Article Text

Abstract
Background Treatment of selected wide-neck internal carotid artery (ICA) bifurcation aneurysms remains challenging for clip reconstruction and for endovascular options.
Objective To describe a new endovascular treatment technique for wide-neck ICA bifurcation (ICAb) aneurysms.
Methods We have employed a treatment approach that uses both complete proximal occlusion and reversal of flow in the ipsilateral A1 segment, using different endovascular modalities such as coils, stent-assisted coiling, or flow diverters (FDs) plus coiling concomitantly. This endovascular technique may overcome the challenges of current treatments and high recanalization rates for coiled ICAb aneurysms.
Results We treated four patients in whom we redirected the pre-existing flow in the supraclinoid ICA into the ipsilateral A1 and M1 segments, to a new unilateral, linear flow from the supraclinoid ICA solely into the ipsilateral M1 segment. This resulted in the establishment of flow from the contralateral A1 segment into the ipsilateral A1 segment, allowing supply of only demanding perforating arteries on this specific (ipsilateral) segment. This technique was not associated with any new neurological deficits or radiographic ischemia. The four patients reviewed were all treated using coils. One was treated with a standard stent. The other two were treated with a FD.
Conclusions We found that the proposed technique of flow modification can allow for hemodynamic conversion of ICAb to ‘side-wall’ aneurysm. In patients with good collateral flow through the anterior communicating complex, this treatment paradigm is safe and effective.
Statistics from Altmetric.com
Introduction
The treatment of wide-neck, large internal carotid artery bifurcation (ICAb) aneurysms remains challenging. Microsurgical clipping has historically been the standard treatment. Clipping of large and dysmorphic ICAb aneurysms may be associated with significant morbidity, due to the challenging dissection of regional perforators and the potential attenuation of the caliber of the proximal M1 and A1 segments after clip closure.1–3 Endovascular treatment carries its own risks. The coiling of ICAb aneurysms has a higher recurrence rate as compared with side-wall aneurysms, requiring a longer follow-up period.4 Advanced endovascular techniques, such as stent-assisted coiling, Y stenting and balloon remodeling, are used to enhance treatment longevity.5–8
We describe a paradigm for endovascular treatment of wide-neck ICAb aneurysms associated with appropriate anatomic collateral configurations. We suggest a flow modification in the anterior cerebral artery (ACA)–anterior communicating artery (ACoA) complex, leading to hemodynamic conversion of the ICAb aneurysm into a ‘side-wall’ aneurysm. This alteration in flow characteristics is achieved by occluding the A1 segment origin at the aneurysmal sac or, alternatively, using a flow diverter (FD) to cover the origin of the A1 segment. By this technique we safely reduce both the complexity of the treatment and, theoretically, reduce the risk of aneurysm recurrence.
Methods
Four patients with incidental ICAb aneurysms were treated by the proposed endovascular technique of flow modification. We retrospectively reviewed the clinical presentation, imaging, and follow-up clinical and radiographic data of all patients.
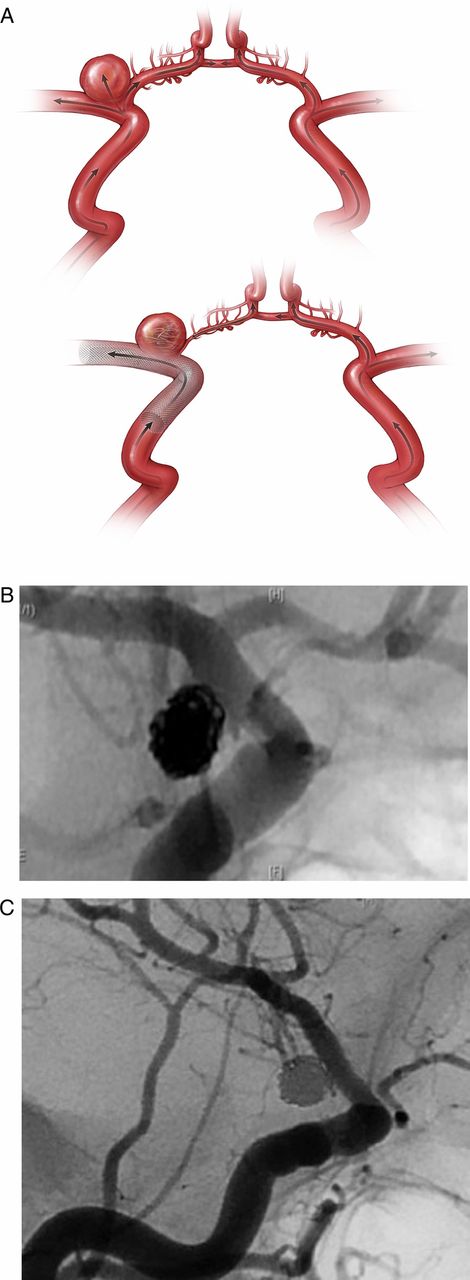
Our proposed technique of flow diversion in the ACA–ACoA complex is based on prior experience with patients harboring supraclinoid ICA aneurysms (at the posterior communicating artery and the anterior choroidal artery), where FDs were used extending from the supraclinoid carotid artery to the M1 segment. In this cohort we observed a reversal of flow, characterized by retrograde filling of the ipsilateral A1 segment from the contralateral A1 segment through the ACoA. Regression in size of the ipsilateral A1 segment was found when compared with the immediate post-procedure angiographic studies, while the medial lenticulostriate arteries on the ipsilateral A1 segments maintained persistent patent flow (figure 1).
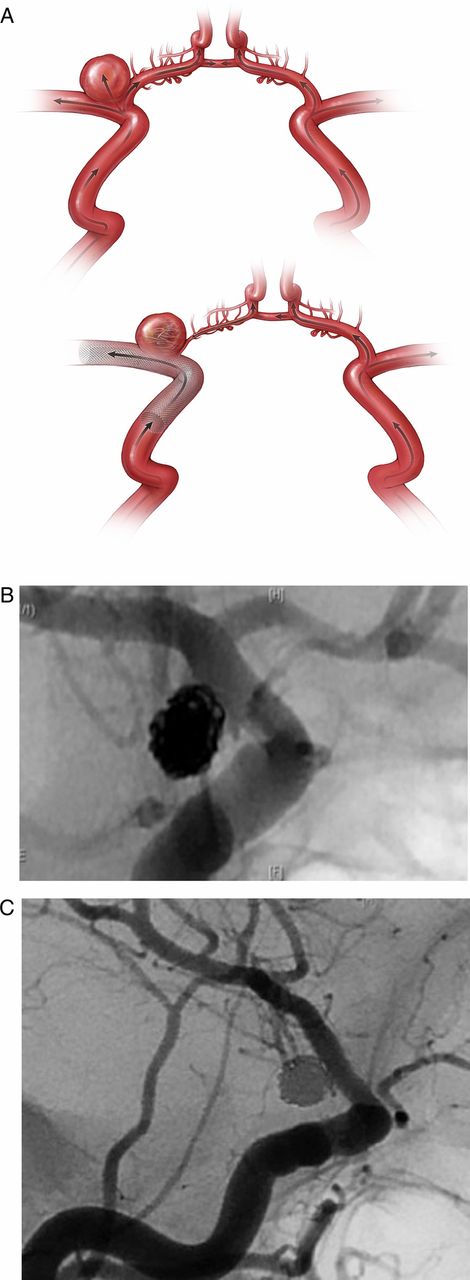
(A) Artist's rendering of an internal carotid artery bifurcation aneurysm treated with coils and a Pipeline embolization device (PED) demonstrates the concept of size regression and reversal of flow in the ipsilateral A1 segment. (B) An anterior choroidal artery wide-neck aneurysm, treated with coil embolization and one PED, covering the right A1 segment. Post-embolization injection demonstrates filling of a large A1 segment through the PED. (C) Six-month follow-up angiography demonstrates complete aneurysmal occlusion with no antegrade filling of the ipsilateral A1 segment through the flow diverter.
Preoperative preparation and procedure
Patients treated with stents were started on dual antiplatelet therapy. A P2/Y12 assay was obtained to evaluate the reaction to dual antiplatelet treatment.
A four-vessel angiogram was obtained, including three-dimensional (3D) reconstructed images. A thorough angiographic assessment of flow dynamics in the circle of Willis, with emphasis on the bilateral ACAs and the ACoA complex, was performed. We evaluated the collateral flow from the contralateral A1 segment through the ACoA into both A2 segments, and the retrograde flow, across the midline, into the ipsilateral A1 segment. If the standard angiographic assessment was not conclusive, we used cross-compression of the ipsilateral cervical common carotid artery (CCA) with concomitant contralateral CCA injection. This allowed visualization of the expected reversal of flow in the A1 segment–ACoA complex.
All procedures were performed by the standard transfemoral approach under full heparinization using the combination of platinum and hydrogel coils. Different stents were used including the Enterprise (Codman & Shurtleff, Raynham, Massachusetts, USA) and the Pipeline embolization device (PED; ev3 Neurovascular, Irvine, California, USA).
Results
Case 1
A middle-aged patient with an incidental, multilobulated, left ICAb aneurysm (9 mm×8 mm, neck 4.5 mm), incorporating the proximal ipsilateral A1 segment, was evaluated. Assessment of the ACoA complex flow dynamics revealed a smaller size ipsilateral A1 segment in comparison with the contralateral A1 segment, with robust filling of both ACAs and filling of the left A1 segment across the ACoA via the contralateral, right A1 segment.
A right-side CCA injection, with left (ipsilateral) cervical CCA compression showed good collateral flow through the ACoA, filling the left A1 segment, the aneurysm, and the left middle cerebral artery (MCA). In view of these findings, we did not use balloon test occlusion (BTO).
An 18 mm platinum frame coil was deployed within the aneurysm and across the neck without coil detachment. Subsequently, an Enterprise stent was deployed from the M1 segment to the supraclinoid ICA, bridging the aneurysmal neck and ‘jailing’ the microcatheter delivering the coil. A dense coil mass was deployed to the level of the aneurysmal neck bridged by the stent. At the end of the procedure slow antegrade flow to the left A1 was still noted; however, on both the 3-month follow-up magnetic resonance angiography (MRA) and 13-month angiography, the aneurysm was completely occluded, without any antegrade flow in the left A1 segment. This ipsilateral left A1 segment filled robustly in a retrograde fashion via the right A1 segment through the ACoA (figure 2). The patient was neurologically intact immediately after the procedure and on long-term follow-up. No evidence of ischemia was documented on follow-up MRI.
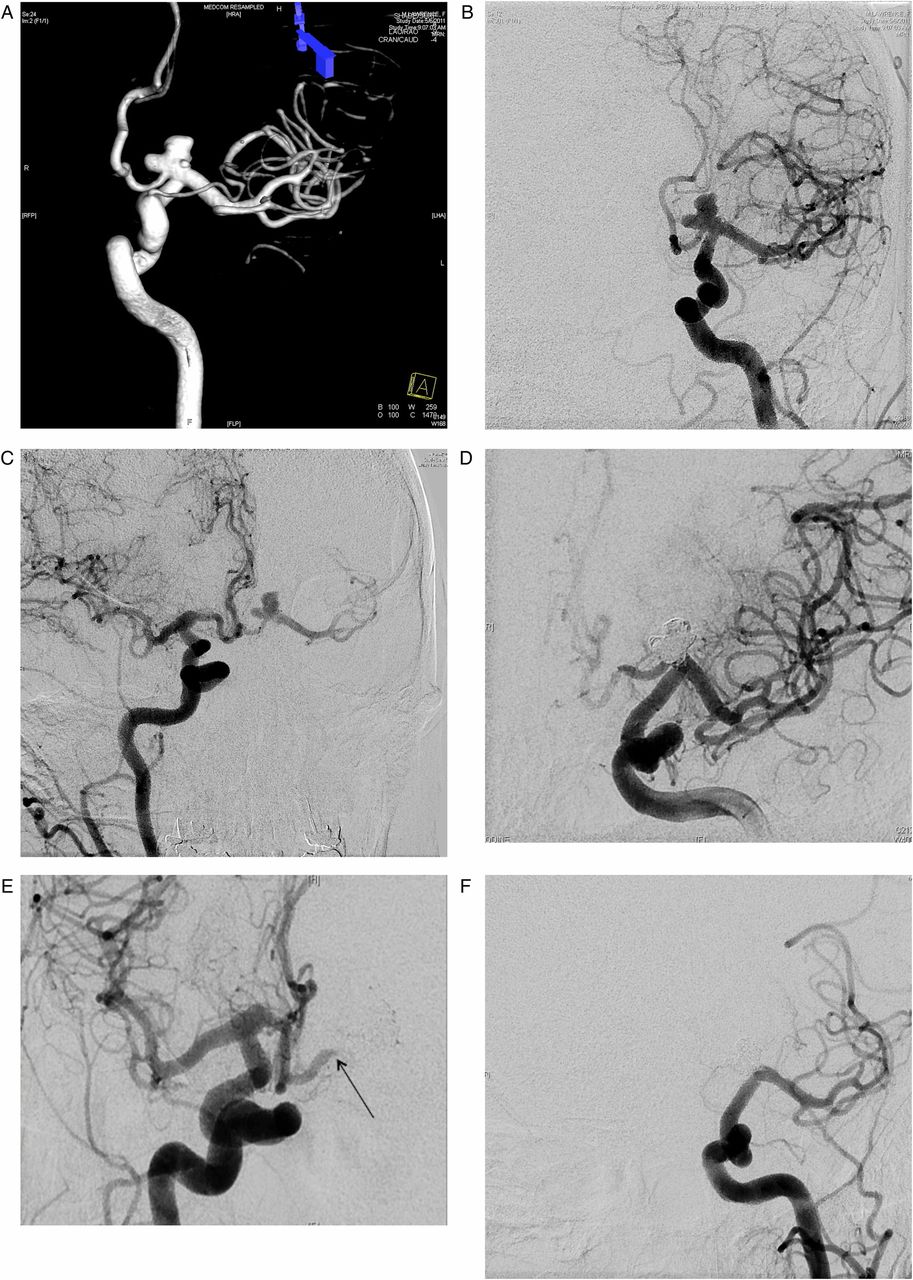
(A) Three-dimensional reconstruction of a left internal carotid artery bifurcation (ICAb) aneurysm incorporating the proximal A1 segment. (B) Left ICA injection demonstrates the ICAb aneurysm. (C) Right contralateral ICA injection demonstrates robust collateral flow to support the left anterior cerebral artery (ACA) as well as retrograde filling of the ipsilateral A1 and M1 segments. (D) Immediate post-coiling angiography demonstrates complete occlusion of the aneurysm and slow flow with residual delayed filling of the A1 segment through the coil mass. (E) Contralateral ICA injection demonstrates robust filling of both ACAs with retrograde filling of the left A1 segment up to the origin off the aneurysm (arrow). (F) Long-term follow-up angiography (13 months) demonstrates complete occlusion of the aneurysm without antegrade filling of the left A1 and without in-stent stenosis.
Case 2
A middle-aged patient was evaluated with an incidental left multilobulated ICAb aneurysm (10 mm × 10 mm, neck 5 mm). The neck incorporated the origin of the left M1 and A1 segments. This aneurysm was associated additionally with a very small (2 mm) left posteriorly projecting A1 aneurysm, and a small (1.5 mm) ipsilateral anterior choroidal artery aneurysm.
An angiographic assessment of the ACoA complex flow dynamics disclosed a large ipsilateral A1 segment. Contralateral, right CCA injection demonstrated robust flow through the right A1 segment to both ACAs. The use of a FD was chosen owing to the multiplicity of the aneurysms, the wide aneurysmal neck incorporating the M1 segment, and finally, owing to the desire to divert flow from the left A1 segment because of the incorporation of this segment into the aneurysmal neck.
A dual microcatheter technique was used to create a coil mass without compromising flow in the A1 and M1 segments. Subsequently, a PED was deployed extending from the supraclinoid ICA to the M1, and simultaneously ‘jailing’ the microcatheter in the aneurysm. Angiographic injection documented immediate flow attenuation in the ipsilateral A1 segment, with filling of only its most proximal portion. Additional coils were deployed until a dense homogeneous mass of coils was achieved. No residual filling of the aneurysm was seen. Control injections confirmed robust flow through the stent, filling the left MCA, complete occlusion of the aneurysm, filling of both ACAs, and retrograde filling of the left A1 segment via the ACoA and the right A1 segment. Five-month follow-up MRA confirmed persistent occlusion of the aneurysms and regression in size of the left A1 segment (figure 3). The patient had a stable clinical course without neurological deficits and without evidence of radiographic ischemia. A long-term follow-up angiographic study is pending.

{kind=link}
{kind=link}
{kind=link}
(A) Two views of 3D reconstructed images of the left internal carotid artery (ICA): a large multilobular left ICA bifurcation aneurysm incorporating the left A1 and M1 segment. Two very small additional aneurysms: left proximal A1 segment (thin arrow) and left anterior choroidal artery aneurysm (thick arrow). (B) Left ICA angiography demonstrates the multilobular large ICA bifurcation (ICAb) aneurysm. Flow is seen through the ipsilateral A1 segment which fills both anterior cerebral arteries (ACAs). (C) Right contralateral ICA injection demonstrates good collateral flow through the anterior communicating artery supporting the left ACA and the ipsilateral A1 segment. (D) Dual microcatheter technique was employed for coil embolization of the wide-neck ICAb aneurysm, while preserving the left A1 segment and M1 segment origins incorporated into the neck. (E) Immediate after deployment of a Pipeline embolization device (PED) with one microcatheter ‘jailed’ within the aneurysm. Immediate flow diversion with minimal antegrade filling of the left A1 is shown. (F) Contralateral ICA angiography demonstrates robust filling of both ACAs with retrograde flow in the ipsilateral A1 segment (filling the perforators) up to the occluded aneurysm (arrow). (G) Three-month follow-up MR angiography confirms complete aneurysmal occlusion, filling of both ACAs and marked size regression of the left A1 segment.
Case 3
A middle-aged patient presented with an unruptured right ICAb/A1 origin aneurysm and a right MCA bifurcation aneurysm. During craniotomy, the MCA aneurysm was clipped, but clipping of the ICAb aneurysm was deferred. After recovery, endovascular obliteration of the ICAb aneurysm was started. A small aneurysmal sac (6 mm) with superior projection and a wide neck incorporating the right A1 segment origin was demonstrated. Review of flow dynamics in the ACA–ACoA complex showed equal sized A1 segments and a patent ACoA. Cross-compression and BTO were deferred. Based on these anatomic findings, coil obliteration of the aneurysm sac, inclusive of the origin of the A1 segment, was performed. Complete obliteration of the aneurysm was achieved concomitant with total occlusion of the ipsilateral A1 ostium, with total retrograde filling of the right A1 segment and antegrade filling of the right ACA via the left A1 segment through the ACoA. The patient was stable neurologically on a short-term follow-up but was lost to follow-up, and thus no long term follow-up imaging was obtained.
Case 4
A middle-aged patient underwent coil obliteration of a ruptured right anterior choroidal artery aneurysm at an outside institution. After complete recovery this patient was lost to follow-up. Cerebral angiography 8 years after the initial procedure demonstrated recanalization of the aneurysm, as well as a 5 mm dysplastic aneurysm at the right ICAb. Angiographic assessment of the ACA–ACoA complex demonstrated equal size of both A1 segments and robust filling of the ACoA. Endovascular coiling of the patent luminal portion of the anterior choroidal artery aneurysm was performed. A PED was deployed extending from the mid-supraclinoid carotid—bridging the aneurysmal neck and the dysplastic ICAb aneurysm at the ICA bifurcation—to the proximal M1 segment. Postembolization studies demonstrated occlusion of the previously ruptured aneurysm and no change of flow through the right A1 segment, without immediate flow changes in the ICAb aneurysm. No immediate neurologic deficits were noted. Follow-up (3 months) MRA demonstrated regression of the ipsilateral A1 segment and reduction of the ICAb aneurysmal size, without complete occlusion. Long-term angiography is pending.
Overall outcome
All patients demonstrated reversal of flow/regression of the ipsilateral A1 segment up to the level of the ICAb aneurysmal neck. Three patients who were treated using coil embolization demonstrated complete occlusion of the aneurysm. One patient with a dysplastic aneurysm, who was treated with one PED and no additional coils, demonstrated regression on the 3-month follow-up imaging. Eliminating the flow into bifurcation aneurysms as outlined still allows for maintenance of patency of all critical vessels and perforators through the process of flow reversal. No ischemic changes were seen radiographically in the territories of the medial or lateral lenticulostriate arteries. All cases showed good flow into the ipsilateral medial lenticulostriate arteries from the contralateral A1 segment.
Discussion
Treatment options for ICA bifurcation aneurysms
ICAb aneurysms represent 2–9% of all intracranial aneurysms. Possible treatments for these aneurysms are microsurgical clipping or endovascular coiling.1–3 ,9 ,10 Microsurgical clipping results can be affected by inappropriate manipulation or occlusion of perforators and end-arteries such as the anterior choroidal artery, the recurrent artery of Heubner, the medial and lateral lenticulostriate arteries and perforators emerging from the ICAb itself.1 Additionally, higher intraoperative rupture rates and higher mortality rates were documented for these lesions in comparison with other microsurgically treated anterior circulation aneurysms.2
Endovascular treatment of ICAb aneurysms can be accomplished by different techniques, such as balloon remodeling, stent-assisted coiling, and the dual microcatheter technique.9 These modalities may be efficacious; however, the long-term recanalization rates in this modality remain a significant limitation.9 ,10
Y stenting techniques have been described in the treatment of ICAb aneurysms and for basilar artery bifurcation aneurysms. The periprocedural complication rate in balloon-assisted coiling or in Y stenting is relatively high (11–31.6%) with a documented retreatment rate of 10%.8 ,11 A ‘cross-over’ stent technique requiring covering of the distal supraclinoid ICA, has also been described for ICAb aneurysms. This modality may be associated with vessel occlusion or distal emboli. Additionally, this technique requires an anatomic angio-architecture with a patent and robust ACoA and bilateral A1 segments with appropriate diameters.12 ,13
Modifying flow to treat aneurysms
Historically, ‘deconstructive’ procedures for the treatment of aneurysms, such as surgical ICA ligation, were used until the beginning of the 1970s. Endovascular occlusion of an aneurysm with the parent vessel, when feasible, achieved complete occlusion and early reduction of mass effect in large aneurysms. However, a series of 461 patients treated in this way had a significant mortality rate of 20.7% and stroke rate of 30%.14 With the advent of sophisticated microsurgical clipping and endovascular techniques, carotid ligation and parent vessel occlusion have essentially been abandoned. Technological advances now allow endovascular obliteration when indicated, including both stent-assisted coiling and more recently, the use of FDs.
Modifying flow with FDs
FDs have been recently reported to modify and redirect flow and thus to be a possible treatment for wide-neck aneurysms.15 Several important reported examples demonstrate flow modification in adjacent branch vessels distinct from the parent vessel itself using a FD. The patency of the ophthalmic artery after treatment of paraclinoid aneurysms with FDs deployed into the ICA was examined. In this cohort, 21% of the ophthalmic arteries were occluded, all without visual changes or clinical symptoms. Two patients who had ophthalmic artery occlusion demonstrated collateral retrograde flow into the ophthalmic artery. The flow and vascular contribution of these more distal collateral vessels might explain the increased tendency for proximal occlusion of branch vessels, such as the ophthalmic artery, when using FDs.16 Lack of distal collateralization—or persistent ‘demand’—allows branch vessels, such as the anterior choroidal artery, to stay patent when ‘covered’ by a FD. Based on these concepts, the placement of a FD was described recently for the treatment of distal MCA giant aneurysms. The authors describe the deployment of the FD in the competitive vessel distal to the parent vessel of the aneurysm, thus ‘covering’ the vessel harboring the lesion. In long-term follow-up studies, the parent vessel and aneurysm were occluded with reconstitution of the distal territory by pial leptomeningeal collaterals.17 However, importantly, when there is a flow/pressure gradient, critical perforators and end-arteries will remain patent, if covered by a FD.16
Modifying flow to treat ICAb aneurysms
Based on these concepts, we have conceptualized an endovascular technique to modify and redirect flow in the region of the ICAb. This technique deals with two inherent difficulties of endovascular treatment of wide-neck aneurysms in this location: the complexity of Y stenting or balloon-assisted coiling techniques, and the increased recurrence risk often seen in long-term follow-up. We observed flow modification in the ACA–ACoA complex using a single FD extending from the supraclinoid ICA to the proximal M1 segment. Supraclinoid ICA aneurysms treated in this fashion showed early or delayed reversal of flow in the ‘covered’ A1 segment, with size regression and retrograde filling through the ACoA. This flow modification clearly depends on the caliber of the contralateral A1 segment and the patency of the ACoA. These critically important angiographic and flow characteristics define the capacity of the collateral circulation to achieve adequate flow reversal (figure 1). To assess these characteristics, we evaluated the flow across the ACoA segment and the concomitant filling of both A2 segments from the contralateral ICA injection on standard angiography or during compression of the ipsilateral cervical carotid with concomitant contralateral carotid injection. If this assessment is still inconclusive, formal ipsilateral BTO with contralateral injection may be efficacious.
We describe two distinct endovascular techniques to treat wide-neck ICAb aneurysms based on the same concept and paradigm of flow modification in the anterior circle of Willis: 1. Focal occlusion of the origin of the A1 segment with the aneurysmal sac. Here, we rely on immediate competence of collateral flow from the contralateral A1 segment through the ACoA complex. 2. The use of a FD in combination with coil embolization to occlude the aneurysmal sac. In this second technique, we advocate the use of a single FD only to reduce the risk of anterior choroidal artery and lenticulostriate artery occlusion. Both these endovascular techniques achieve the same desired efficacious alteration of flow.
Study limitations
Our case series includes only four patients who were treated with different endovascular modalities. In all patients discussed we based our treatment on the same unifying concept of flow reversal, which resulted in the hemodynamic conversion of a bifurcation aneurysm into a ‘side-wall’ aneurysm. We present here only mid-term follow-up, particularly with respect to angiographic follow-up of the flow modification achieved. Average vascular imaging (MRA/angiography) follow-up in our series was 7 months. Formal angiographic longevity is yet to be assessed and compared with other possible treatments. Additionally, this technique may be problematic in the presence of acute subarachnoid hemorrhage. Vessel occlusion or flow modification may increase the risk of ischemia in the setting of vasospasm. Also, limitations to the use of antiplatelet agents in this setting have been well described.
Conclusions
Alteration of flow in the ACA–ACoA complex, when the collateral anatomy is favorable, allows hemodynamic conversion of the flow characteristics of ICAb aneurysms to those of ‘side-wall’ aneurysms. This anatomic flow modification did not result in any observable ischemic changes radiographically or new neurologic deficits after treatment. Continuing clinical and radiographic review of future patients treated with this flow alteration technique is necessary.
References
Footnotes
-
Contributors EN, DJC, AS: substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work. Drafting the work or revising it critically for important intellectual content. Final approval of the version to be published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. ML: final approval of the version to be published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
-
Competing interests None.
-
Ethics approval Institutional review board North-Shore.
-
Provenance and peer review Not commissioned; externally peer reviewed.