoperfusion volume in mL (OR=0.998, CI 0.997 to 1.00; p=0.03), but not imaging-mismatch (OR=0.999, CI 0.997 to 1.00; p=0.12). We performed multivariable regression analyses by including age, NIHSS, and CT ASPECTS or CTP measures (hypoperfusion, CV, or imaging-mismatch) as predictor variables and 3-month mRS 0–2 as the outcome variable. CT ASPECTS and CTP CV were not included together in the same model owing to their biological collinearity. The 14 multivariable models tested are shown in table 2. As compared with the reference model that contained age, baseline NIHSS, and CT ASPECTS (model 10, AUC=0.76), the predictive accuracies of model 11 (age, baseline NIHSS, CTP CV, AUC=0.75, p=0.74), model 12 (age, baseline NIHSS, hypoperfusion volume, AUC=0.75, p=0.57), model 13 (age, baseline NIHSS, imaging mismatch, AUC=0.75, p=0.57), and model 8 (age, CV, AUC=0.72, p=0.12) were similar. Model 110had a slightly higher predictive accuracy than model 9 (age, hypoperfusion, AUC=0.70, p=0.04).
Prognostic accuracies of multivariable regression models for 3 month good functional outcome (modified Rankin Scale (mRS) 0–2)
Receiver operating characteristic curves comparing the prognostic accuracies of all models are shown in figure 1A. Predicted outcomes from models 1 and 2 also had excellent agreement (R2=0.84, p<0.001, figure 1B). Although time from last-seen-well to ET was not independently associated with good outcome (p=0.09 after adjusting for age, NIHSS, and CT ASPECTS), we stratified the CTP cohort into those treated within 6 hours (n=229) or beyond 6 hours (n=279) from time last-normal and assessed the prognostic accuracy of age/NIHSS/CT ASPECTS and age/NIHSS/CTP CV models to predict good outcome. Both models had comparable AUCs in the ≤6 hour (0.75 and 0.75) and >6 hour groups (0.77 and 0.76), confirming that time to treatment did not affect our overall results. In order to capture the entire breadth of the mRS scale rather than a dichotomized approach, we also performed ordinal logistic regression, in which mRS was used an ordinal outcome variable and compared age/NIHSS/CT ASPECTS and age/NIHSS/CTP CV models. In each ordinal regression model, all three covariates were independently associated with mRS score at 90 days (p<0.05 for each variable). The overall pseudo-R2 (Nagelkerke) was 0.24 for the first model and 0.22 for the second model, again suggesting similar overall predictive accuracy.
{kind=link}
Comparison of predictive accuracies of models containing CT Alberta Stroke Programme Early CT Score (ASPECTS) or CT perfusion (CTP)-based core volume (CV) measures. (A) Receiver operating characteristic curves (outcome 3-month modified Rankin Scale score 0–2) comparing predictive accuracies of 14 statistical models (see table 2 for details). Model 10 (age, baseline National Institutes of Health Stroke Scale (NIHSS) score, CT ASPECTS) and model 11 (age, baseline NIHSS score, CTP CV) are the key models of interest. (B) Correlation between predicted probabilities of good outcome based on CT ASPECTS and CTP CV-based models (models 10 and 11, respectively).
Since our study cohort was a purely endovascular cohort, it is also possible that homogeneity within the study population with uniformly favorable patient profiles might have contributed to the relatively small prognostic importance of CT ASPECTS or CTP CV on 3-month functional outcome. To deal with this, we performed sensitivity analyses by comparing model 1 (age, NIHSS, CT ASPECTS) and model 2 (age, NIHSS, CTP CV) in patients with more favorable (pre-ET CTP CV <50 mL) and less favorable pretreatment imaging profiles (pre-ET CTP CV ≥50 mL). In general, all models were more predictive in patients with CTP CV >50 mL (model 1: AUC=0.89, model 2: AUC=0.85), although models containing either CT ASPECTS or CTP CV performed equivalently in both subgroups.
Since CT and CTP imaging were carried out at almost the same time in this cohort, it is possible that CT ASPECTS interpretation by the treating provider might have been influenced by the CTP imaging data. If the observed similarity of models 1 and 2 was affected by this potential bias, we would expect the predictive accuracy of model 10 (age/NIHSS/CT ASPECTS) to differ significantly in a cohort where CT ASPECTS was used without CTP. Therefore, we additionally assessed the performance of model 10 to predict 3-month good outcomes in patients with aELVO, who were selected for ET based solely on CT ASPECTS without CTP imaging. As compared with the primary cohort used in our analysis, patients in the CT ASPECTS-only cohort (n=357, table 1) had higher baseline NIHSS score (median 19 (IQR 14–23), p<0.001), higher frequency of atrial fibrillation (41.9%, p=0.02) and cardioembolic etiology (p<0.001), higher ICA terminus occlusions (p=0.01), and overall lower rate of good outcome (mRS 0–2=39.2%, p<0.001). However, age (mean 66 years (SD 15) and CT ASPECTS (median 8 (7-9) were similar. Despite these differences, predictive accuracy of model 1 was similar to the primary cohort (AUC=0.74 vs 0.76, p=0.7).
Discussion
CT ASPECTS is an ordinal, semiquantitative scale used to estimate infarct core, although its correlation with CV is modest12 and inter-rater reliability is variable.13 14 However, CT ASPECTS compensates for these limitations by its simplicity and easy availability without dependence on technical expertise to perform CTP or need for image processing for interpretation. CT ASPECTS also remains a strong predictor of long-term outcomes in patients with aELVO, and a key parameter for patient selection for ET.7 10 We hypothesized that preintervention prognostic models that include age, pretreatment NIHSS, and CT ASPECTS might be improved if CT ASPECTS were replaced by CTP CV and measures of perfusion-imaging mismatch.8 However, contrary to this hypothesis, our results indicate that CTP CV does not alter the overall performance of the prognostic model. Consistent with our findings, a recent study also found no significant difference between predictive accuracies of CTP and CT ASPECTS in predicting hyperacute MRI lesion volumes in acute ischemic stroke.19 Therefore, our results suggest that additional incorporation of perfusion imaging data in preintervention prognostic models such as the THRIVE, PRE, or MR PREDICTS scores will not yield higher prognostic accuracy.6 9
Recent retrospective studies of patients with aELVO treated with ET have found that CTP selection paradigms may result in better 3-month clinical outcomes than purely CT ASPECTS-based approaches.16 20 However, results in this analysis suggest that overall prognostic accuracies of models containing either CT ASPECTS or CTP core are similar. This apparent discordance is explained by the fact that CT ASPECTS-based selection may include some patients for ET that CTP-based approaches would have excluded owing to the well-known inter-rater reliability and non-volumetric nature of CT ASPECTS,12 21 leading to better outcomes in the CTP-selected group. Consistent with this, we also found that rates of good outcome in the CTP-selected patients were significantly higher than in the CT ASPECTS-selected cohort within our registry. We also observed that models containing perfusion mismatch did not outperform models containing CTP core volume. This is in agreement with previous studies, in which perfusion mismatch-based patient selection resulted in exclusion of patients from ET without altering 3-month outcomes.16 This finding could be explained by the very high rates of successful reperfusion in our cohort, resulting in a close association between pre-ET core volume and final infarct volume. Another explanation is that clinical core mismatch is already partly accounted for in the model when NIHSS and CT ASPECTS (or CTP CV) are included, and thus, no additional prognostic value is added by including radiographic perfusion mismatch into the model. Lastly, it is also possible that RAPID-based CTP CV estimation (regional cerebral blood flow <30%) is a more accurate representation of true core infarct than RAPID-based estimation of true penumbral tissue. Although we have not explored these possibilities in our study, our findings emphasize the importance of applying the concept of ‘clinical-core mismatch’ as an easy and effective tool in patient selection for ET.
Regardless of the method used to estimate established core volume (CT ASPECTS or CTP), an area of active research in the field is whether ET can benefit patients with large core infarcts and whether established core volume before ET influences the treatment effect of ET. In the HERMES collaboration, no significant interaction between the treatment effect of ET and CT ASPECTS was observed (interaction p=0.052) although the total number of patients with ASPECTS <5 was relatively small. A CTP core volume by treatment effect interaction was also not seen in a post hoc analysis of MR CLEAN, in which only 175 out of 333 patients with CTP imaging were included in the analysis.22 However, estimates from the THRACE study suggest that the number needed to treat (NNT) to achieve an additional good outcome in patients with aELVO with large established core volumes (>80 mL) is >10 as compared with a NNT of 2–3 for those with small core infarct volumes.23 Based on these findings, future randomized studies will determine the magnitude of benefit of ET in patients with relatively large established core volumes.
Our study is limited by its retrospective nature, which might have introduced selection bias and biases due to lack of blinded measurement of CT ASPECTS or 3-month mRS score. Selection of patients for ET was also based primarily on CTP in conjunction with CT ASPECTS rather than either approach by itself. To partly overcome this, we validated our findings in a cohort of patients with aELVO treated by ET who were selected based only on CT ASPECTS without the need for CTP. Another limitation is that all patients included in the study underwent ET, therefore limiting its applicability when patients do not receive ET. Since CT ASPECTS and CTP were performed on all patients at nearly the same time and raters grading CT ASPECTS were not blinded to CTP findings, the CTP parameters might have influenced the grading of CT ASPECTS. Conversely, our study represents a real-world endovascular cohort as opposed to a highly controlled and selected randomized trial cohort. It is therefore important to validate our findings in more contemporary randomized ET trial datasets.
Conclusion
We observed that incorporation of CTP measures of core or penumbral volume did not improve prognostic accuracy of a model containing pre-ET variables, including age, NIHSS and CT ASPECTS, in patients with aELVO. These findings highlight the prognostic equivalency of CT ASPECTS and CTP CV in these patients. Before extending these findings to patient selection, future studies assessing the value of ASPECTS or CTP-based preinterventional risk-stratification tools in predicting the treatment effect of ET are warranted.
References
Footnotes
Contributors SAR and SR conceptualized the study, performed the analyses, and wrote the manuscript. CMB, GMR, DCH, MRF, and RGN assisted in data collection, adjudication of imaging and clinical data, and critically revising the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RGN serves as follows: Stryker: DAWN trial principal investigator, TREVO Registry steering committee, Trevo-2 trial principal investigator, consultant; Medtronic: SWIFT Trial steering committee, SWIFT Prime Trial steering committee, STAR Trial sngiographic core laboratory; Cerenovus/Neuravi: ENDOLOW trial principal investigator, ARISE-2 trial steering Committee, Physician Advisory Board; Phenox:Physician Advisory Board; Anaconda: Physician Advisory Board; Genetech: Physician Advisory Board; Biogen: Physician Advisory Board; Viz-AI: Physician Advisory Board; Vesalio: Physician Advisory Board; Ceretrieve: Physician Advisory Board; and Intervention Neurology Journal: Editor-In-Chief.
Patient consent Not required.
Ethics approval Institutional review board approval was obtained for this study.
Provenance and peer review Not commissioned; externally peer reviewed.