Article Text

Abstract
Objective Intracranial atherosclerosis is a major cause of ischaemic stroke worldwide. A number of studies have shown the effects of statin treatment on coronary and carotid artery plaques, but there is little evidence on the effects of statin treatment on intracranial atherosclerotic plaques.
Methods The Intensive Statin Treatment in Acute Ischaemic Stroke Patients with Intracranial Atherosclerosis - High-Resolution Magnetic Resonance Imaging (STAMINA-MRI) Trial is a single-arm, prospective, observational study monitoring imaging and clinical outcomes of high-dose statin treatment among statin-naive patients with acute ischaemic stroke caused by symptomatic intracranial atherosclerosis. The primary outcome was the change in vascular remodelling and plaque characteristics before and after 6 months (median: 179 days, IQR 163–189 days) of statin treatment measured by high-resolution MRI (HR-MRI).
Results A total of 77 patients (mean age: 62.6±13.7 years, 61.0% women) were included in this study. Low-density lipoprotein cholesterol (LDL-C) levels (mg/dL) at initial and follow-up assessments were 125.81±35.69 and 60.95±19.28, respectively. Overall, statin treatment significantly decreased enhancement of plaque volume (mm3, 32.07±39.15 vs 17.06±34.53, p=0.013), the wall area index (7.50±4.28 vs 5.86±4.05, p=0.016) and stenosis degree (%, 76.47±20.23 vs 64.05±21.29, p<0.001), but not the remodelling index (p=0.195). However, 35% patients showed no change or increased enhancement volume and stenosis degree after statin treatment. Higher reduction of LDL-C and longer duration of statin treatment were associated with decreased enhancement volume after statin treatment.
Conclusions High-dose statin treatment effectively stabilised symptomatic intracranial atherosclerotic plaques as documented by HR-MRI. Further study is needed to determine laboratory and genetic factors associated with poor response to statins and alternative therapeutic options, such as proprotein convertase subtilisin-kexin type 9 inhibitors, for these patients.
Trial registration number ClinicalTrials.gov NCT02458755.
- cerebral infarction
- stroke
- statins
- intracranial atherosclerosis
- high-resolution MRI
Statistics from Altmetric.com
Introduction
Intracranial atherosclerotic disease (ICAD) is a major cause of ischaemic stroke worldwide and is more prevalent in Asians and Blacks than in Caucasians.1 ICAD is associated with a high risk of recurrent stroke, particularly in individuals with severe stenosis and those experiencing recent ischaemic events.2–4 Several therapeutic strategies for symptomatic intracranial stenosis have been proposed and evaluated. First, there have been efforts to prevent thromboembolism using antithrombotics, but these had limited effects on the stabilisation of vulnerable atherosclerotic plaques.2 3 5 Second, percutaneous transluminal angioplasty and stenting have been tested for the prevention of thromboembolism and the restoration of blood flow.6 7 However, these are not recommended due to the high risk of peri-procedural stroke. Lastly, aggressive medical management of risk factors by targeting low-density lipoprotein cholesterol (LDL-C) to below 70 mg/dL, systolic blood pressure to below 140 mm Hg and the adoption of a comprehensive lifestyle modification programme are recommended.
The ability of statins (3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors) to stabilise symptomatic atherosclerotic plaques and prevent them from rupturing has also been demonstrated in symptomatic coronary arteries8–10 and extracranial carotid arteries.11 Randomised controlled trials evaluating statins have shown that intensive lipid lowering by statins reduced the progression of coronary atherosclerosis on serial intravascular ultrasound evaluations.12 A meta-analysis of randomised controlled trials showed that statin therapy decreased the rate of carotid atherosclerosis progression over the long term as measured by serial carotid duplex scans.13 Pre-stroke statin use has been reported to modulate plaque enhancement in symptomatic intracranial atherosclerosis.14 However, a paucity of data currently exists regarding the long-term effects of high-dose statin treatment on the stabilisation of vulnerable intracranial plaques. Vessel wall imaging techniques, such as high-resolution MRI (HR-MRI) has recently been introduced, which can illustrate the morphology of atherosclerotic plaques, arterial walls and surrounding structures in the intracranial arteries, beyond simple luminal changes.15 To date, only luminal changes (serial magnetic resonance angiography (MRA) or conventional angiography) with statin therapy have been studied in patients with ICAD.16 17
Thus, we conducted a single-arm, prospective, serial HR-MRI study in statin-naive patients with acute symptomatic ICAD to evaluate the efficacy and safety of high-dose statin treatment for 6 months. The investigators hypothesised that high-dose statin treatment during the acute period of ischaemic stroke could result in stabilisation of symptomatic intracranial plaque and regression of arterial stenosis without serious complication to these patients.
Materials and methods
Study design
The Intensive Statin Treatment in Acute Ischaemic Stroke Patients with Intracranial Atherosclerosis - High-Resolution Magnetic Resonance Imaging (STAMINA-MRI) Study is a single-arm, prospective, observational study, monitoring imaging and clinical outcomes of high-dose statins (atorvastatin 40–80 mg and rosuvastatin 20 mg) in symptomatic intracranial atherosclerosis. In this study, a high-dose statin was used as high-dose statins possess additional anti-inflammatory and antioxidant effects compared with moderate-intensity to low-intensity statins and may lead to greater plaque regression.18 Patients were recruited from December 2011 through June 2017 from a university hospital. The sample size required to demonstrate a representative effect of high-dose statins on changes in vascular characteristics of symptomatic intracranial stenosis after 6 months of the treatment could not be assumed due to lack of previous literature. The authors planned to enrol 80 patients considering the recruitment period and the available study funds. The protocol and consent forms were approved by the institutional review board (SMC-IRB No. 2014-10-085). All patients provided signed informed consent prior to enrolment.
Patients with acute ischaemic stroke within 7 days of symptom onset, who had symptomatic intracranial artery stenosis (above 50%) at the proximal portion of the middle cerebral artery (MCA), basilar artery or at the intracranial portion of the internal carotid artery, but not receiving statins were recruited for this study. Patients with extracranial artery (carotid artery bifurcation, proximal vertebral artery) stenosis above 50%, stroke attributable to cardioembolic origin (atrial fibrillation, valvular heart disease or aortic arch atheroma) and severe hepatic or renal dysfunction were excluded.
Patients who met the inclusion and exclusion criteria underwent the 6-month high-dose (atorvastatin 40–80 mg or rosuvastatin 20 mg) statin protocol. All patients were examined by HR-MRI before and after statin treatment. Pre-specified endpoints were measured after 6 months of statin treatment. The primary endpoint was the change in vascular characteristics before and after statin treatment measured as (1) stenosis degree, (2) remodelling index, (3) wall area index and (4) enhancement volume of atherosclerotic plaque on HR-MRI. Secondary endpoints included the following: (1) changes in serum biomarkers including liver function tests, fasting glucose, lipid profiles, lipoprotein(a), apolipoprotein A1 and apolipoprotein B and (2) clinical outcomes including the modified Rankin scale (mRS) score at 3 months and recurrent stroke, transient ischaemic attack or all-cause death occurring during the 6-month follow-up.
High-resolution MRI
HR-MRI was performed using a 3-Tesla system (Achieva; Philips Medical System, Best, Netherlands) with a standard eight-channel head coil. The neuroradiologist (JC) selected the vessel and site of evaluation based on clinical presentation and three-dimensional time-of-flight MRA findings and chose the combination of acquisition orientations (axial only or axial and sagittal). Black-blood HR-MRI using the spatial pre-saturation technique was performed as follows: (1) axial and sagittal proton density (repetition time (TR)/echo time (TE)=2150/12.5 ms, echo train length=10, slice thickness=2 mm, flip angle=90°, matrix=280 × 280, field-of-view=14 cm, number of excitations=2); (2) axial and sagittal T2-weighted images (TR/TE=2150/100 ms, echo train length=10, slice thickness=2 mm, flip angle=90°, matrix=280 × 280, field-of-view=14 cm, number of excitations=2); (3) sagittal T1 fluid-attenuated inversion recovery, precontrast and postcontrast (TR/TE=2100/10 ms, echo train length=6, slice thickness=2 mm, flip angle=90°, matrix=280 × 280, field-of-view=14 cm, number of excitations=2). Postcontrast images were acquired after intravenous injection of contrast agent (Dotarem (gadoterate meglumine); Guerbet, Villepinte, France; 0.1 mmol/kg of body weight).19 20
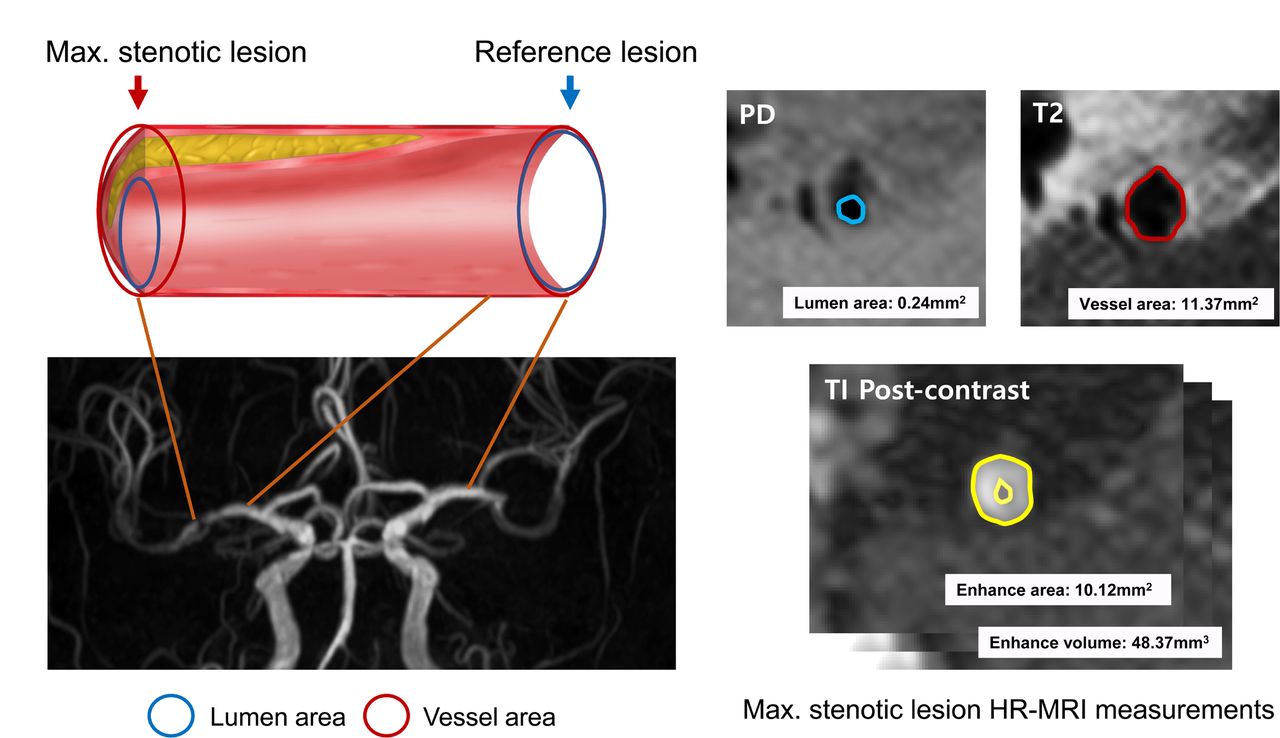
The location of cross-section measurement was selected based on the luminal image with time-of-flight MRA where maximal stenosis was located, and sagittal images for MCA and axial image for basilar artery were used for image analyses. The lumen contours were traced manually on proton density-weighted images and outer vessel contours were traced manually on T2-weighted images using the Medical Image Processing, Analysis and Visualization (MIPAV) application. The lumen area and vessel area were automatically calculated after tracing by the application. The wall area was defined as the difference between the areas of the vessel and lumen (ie, wall area=vessel area−lumen area). Normal vessels located contralateral or proximal to the stenotic portion were also assessed as reference values. The degree of stenosis was calculated as: (1−lumen area of stenotic lesion/reference lumen area)×100%. The remodelling index was defined as the ratio of the vessel area at the stenotic lesion to that of the reference vessel. We defined the wall area index as the ratio between the wall area at the stenotic lesion and that of the reference wall.
Precontrast and postcontrast T1 fluid-attenuated inversion recovery images were compared to determine the presence or absence of enhancement, the enhancement pattern (concentric vs eccentric) and the enhancement volume.21 The enhancement volume was measured semiautomatically using the MIPAV application. When multiple plaques were detected in a symptomatic intracranial artery, the plaque causing the highest degree of stenosis was considered symptomatic and selected for analysis. The volume was measured throughout the longitudinal axis of plaque. Patients were categorised into three groups based on enhancement of volume change as follows: good responder (>25% reduction), non-responder (less than +25%) and poor responder (>25% increase). Two neurologists (J-WC and M-SP) assessed the HR-MRI. A third reader (I-WY) was invited to resolve any disagreements between the two interpreters. All quantitative data were re-measured 2 weeks later by a neurologist (J-WC) to estimate intraobserver variability. The intraclass correlation coefficients for the measured HR-MRI parameters were examined for both interobserver and intraobserver agreement and the final database was locked after achieving intraclass correlation coefficients above 0.80. A figure demonstrating HR-MRI measurement methods and parameters is summarised in figure 1.

Illustration of HR-MRI measurements. HR-MRI, high-resolution MRI; Max, maximal; PD, proton density; TOF, time-of-flight; T2, T2-weighted imaging; T1, T1-weighted imaging.
Laboratory studies
Blood samples were drawn on the days (initial and 6-month follow-up) of HR-MRI examination after an overnight fast. Lipoprotein(a) concentration was measured immediately after venous blood sampling by an immunoturbidimetric method (Roche Hitachi Modular P800, Japan). The serum level of lipoprotein(a) was expressed in milligrams per decilitre. The mean intra-assay coefficients of variation for lipoprotein(a) estimation were <10% for all cases. Serum high-sensitivity C-reactive protein (hs-CRP) concentration was measured with a turbidimetric immunoassay utilising an autochemistry analyzer (Hitachi 7600–210, Hitachi, Japan) and expressed in milligrams per litre. The lower limit of detection for serum hs-CRP was 0.2 mg/L. The mean intra-assay coefficients of variation for hs-CRP measurements were <5% for all cases.
Statistical analysis
Categorical variables were summarised according to frequencies and percentages, whereas continuous variables were expressed as mean±SD. During the study period, two guidelines on cholesterol management have been published.22 23 The proportions of patients achieving target LDL-C were calculated and compared between good responder versus non-responder and poor-responder groups. We examined the differences in discrete variables pre-high and post-high-dose statin treatment using χ2 test, Fisher's Exact test or Mann-Whitney test and the differences in continuous variables using a one-way analysis of variance, Kruskal-Wallis test or t-test. Multivariable linear regression analyses were further applied to investigate the independent clinical and radiological factors associated with the changes in plaque enhancement volume and stenosis degree. Variables with p<0.20 in univariate analyses were considered explanatory variables and were evaluated in the subsequent multivariable analysis. In all analyses, values of p<0.05 were considered statistically significant. Commercially available software (STATA, V.13.1; Stata Corp, College Station, TX, USA) was used for the statistical analyses.
Results
Of the 80 patients that provided consent for enrollment in the study, 77 patients completed 6 months of high-dose statin treatment and were examined with follow-up HR-MRI. The exclusion criteria included poor compliance to high-dose statin, loss to follow-up and misdiagnosis of intracranial artery dissection as atherosclerosis. The mean age was 62.6±13.7 and 47 (61.0%) were men. The median time interval between stroke onset and initial HR-MRI evaluation was 4 (IQR: 2–6) days and the interval between the initial and follow-up HR- MRI was 179 (IQR: 163–189) days. Overall, 64 (83.1%) of patients had MCA territory infarction and 59 (76.6%) patients were treated with rosuvastatin in this study. The details of the baseline characteristics of the patients including vascular risk factors, laboratory findings and time interval for MRI are summarised in table 1.
Baseline characteristic of study participants
Six months of high-dose statin treatment significantly decreased total cholesterol, triglyceride, LDL-C and apolipoprotein B levels. A marginal decrease in D-dimer levels was also observed, which could be attributed to a normalisation of D-dimer after the acute ischaemic stroke period. In terms of statin-related adverse effects, no significant elevation was observed in liver function parameters, creatine kinase and fasting glucose levels in the study. Among HR-MRI parameters, the degree of stenosis (%, 76.47%±20.23% vs 64.05±21.29%; p<0.001) and the wall area index (7.50±4.28 vs 5.86±4.04; p=0.016) in symptomatic intracranial arteries were significantly reduced. The change in plaque enhancement volume was significantly correlated with the change in stenosis degree (coefficient, 2.62; SE, 1.22; p=0.035, figure 2A). However, the remodelling index did not show any significant change after the statin treatment (1.09±0.35 vs 1.03±0.30; p=0.195). In terms of the parameters indicating plaque activity, the proportion of patients with plaque enhancement (94.8% vs 75.3%, p<0.001) decreased and enhancement volumes of atherosclerotic plaques (mm3, 32.07±39.15 vs 17.06±34.5; p=0.013) were also reduced after high-dose statin treatment. However, the enhancement patterns did not show any significant changes. Details of the laboratory and HR-MRI findings pre-statin and post-statin treatment are summarised in table 2.
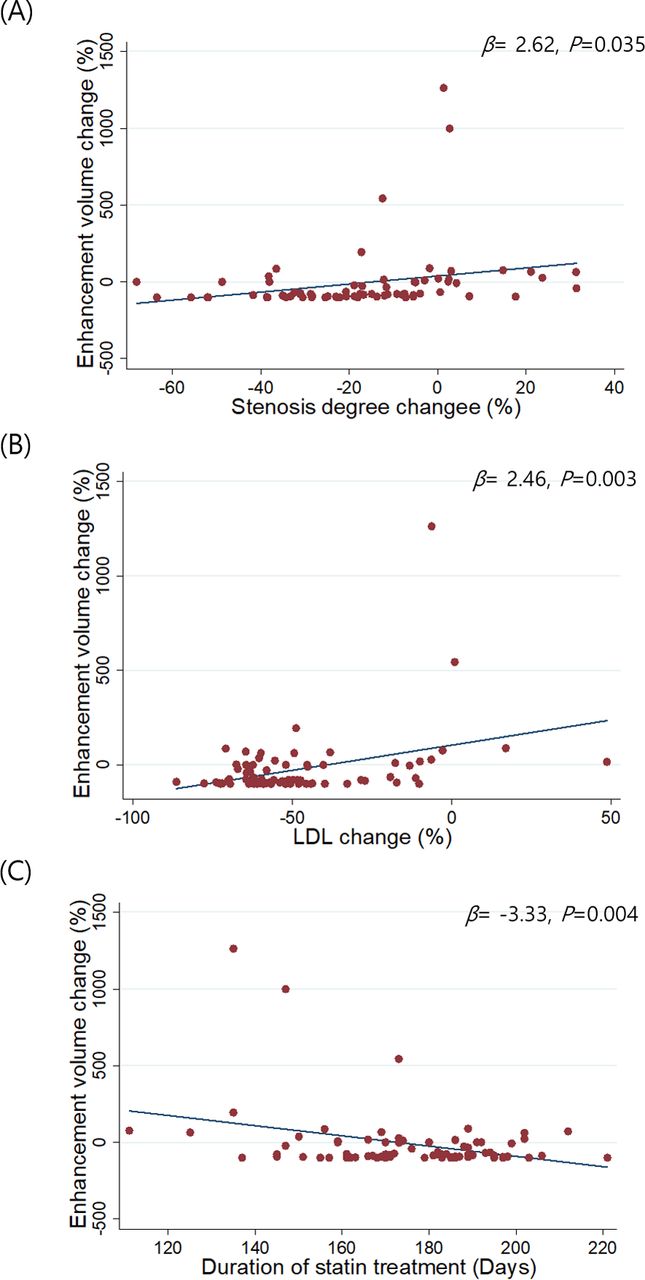
Changes in LDL-C and duration of statin treatment in stenosis degree and enhancement volume changes. LDL-C, low-density lipoprotein cholesterol.
Laboratory and HR-MRI changes
Based on these results, multiple linear regression analyses were performed to identify the independent factors associated with changes in enhancement volume after high-dose statin treatment. Among the clinical and laboratory variables, the LDL-C level change (%, coefficient, 2.24; SE, 0.78; p=0.005) and duration of statin treatment (days, coefficient, −2.38; SE, 0.92; p=0.011) were positively associated with enhancement volume (table 3 and figure 2B and C).
Univariate and multiple linear regression analyses for changes in the enhancement volume on serial HR-MRI.
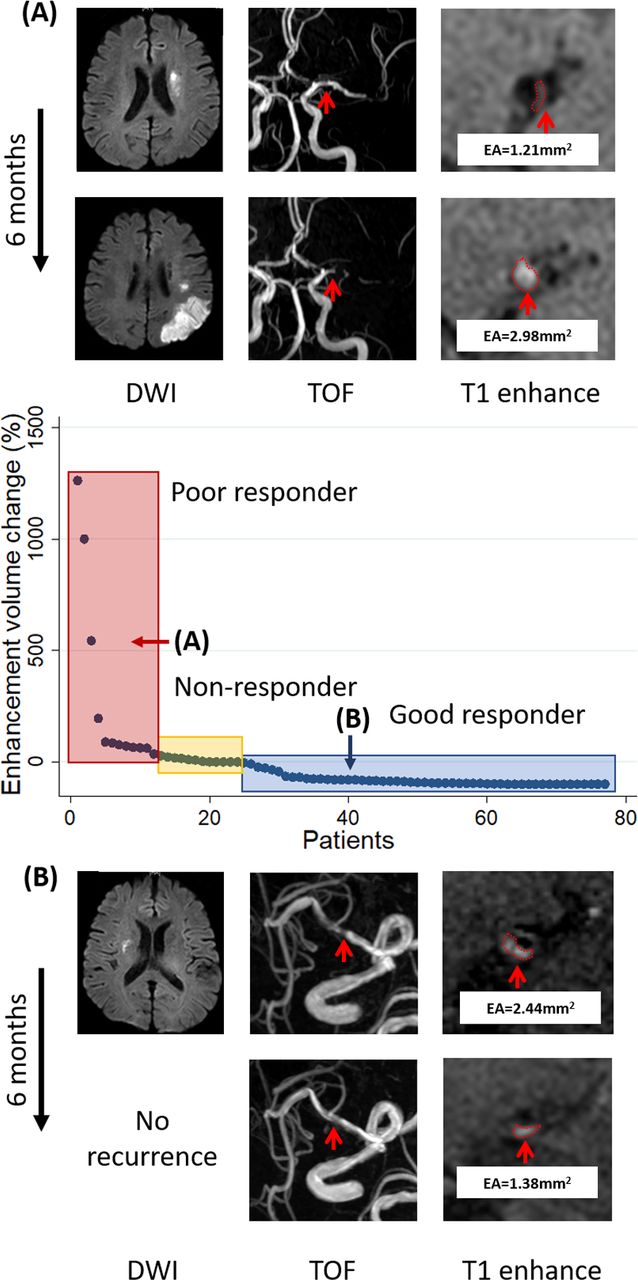
Although high-dose statin treatment was associated with regression of plaque enhancement volume, a relatively large proportion of patients showed a non-response (less than +25% change, n=14 (18.2%)) or poor response (>25% increase, n=13 (16.9%)) to the treatment. Compared with non-responders and poor responders, good responders were treated longer with high-dose statin (days, 173 (150–189) vs 183 (168–189]), p=0.034), and they showed greater reduction in LDL-C (−47.3±38.2 vs −74.8±34.1, p=0.002) and non-high-density lipoprotein cholesterol (HDL-C; −52±45.1 vs −81.3±36.3, p=0.003). When patients were categorised according to the two recent guidelines regarding management of cholesterol levels, a higher proportion of patients achieving LDL-C target reduction as defined by the 2018 guidelines (>50% reduction of LDL-C) were good responders (44.4% vs 76%) (table 4). Representative cases of good and poor responders are shown in figure 3.

{kind=link}
{kind=link}
{kind=link}
Examples of poor (A) and good (B) responders. DWI, diffusion-weighted imaging; EA, enhancement area; PD, proton density; RI, remodelling index; TOF, time-of-flight; WA, wall area.
Baseline characteristics of study subjects by high-dose statin response measured by plaque enhancement volume
In terms of clinical outcomes, 83.1% of the study population was functionally independent (mRS <2) at 3 months. There were no deaths during the study follow-up period (6 months after the stroke onset) and four patients experienced recurrent stroke after the follow-up period in the same vascular area (one in the good responder group and three in the non-poor-responder group). Safety assessments revealed two cases of myalgia that did not require discontinuation of high-dose statin. Persistent elevation of alanine or aspartate aminotransferase (>3 times the upper limit of the normal) or creatine kinase (>2 times the upper limit of the normal) was not found in this study.
Discussion
The major findings of this study are as follows. First, high-dose statin treatment effectively stabilised symptomatic intracranial atherosclerotic plaques on serial HR-MRI evaluation at 6 months. With stabilisation of plaques, stenosis degree was also improved with the use of a high-dose statin. A significant proportion of patients were statin non-responders or poor responders, that is, no significant decrease or even increase in plaque enhancement volume on the serial HR-MRI study. Achieving a>50% reduction of LDL-C levels was associated with good responders. Lastly, high-dose statin treatment during acute period of ischaemic stroke did not show significant symptomatic or laboratory-defined side effects.
The intracranial artery has been reported to have distinct characteristics compared with the extracranial carotid, coronary and systemic arteries.24–27 Unlike coronary atherosclerotic disease, stroke associated with ICAD occurs in association with various stroke mechanisms such as in situ thrombotic occlusion, artery-to-artery embolism, haemodynamic insufficiency and branch occlusive disease (BOD).28 Luminal features as well as HR-MRI characteristics of the plaque and remodelling pattern enhancement differ between BOD and non-BOD type ICAD.29 30 This study tested whether the effects of statin treatment differ between these two types of ICAD, and suggested that the effects of statin treatment are consistent despite differences in vascular and infarct pattern in patients with ICAD.
Among patients with coronary artery disease receiving statin treatment, approximately 20% of patients fail to have a significant LDL-C lowering response and experience significant progression of coronary atherosclerosis.31 In the present study, defined by changes in enhancement volume of atherosclerotic plaque, 18% were non-responders and 17% were poor responders to high-dose statin treatment. This is in line with previous reports of luminal changes with statin use.16 17 Although different definitions were used, a serial time-of-flight MRA study showed regression in 58%, stable in 38% and progression in 4% at 6 months,16 and a serial conventional angiographic follow-up study at 1 year showed regression in 49%, stable plaques in 43% and progression in 8%.17 Interpersonal variations in statin response may explain non-responder and poor-responder rates. More importantly, residual risk with statin therapy may be associated with suboptimal LDL-C levels, non-HDL-C, non-fasting remnant cholesterol, lipoprotein(a) and genetic factors related to the pleiotropic effects of statins. First, despite the use of a high-intensity statin, patients may have suboptimal LDL-C levels. In this study, non-responders and poor responders had significantly lower LDL-C reduction compared with good responders (table 4). The proprotein convertase subtilisin-kexin type 9 (PCSK9) trial showed that there was a monotonic relationship between achieved LDL-C and major cardiovascular outcomes with LDL-C concentrations of less than 0+2 mmol/L (7.72 mg/dL). The Cholesterol Treatment Trials Collaboration investigators recently showed that further lowering of LDL-C thresholds to as low as 0.5 mmol/L (21 mg/dL) was safe, even in patients with very low LDL-C levels (1.8 mmol/L, 70 mg/dL).32 All participants of the present study were followed by current guidelines for patients with symptomatic ICAD, which recommended high-intensity statin use, irrespective of cholesterol levels.33 The results of this study suggest that measurement of cholesterol levels is needed and that recent guidelines recommending to achieve a>50% reduction of LDL-C level are suitable for these patients.
Second, statins might be more beneficial or ineffective depending on laboratory findings other than LDL-C. It has been suggested that inflammatory status, as assessed by hs-CRP concentration, modifies the vascular protective effects of statin therapy, although conflicting results have been reported.34 35 After statin treatment, levels of hs-CRP were associated with coronary atheroma regression on serial intravascular ultrasound measures.36 Atherogenic dyslipidaemia, low HDL-C and high triglycerides were associated with high residual cardiovascular risk in patients with stroke or transient ischaemic attack receiving statin therapy.37 Lipoprotein(a) was a significant determinant of residual risk of cardiovascular events in patients receiving statins.38 39 The results of the present study showed that serum levels of hs-CRP and lipoprotein(a) did not change with the use of a high-intensity statins and that the baseline concentrations did not modify the vascular benefits of statin therapy.
Third, genetic variations at gene loci that affect intestinal cholesterol absorption, cholesterol production or mechanisms underlying the pleiotropic effects of statins could be an explanation for differences in individual responses.40–42 In patients with these variants, non-statin agents may be indicated. Lastly, another important factor influencing statin response is drug compliance, but in this single-arm, prospective, observational study all patients showed a compliance rate over 95%.
Strengths and limitations of this study
The strengths of this study are exclusion of non-atherosclerotic intracranial large vessel diseases such as intracranial dissection or Moyamoya disease, which are increasingly diagnosed and may be misclassified as ICAD.43 In addition, drug compliance is an important factor in statin response. In this study, all patients showed a compliance rate of over 95%. Insufficient statin treatment duration might, at least in part, explain hypo-responders to statin.
Several limitations of this study should be acknowledged. First, this was a single-centre study with small number of patients comprising only the Korean population and genetic polymorphisms have been shown to affect patient responses to statin.40 Therefore, generalisability of the study findings may be limited and needs to be validated in a larger study including a multiethnic population. Second, although this was a prospective study, there was significant variability in the time interval between initial and follow-up HR-MRIs. The variability in statin treatment duration may have also affected the proportion of non-responders and poor responders in the study. Further studies with a longer follow-up are needed because there was a monotonic relationship observed between enhancement of volume changes and the duration of statin therapy. Our ongoing long-term follow-up study of STAMINA-MRI patients, the STAMINA-MRI registry study, will provide long-term safety and outcome data regarding high-dose statin treatment for symptomatic intracranial atherosclerosis. Third, this was a single-arm study with all the patients treated with high-dose statin. Therefore, natural course of symptomatic ICAD plaque and effect of low-dose statin cannot be determined by this study. However, based on the accumulating evidence of high-dose statin treatment effect on symptomatic atherosclerotic plaque, it would be inappropriate to conduct a randomised clinical trial on the issue. Fourth, besides statin, antiplatelet, antihypertensive and hypoglycaemic drug can interfere with progression of atherosclerotic plaque. The issue needs to be addressed in a larger study. Fifth, anterior and posterior circulation vessels have different histopathological properties and vascular haemodynamic.44 45 The sample size of the study may have not been sufficient to detect differential effect of high-dose statin in the two circulations. Sixth, only two-dimensional images were acquired for image analyses in this study, since the study recruitment period was prior to wide use of three-dimensional acquisition which could have provided more precise cross-sectional vessel image with curved planar reformation. Lastly, potential factors associated with non-response or poor response were not determined in this study. Our ongoing STAMINA-MRI genetic substudy will evaluate polymorphisms associated with lipid metabolism and plaque stabilising effect of statins.
Conclusion
Our data indicate that high-dose statin treatment effectively stabilises symptomatic intracranial atherosclerotic plaques. However, a significant proportion of patients with ICAD were statin non-responders/poor responders. Further studies are needed to determine laboratory and genetic factors associated with poor statin response and alternative therapeutic options, such as PCSK9 inhibitors or combination with ezetimibe for these patients.
References
Footnotes
Presented at This study was presented at European Stroke Organization Conference 2018 as an oral presentation.
Contributors J-W Chung, the first author, established the study concept, analysed and interpreted the data, and wrote the manuscript; J Cha, MJ Lee, I-W Yu, MS Park, W-K Seo, ST Kim, SM Sung established study database and made critical revision of the manuscript; OY Bang, the corresponding author, established the study idea and database, and made critical revision of the manuscript with intellectual contents.
Funding The study was supported in part by funds from Samsung Medical Center(OTX000036) and Dong-A Pharma, Inc.(PHO112519) Seoul, South Korea.
Competing interests The statistical analysis was conducted by J-W Chung (Department of
Neurology, Samsung Medical Center, Sungkyunkwan University School of Medicine).
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.