Article Text

Abstract
Objective To identify clinical, morphological, and hemodynamic independent characteristic factors that discriminate posterior communicating artery (PCoA) aneurysm rupture status.
Methods 173 patients with single PCoA aneurysms (108 ruptured, 65 unruptured) between January 2012 and June 2014 were retrospectively collected. Patient-specific models based on their three-dimensional digital subtraction angiography images were constructed and analyzed by a computational fluid dynamic method. All variables were analyzed by univariate analysis and multivariate logistic regression analysis.
Results Two clinical factors (younger age and atherosclerosis), three morphological factors (higher aspect ratio, bifurcation type, and irregular shape), and six hemodynamic factors (lower mean and minimum wall shear stress, higher oscillatory shear index, a greater portion of area under low wall shear stress, unstable and complex flow pattern) were significantly associated with PCoA aneurysm rupture. Independent factors characterizing the rupture status were identified as age (OR 0.956, p=0.015), irregular shape (OR 6.709, p<0.001), and minimum wall shear stress (OR 0.001, p=0.038).
Conclusions We combined clinical, morphological, and hemodynamic characteristics analysis and found the three strongest independent factors for PCoA aneurysm rupture were younger age, irregular shape, and low minimum wall shear stress. This may be useful for guiding risk assessments and subsequent treatment decisions for PCoA aneurysms.
- Aneurysm
- Blood Flow
- Hemorrhage
- Stroke
- Angiography
Statistics from Altmetric.com
Introduction
Unruptured intracranial aneurysms (UIAs) are increasingly detected and often remain clinically asymptomatic for a long time before rupture. However, the natural history of UIAs is not entirely clear, and there is still no clinical consensus on whether to choose continual observation or active surgical intervention.1 ,2 The reported mean observed 1-year risk of aneurysm rupture is 1.4% and the 5-year risk is 3.4%.1 Meanwhile, preventive treatment also indicates a risk for patients with UIAs: reported combined morbidity and mortality rates for surgical clipping are commonly >10%2 while, for endovascular management, the adverse outcome rate is up to 5%3 accompanied by a recurrence rate of 10–20%.4 Aneurysm rupture risk assessment can help doctor's decision-making, but data on UIAs that are prone to rupture are still infrequent and rare. Researchers therefore usually compare ruptured and unruptured aneurysms to explore potential markers for rupture risk, as it is assumed that UIAs with similar features to ruptured aneurysms may be at a higher risk.5
In recent years clinicians have begun to study aneurysm rupture in a systematic and location-specific manner. Posterior communicating artery (PCoA) aneurysms are one of the most common aneurysms (15–25% of cerebral aneurysms).6 ,7 Investigating rupture-related factors specific to PCoA aneurysms is particularly meaningful because this location indicates a relatively higher risk of rupture.7 ,8 One group in Japan retrospectively reviewed 134 consecutive patients with PCoA aneurysms (39 ruptured, 95 unruptured) and investigated their rupture-related clinical and morphological characteristics,9 and another group in America evaluated 63 patients (40 ruptured, 23 unruptured).10 Both groups reported interesting findings, but they also provided some conflicting results on, for example, age, hypertension, and aneurysm size.
Hemodynamic factors are thought to be important for aneurysm rupture, and computational fluid dynamics (CFD) has become a popular non-invasive tool for studying intracranial aneurysm hemodynamics.5 ,11 Researchers performed morphological–hemodynamic analysis on matched pairs of ruptured/unruptured mirror or symptomatic PCoA aneurysms and found correlations between some hemodynamic factors and PCoA aneurysm rupture.12 ,13 This is encouraging and promising, but the findings are limited by very small sample sizes and lack of analysis of clinical characteristics.
Here we report a larger sample size of 173 location-specific (ie, PCoA only) aneurysms in a single center. Another innovation is that we comprehensively examined three types of reported features (clinical, morphological, and hemodynamic) associated with aneurysm rupture. Multivariate logistic regression analysis will help to avoid potential confounding factors and inherent correlations often seen in single observational studies.
Materials and methods
Patients
A total of 173 patients were retrospectively selected from our database according to the following criteria: (1) patients with PCoA aneurysms admitted to our hospital between January 2012 and June 2014; (2) single aneurysms; and (3) rupture status identified by intraoperative findings or head CT scan imaging. The exclusion criteria were: (1) fusiform or dissecting aneurysms; and (2) multiple aneurysms (the presence of which may be an independent risk factor for aneurysm rupture14 and sometimes it is hard to define the bleed site).
All the medical data were acquired for diagnostic purposes and the research was approved by the ethics committee of the institute.
The patients were divided into two groups: ruptured (108 cases) and unruptured (65 cases). Their clinical characteristics including age, sex, health habits (cigarette smoking and alcohol drinking), and comorbidities including hypertension, diabetes mellitus, hyperlipidemia, atherosclerosis, cerebral infarction, and coronary heart disease were compared.
Modeling of aneurysms
Patient-specific three-dimensional (3D) digital subtraction angiography (DSA) data were obtained and a software package developed in-house was used to create and modify a stereolithographic image that contained blood vessel luminal surface information.15 A number of geometric features including aneurysm size (maximum height), neck width, surface area, volume, aspect ratio (dome to neck ratio), and size ratio (dome to parent vessel diameter ratio) were measured and calculated.
The number of each morphological type including neck size (≥4 mm, wide; <4 mm, narrow), aneurysm size (>7 mm/≤7 mm), lateral/bifurcation type (at the vessel junction with branch diameter/parent vessel diameter >1/5, bifurcation type; otherwise, lateral type16), small vessel on aneurysms (with branch taking off from the aneurysm and size <1/5 parent vessel diameter), and irregular shape (blebs, nipples, or multiple lobes) were recorded.
Numerical simulation
The inlet for each 3D image is on the internal carotid artery cervical segment. A mesh independence analysis was performed and the maximum element size was set to 0.2 mm. Each model was imported into ANSYS Workbench V14.0 (ANSYS, Canonsburg, Pennsylvania, USA) to create more than 1 000 000 finite volume tetrahedral element grids. The governing equations underlying the calculation were the Navier–Stokes formulation with an assumption of Newtonian fluid, laminar and incompressible blood flow. The density and dynamic viscosity of blood were specified as ρ=1060 kg/m3 and μ=0.004 Pa·s, respectively. The inflow boundary condition was a pulsatile period velocity profile of an ordinary person. Two cardiac cycle simulations were performed and the second cycle was taken as output.
After CFD simulation, the following hemodynamic variables were calculated: (1) wall shear stress (WSS)-related variables: the time-averaged WSS was calculated by integrating the WSS magnitude over the cardiac cycle, the WSS was then normalized by the average vessel WSS at the anterior genu of the carotid siphon in the same patient to minimize the dependence on the inlet condition,17 and the mean, maximum, and minimum time-averaged WSS (defined as WSSmean, WSSmax and WSSmin, respectively) on the aneurysm sac were recorded; (2) oscillatory shear index (OSI) calculated using the method described by He et al18 and defined as the spatially averaged OSI on the aneurysm; (3) low WSS area (LSA): proportion of the low WSS area (<10% of the mean vessel WSS at the anterior genu of the carotid siphon) to the whole area of the aneurysm;17 (4) flow pattern: flow complexity (simple/complex) and flow stability (stable /unstable) were defined using the method of Byrne et al.19
Statistical analysis
Statistical analysis was performed with a SPSS V17.0 package. Univariate analyses were performed to obtain valuable variables: the χ2 test was performed to compare frequencies and the Fisher's exact test and Bonferroni correction (for R×C table) were used to compare the differences between age groups. For quantitative data, the one-sample Kolmogorov–Smirnov test was used to test the normal distribution and the unpaired t test/rank sum test was then applied. For all marginal or significant univariate variables, collinearities were tested and controlled. Multivariate backward stepwise logistic regression was then performed to obtain independent characteristic factors for rupture; p<0.05 was considered statistically significant.
Results
Clinical factors
Patients with ruptured aneurysms were graded according to the Hunt and Hess scale (grade I–II: 75.9% (82/108); grade III–V: 24.1% (26/108)). In the group with unruptured aneurysms, 61.5% (40/65) had no symptoms or only headache or dizziness, 15.4% (10/65) had a transient ischemic attack or ischemic stroke, 12.3% (8/65) had occulomotor nerve palsy, and 10.8% (7/65) had blurred or decreased vision.
Table 1 shows the results of the comparison of clinical characteristics. Patients in the ruptured group tended to be slightly younger and to have atherosclerosis. The proportion of patients with ruptured aneurysms was higher in the 40–49 and 50–59 age groups than in the 60–69 age group. No significant differences (p>0.10) were found for other clinical characteristics.
Clinical characteristics
Morphological factors
Compared with unruptured aneurysms, ruptured aneurysms had a significantly higher aspect ratio and tended to be of bifurcation type with an irregular shape. Except for the size ratio, which had a marginally significant difference (p=0.088), other morphological factors showed no significant differences (p>0.10, table 2).
Morphological characteristics
Hemodynamic factors
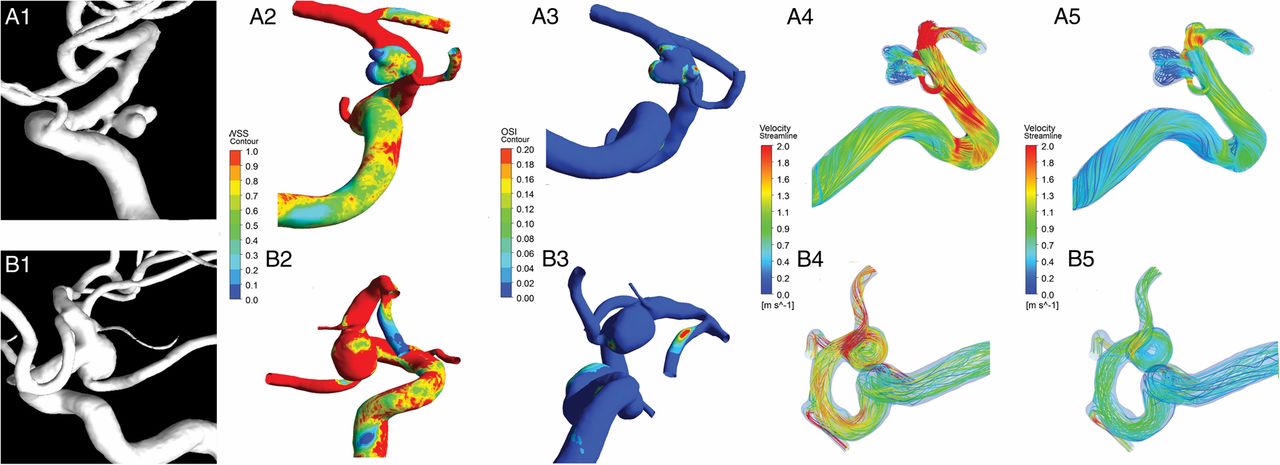
Figure 1 shows comparisons of hemodynamics characteristics. Compared with the unruptured group, the ruptured group had significantly lower WSSmean and WSSmin but higher OSI and LSA. Unstable and complex flow patterns were more often found in the ruptured group. Other hemodynamic factors showed no significant differences (p>0.10, table 3).
Hemodynamic characteristics

{kind=link}
Morphological and hemodynamic characteristics of two representative posterior communicating artery aneurysms: (A) ruptured; (B) unruptured. From left to right: (1) three-dimensional digital subtraction angiography images; (2) normalized time-averaged wall shear stress (WSS); (3) oscillatory shear index (OSI); (4) streamlines at the systolic peak; (5) streamlines at the diastolic end. The ruptured aneurysm has irregular shape, higher aspect ratio (dome to neck ratio), lower WSS, higher OSI, complex and unstable flow pattern.
Collinearity
The multicollinearity diagnostic results for all marginal or significant univariate variables are shown in online supplementary table S1. Age and age group are highly correlated. We only kept age for further logistic regression analysis because it contains more statistical information. For aspect ratio and WSSmean (which are moderately related), stepwise regression can help control for collinearity bias and we obtained the same logistic regression results when one or both were initially entered.
Multivariate logistic regression analysis
One clinical factor (age), one morphological factor (irregular shape), and one hemodynamic factor (WSSmin) were found to be independent predictive factors for the rupture status of PCoA aneurysms.
The ORs indicate that ruptured aneurysms are 6.709 times (95% CI 2.991 to 15.048, p<0.001) more likely to be irregularly shaped. Age (OR 0.956, 95% CI 0.922 to 0.991, p=0.015) and WSSmin (OR=0.001, 95% CI 0.000 to 0.689, p=0.038) are inversely correlated with aneurysm rupture.
Discussion
This study identified rupture-related factors in a large cohort of patients with PCoA aneurysms. We focused our attention on the interplay of clinical, morphological, and hemodynamic factors associated with aneurysm rupture. The novel findings are that, when a number of putative factors were considered, age, irregular shape, and WSSmin were the only independent factors able to distinguish ruptured aneurysms. Aneurysm size was not related to aneurysm rupture.
Clinical factors
Patient age appeared to be independently and inversely correlated with PCoA aneurysm rupture in this study. Some retrospective results specific to PCoA support our finding. A meta-analysis performed by He et al20 found that age was negatively correlated with the rupture status of true PCoA aneurysms. Matsukawa et al9 found that patients with ruptured PCoA aneurysms were younger, and age <60 years was an independent age-related rupture discriminator.9 Our further analysis in different age groups found that the proportion of patients with ruptured aneurysms in the 40–49 age group and 50–59 age group was higher than in the 60–69 age group. This might be explained by the fact that PCoA aneurysms rupture earlier than other aneurysms or because older people die of other causes. Further research and discussion is needed before definitive conclusions can be drawn.
With regard to other clinical factors, our later logistic analysis excluded atherosclerosis as an independent characteristic factor for rupture. Female sex, smoking, drinking, and hypertension were not significantly correlated with PCoA aneurysm rupture. This may be because these common factors may be influenced by more confounding factors. Further study with a larger sample and inclusion of a normal control group may help to resolve this question.
Morphological factors
Studies on UIAs have proposed that aneurysm size is a key predictor for rupture, with diameter >7 mm representing a much higher risk of subarachnoid hemorrhage.7 ,8 ,21 However, the PCoA is considered to be a special location with a higher risk even with a diameter of ≤7 mm.7 In our study, 74.6% of the PCoA aneurysms were ≤7 mm. The median size was 5.33 mm for ruptured aneurysms and 4.36 mm for unruptured aneurysms, but the difference did not reach statistical significance (p=0.145). Matsukawa et al9 found that ruptured PCoA aneurysms were more often >7 mm in diameter, but they excluded this factor in later logistic analysis. Ho et al10 studied 63 PCoA aneurysms and found a similar size between the ruptured and unruptured group (5.97 mm vs 5.85 mm, p=0.440). All these data indicate that size may not be a good assessment factor for rupture of PCoA aneurysms. This also highlights the importance of location-specific study of intracranial aneurysms.
Irregular shape has been reported to be an independent predictor of aneurysm rupture.7 ,22–25 Focal bulges on the surface of an aneurysm often indicate a weak and thinner wall, indicating a higher risk of rupture.22 ,24 Our study has extended previous investigations in this area by showing that this notion is also applicable in PCoA aneurysms.
Hemodynamic factors
Localized extraordinarily low WSS caused by flow stagnation or intra-aneurysmal thrombosis is thought to have local inflammatory effects on the arterial wall, to which chronic exposure might cause ongoing wall degeneration and thinning and finally rupture.26 ,27 Previous retrospective studies have reported a close connection between WSSmin and aneurysm rupture. Fukazawa et al27 investigated the association between local hemodynamic features and rupture points observed during the microsurgical clipping in 20 ruptured aneurysms. The bleeding point was correlated with a markedly low WSSmin but not with aneurysm size or aspect ratio.27 To investigate possible features linked to bleeding aneurysms independent of patient characteristics, Zhang et al28 studied 20 aneurysm pairs with different rupture status in the ipsilateral anterior circulation of one patient. The ruptured aneurysms were found to have lower WSSmin than the unruptured aneuryms in the pairs.28 Our study has come to a similar conclusion in a location-specific (PCoA) manner. In addition, the results of a prospective study have provided further verification only on PCoA. Takao et al29 studied initially unruptured aneurysms of medium size (50 cases each on the PCoA and middle cerebral artery (MCA)). Rupture occurred in six PCoA aneurysms and seven MCA aneurysms during follow-up. A comparison of the initial hemodynamic data of the ruptured aneurysms and those that did not rupture showed that lower WSSmin on PCoA aneurysms was the only significant WSS parameter to predict future rupture.29
Limitations of this study
Some limitation of the present study must be noted. First, this is a study based on single-center data with inevitable selection bias. Second, this is a retrospective study and our research only documented the features of PCoA aneurysms before or after rupture. Sometimes it was technically difficult to separate small vessels on aneurysms from artifacts of closely neighboring vessels. Also, there is no general agreement on rupture-associated changes in aneurysm shape.25 ,30 Of the 65 patients with UIAs included in this study, only 21 chose to have continuous observations and, to date, angiographic follow-up data for only five cases are available (1–20 months post-discharge, mean 7.5 months) but no rupture or morphological changes have been found. Continued follow-up of the participants with unoperated UIAs in this study will be helpful to verify our results. Finally, patient-specific inlet flow rates are unknown. The same inlet setting may make hemodynamic results depend on the geometry of the luminal models. We did normalization on aneurysm WSS by vessel WSS to help remove dependence on the inlet flow condition, performed multicollinearity diagnostics to identify high correlations among the variables and did corrections accordingly. Moderate multiple collinearity between one morphological factor (aspect ratio) and one hemodynamic factor (WSSmean) was identified but this did not affect our final results.
Conclusion
This study analyzed a combination of clinical, morphological, and hemodynamic characteristics in a systematic and location-specific study of rupture of PCoA aneurysms. Three factors (age, irregular shape, and WSSmin)—that is, one factor per category—were found to be independently associated with PCoA aneurysm rupture. Our findings addressed the importance of studying aneurysms in a location-specific manner and help to improve rupture risk assessment for patients with PCoA aneurysms.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors YZ drafted the manuscript and performed statistical analysis. XY conceived and designed the research. SW did the CFD simulation. HL designed in-house software. LJ, JL, CL and JF acquired the data.
Funding This work was supported by the National Natural Science Foundation of China (grant nos 81301003, 81371315, 81171079, and 81220108007), Special Research Project for Capital Health Development (grant no 2014-1-1071), and the Youth Fund of Beijing Neurosurgical Institute (grant no 2014-001).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors agree to share any data on request. Any data from this study are available by contacting the corresponding author.