Article Text

Abstract
Objective: To assess stroke awareness among patients presenting to the emergency department with an acute ischaemic stroke or transient ischaemic attack (TIA).
Methods: A consecutive cohort of patients presenting with a cerebrovascular event was prospectively enrolled over a 15-month period and questionnaires were administered. If the patient was unable to respond to the questions or answer the questionnaire, it was administered to the primary caregiver. Comprehension of having a cerebrovascular event, reason for delay in presentation, mode of arrival and knowledge of treatment modalities were determined.
Results: Only 42% of 400 patients thought they were having a stroke or TIA. The median time to presentation was 3.4 h. Delayed presentation was almost equal in men and women. When asked about onset, 19.4% thought that a stroke came on gradually and only 51.9% thought immediate presentation was crucial. 20.8% of patients had heard of thrombolysis.
Conclusion: Community knowledge of ischaemic stroke needs to be enhanced so that individuals present earlier, leading to timely management.
Statistics from Altmetric.com
Ischaemic stroke causes an increase in functional disability and a decrease in quality-adjusted life years.1 Increased knowledge and awareness of the condition would potentially improve prevention, risk factor control and early presentation to a healthcare centre. The American Stroke Association found that only 2% of the US population cite stroke as the disease or health condition concerning them the most, and 50% of adults do not even believe they are at risk for stroke.2
Ischaemic stroke is the third leading cause of death worldwide, and the annual number of deaths due to stroke is roughly 5 million.3 Every year there are about 750 000 new strokes in Europe and a similar number in the USA.4 In addition, one-third of people who survive a stroke will have a recurrence. Stroke is not restricted to developed countries and recent surveys show that it is also a major health problem in developing countries.3 Since ischaemic stroke is associated with an increase in functional disability and a decrease in quality-adjusted life years,5 increased knowledge and awareness of the condition would potentially improve functional outcomes.
The objective of this study was to assess knowledge and to determine the awareness and public understanding in our region. Our study targeted patients presenting to the emergency department with an acute ischaemic stroke or transient ischaemic attack (TIA).
METHODS
Study design and patient enrolment
The study was conducted at a tertiary referral academic medical centre with an annual emergency department census of 77 000. A consecutive cohort of patients who presented to the institution with a probable diagnosis of acute ischaemic stroke or TIA over a 15-month period from July 2005 to September 2006 was prospectively enrolled. Patients admitted through the emergency department were enrolled in real time; all others were enrolled within 24 h of presentation. We chose this cohort over a group within the community so that we could get a first-hand account of the reasons for delayed presentation following symptoms, as well as an estimated time of delay.
Written informed consent was obtained prior to enrolment and approval was granted by the institutional review board.
Methods of measurement
A 30-point questionnaire designed to assess comprehension of having a cerebrovascular event, reason for delay in presentation, awareness of early presentation and treatment modalities was administered. In instances where the patient was unable to complete the questionnaire owing to unresponsiveness or aphasia, the survey was administered to the primary caregiver of the patient.
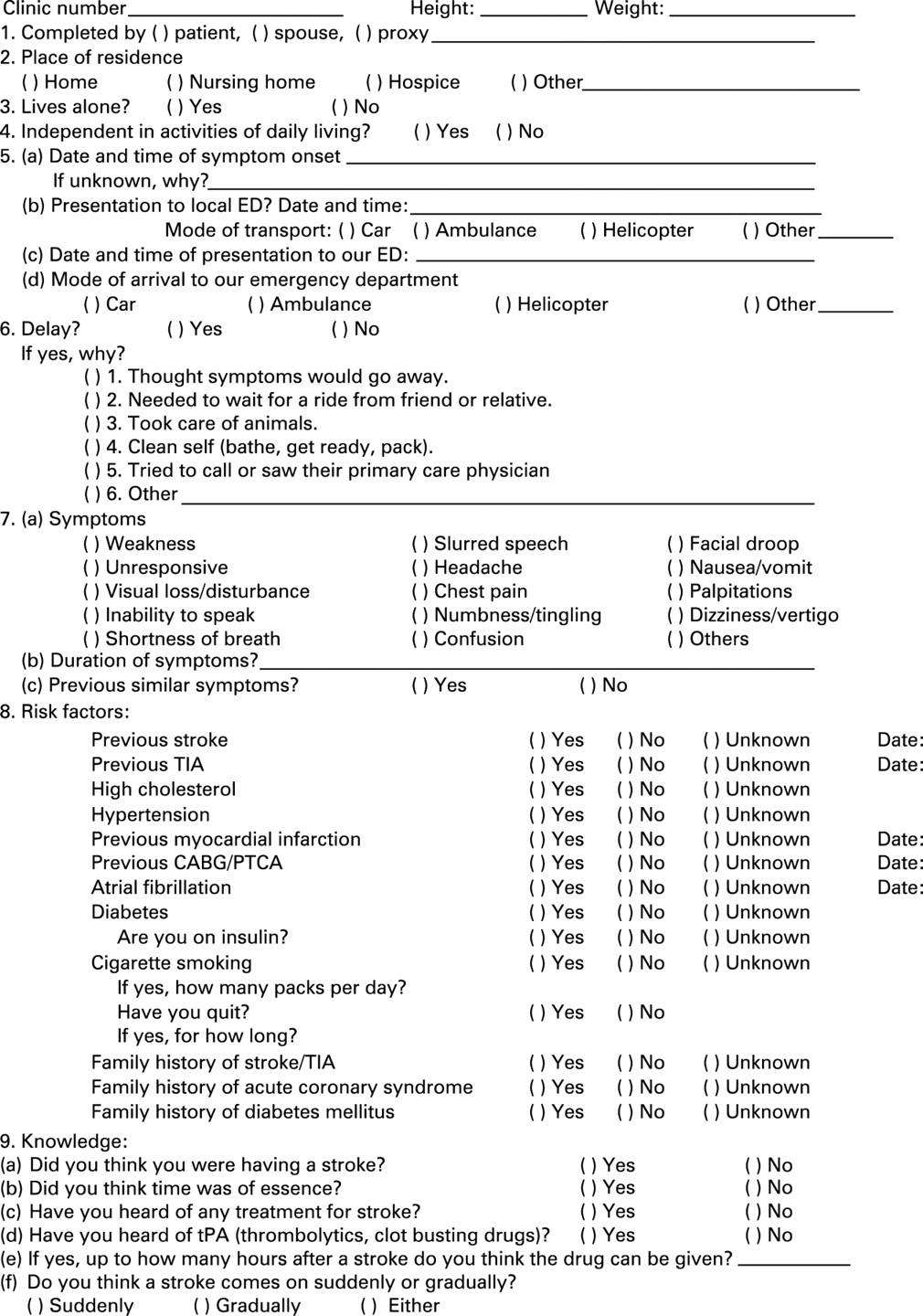
Knowledge of having a cerebrovascular event was assessed. The time to presentation was documented and the reasons for delay, if any, were recorded verbatim. Awareness of symptoms, onset of stroke, treatment modalities including thrombolytic therapy and importance of early presentation were recorded (fig 1). Demographic factors such as age and sex were recorded for each patient and information on the presence of risk factors was abstracted. A family history of stroke or TIA, coronary artery disease and past medical history of a stroke, TIA, hyperlipidaemia, hypertension, myocardial infarction, atrial fibrillation and smoking were considered potential risk factors.3 4

{kind=link}
Analysis of data
The data collected were tabulated and statistical analyses performed using JMP software Version 6.0 (SAS Institute, Chicago, Illinois, USA).
Univariate and contingency analyses were used to determine the relationship between components of stroke knowledge, awareness, risk factors and demographic variables. The type I error rate was set at 0.05, and p values reported were obtained using analysis of variance (ANOVA) and Pearson χ2 tests. The results were summarised as percentages and odds ratios (ORs) with 95% confidence intervals (CIs). Since the time from onset to presentation at the emergency department did not lend itself to a normal distribution, the non-parametric methods of Wilcoxon/Kruskal-Wallis rank test were used for these analyses.
RESULTS
Demographic data and risk factors
Of a total of 400 patients enrolled in the study (294 with stroke, 106 with TIA), 55.5% were men. The mean (SD) age of the studied population was 69.1 (15.6) years. Only 27% of the patients were unable to answer the questionnaire themselves and in these cases the survey was completed by proxy.
Data were collected on the residence and baseline functional level of the patients: 92.8% resided at home and 4.8% in a nursing home or assisted living facility; 26.3% lived alone and 95% were independent in their activities of daily living prior to the event (table 1).
Approximately one-fifth of the cohort had suffered from a stroke (21%) or TIA (19%) prior to the current event.
Box 1 Patients’ reasons for delayed presentation to the emergency department
“I did not want anyone to find out”
“Ambulance did not run in the daytime in our town and I had to call neighbouring community’s ambulance”
“It happened while we were sleeping and I did not know it was happening”
[Patient] on the streets; no one noticed a difference in his speech or demeanour
“Did not want to come in on Saturday because I thought the ER would be too busy”
“I wanted to watch the play-offs”
[Patient] was alone and passed out
[Patient] was found unresponsive the next morning
“Ambulance people stated it wasn’t my symptoms were not concerning. They had sent the other EMT down to the ambulance for a break. In the meantime [patient] became unresponsive and the EMT in the apartment had to try and get the other EMT back to the apartment. He wouldn’t answer his radio so they had to go through the dispatcher to get him back to the apartment”
[Patient] was obese and had a size issue
“Ambulance could not find my address”
“I fell and couldn’t get to the phone so I waited for someone to come”
[Patient] in denial about having a stroke, refused EMS transport even though wife had called promptly
“I didn’t want to come without a friend in case I would die in the hospital alone”
“I didn’t see the point of coming; last time I had a stroke they kept me for 4 days and sent me home on an aspirin”
“I have had a bum left arm for months, I figured it was just that”
Presentation
Although 73.5% of the group had ischaemic strokes, 58% did not think they were having a stroke following symptom onset. With regard to their mode of arrival at the hospital, 54.3% were transported by ambulance, 42% by car and 2% were airlifted (table 1). The patients who were transported by ambulance or helicopter had a significantly shorter time from onset of symptoms to presentation (p = 0.003). The time to presentation following onset of symptoms ranged from 10 min to 192 h with a median time of 3.37 h (interquartile range (IQR) 1.3–11.8). The median time to presentation was 2.37 h (IQR 1.0–7.7) for those who came by ambulance or helicopter and 4.5 h (IQR 1.5–14.5) for those who came by car. A total of 135 patients (33.8%) presented within 2 h of symptom onset (96 (32.7%) of the 294 patients with ischaemic stroke and 39 (36.8%) of the 106 with TIA). Less than half of the cohort (48.3%) presented within 4 h; 136/294 (46.3%) with ischaemic stroke and 57/106 (53.8%) with TIA. The most common cause of delay was the patient thinking that the symptoms would go away (16%). Some of the reasons given by patients for delayed presentation to hospital are shown in box 1.
Stroke awareness
When asked if a stroke came on suddenly or gradually, 62% felt it was sudden, 19.4% thought it was gradual, 3.8% said it could be either and 14.6% were unsure; 45.3% felt time was not of essence in presentation after a stroke. When asked about treatment modalities, only 20.8% had heard of thrombolytic therapy even though almost one-fifth of the cohort had a history of previous stroke or TIA. Other modes of treatment volunteered were aspirin, blood thinners, exercise and rehabilitation. None of the patients had heard of mechanical intervention for stroke. Of the patients presenting with acute ischaemic stroke, 10 (3.4%) received thrombolytic therapy.
Patients with a prior stroke were 0.93 times more likely to think that time was of essence (95% CI 0.63 to 1.36) and 1.28 times more likely to know they were having a stroke (95% CI 0.87 to 1.87).
Analysis of variables
We found no difference in the time of presentation between the sexes (p = 0.58). A positive family history of a cerebrovascular event had no effect on the time to presentation (p = 0.48). There was no difference in the knowledge of thrombolytic therapy (p = 0.68), awareness of early presentation (p = 0.81) or other treatment modes (p = 0.46) with respect to age or sex. Individuals who thought they were having a stroke (p<0.0001), those who thought time was of essence (p<0.0001) and those who had heard of thrombolytic therapy (p = 0.025) or other treatment for stroke (p = 0.004) were significantly more likely to present earlier.
DISCUSSION
With the increasing incidence in ischaemic stroke, numerous studies have been conducted to investigate patient awareness, delay in presentation and prehospital time for acute ischaemic strokes.5–7 Lack of community awareness has always been considered to be one of the major causative factors for delayed presentation.8–10 Education programmes for the public to improve their knowledge of acute stroke symptoms have played a major role in the quest for improving timely presentation.
Thrombolysis is known to reduce the severity of ischaemic strokes when given within 3 h of the onset of symptoms of stroke,11 but most patients fail to present to medical services within this short “window of opportunity”. Treatment with intravenous tissue plasminogen activator was underused in a hospital-based stroke registry,12 and the primary reason for this non-treatment was found to be delayed presentation.13
A European study showed that, although 40% of a study population recognised they were having a stroke, almost 80% called their primary care physician rather than an ambulance.14 This suggests that there was a void between the knowledge of symptoms and the awareness of imminent risk and early presentation.
Although the Copenhagen study showed that signs and symptoms of a severe stroke favour early presentation at hospital,7 it was proposed that a history of illness probably contributed to heightened awareness of symptoms of a cerebrovascular event and increased knowledge of care.15 A study which compared the knowledge of stroke between the general public and patients who had already had a stroke found that there was little difference between the groups.16 A few trials have reported a correlation between haemorrhagic stroke and early presentation.17 18 Our patient cohort included only those with ischaemic stroke and TIA. Since most strokes are ischaemic in aetiology, it is necessary to improve awareness of the importance of early presentation considering the advent of time-dependent treatments such as thrombolysis and mechanical embolectomy.
Implications
Education of patients who have presented to a healthcare facility is vital as our study showed that although more than one-fifth of the cohort had had a previous stroke, awareness was not improved. Further research is also required to establish cost effective measures to educate the public and reiterate the importance of early presentation. We accept that improving community knowledge alone might not be sufficient to improve timely and appropriate acute and preventive stroke care. Many other factors such as training of emergency medical technicians, timely transfers, emergency department staff training and fast track in hospital systems to streamline acute stroke care to stroke care units are essential.
Limitations
Our study was restricted to a single academic centre and the population was predominantly Caucasian. While one might consider that a region receiving medical care by a large academic centre might have a higher level of awareness, it was not suggested by this study. Although our patient population may be older and not representative in age of the general population, they are more prone to developing the disease and hence should be targeted for stroke education. In patients who were unable to complete the questionnaire, the primary carer (most often the spouse) was requested to respond (27%). Although we understand that this may not reflect the patient’s knowledge, we feel it is important as patients often turn to their caregiver for assistance. The results presented might also suggest that, to improve knowledge, education should be targeted to a wider audience as well as to those at risk of stroke.
The other major limitation of the study is that it only included those who actually did present to the hospital with a stroke. We cannot account for those who had a stroke and did not seek medical attention, a population that unfortunately does still exist. Although we did administer education packages to these patients, the impact of this has not yet been reported.
CONCLUSIONS
The knowledge of thrombolytic therapy and its “time window” in the general community needs to be improved so that individuals present earlier with their symptoms. Factors such as training of emergency medical technicians, timely transfers, emergency department staff training and fast track in hospital systems to streamline acute stroke care to stroke care units are also essential to reduce the intensity and disability of an otherwise morbid disease.
REFERENCES
Footnotes
Funding: None.
Competing interests: None.
Ethics approval: Written informed consent was obtained prior to enrolment and approval was granted by the institutional review board.