Article Text

Abstract
Objective Amyotrophic lateral sclerosis (ALS) is a severe neurodegenerative disease and information on disease burden of ALS in mainland China was limited. We aimed to estimate the prevalence and incidence of ALS in China.
Methods We used 2012–2016 data from China’s Urban Employee Basic Medical Insurance and Urban Residence Basic Medical Insurance, covering approximately 0.43 billion individuals. ALS cases were identified by the primary diagnosis (International Classification of Diseases code or text of diagnosis) in the insurance database.
Results The crude prevalence and incidence in 2016 were 2.91 per 100 000 person-years (95% CI 2.31 to 3.58) and 1.65 (95% CI 1.33 to 2.01), respectively. The standardised prevalence and incidence based on 2010 Chinese census data were 2.97 (95% CI 2.91 to 3.03) and 1.62 (95% CI 1.58 to 1.67), respectively. The annual prevalence between 2013 and 2016 remained relatively constant, ranging from 2.91 (95% CI 2.31 to 3.58) in 2016 to 3.29 (95% CI 2.51 to 4.17) in 2014 (linear regression: β=−0.129, p=0.104). Both rates peaked in the group aged 75–79 years.
Conclusions The prevalence and incidence of ALS in mainland China were lower than those in developed countries, and maintained a relatively stable trend. The age at onset and age at diagnosis for ALS patients were younger than those in developed countries. Further research is expected to clarify the potential pathophysiological mechanism of ALS.
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) is a fatal neurodegenerative disease, which may result in progressive weakness of the limbs, muscle atrophy, pyramidal signs, dysarthria, dysphasia and dyspnoea.1 2 More than 73% of patients with ALS will die of respiratory failure.2 3 The severe disability associated with the disease and the consequently high fatality rate not only affect the disability-adjusted life years and quality of life of patients, but also impose a heavy burden on patients’ families and on society.4 5 Some information on epidemiology and disease burden of ALS has been collected, but that from low-income and middle-income countries has been limited.2
It has been reported that developed countries have much higher rates of ALS incidence and prevalence than low-income and middle-income countries.2 Previous studies also indicated that Asians show a relatively lower incidence than Caucasians.2 The prevalence was 2.25–9.9 per 100 000 people and the incidence was 0.69–2.2 per 100 000 person-years in Japan, while the numbers were 3.4 per 100 000 people and 2 per 100 000 person-years in South Korea, respectively.1 6 7 However, epidemiological studies of ALS statistics are limited and inconsistent in China. Population-based studies from Hong Kong or Taiwan reported a prevalence ranging from 0.95 to 3 per 100 000 people, and the incidence ranging from 0.3 to 0.5 per 100 000 person-years.1 5 8 9 Both rates, especially the incidence rate, were much lower in Hong Kong and Taiwan than in Japan and South Korea.1 2 For mainland China, only two hospital-based studies have been performed.10 11 These existing studies were limited to only a single city, or calculated the rates with a rough capture–recapture method, or used inconsistent definitions of ALS.10 11 In addition, no further epidemiological studies are available to estimate the rates among different sexes, age groups and geographical regions in mainland China, which is of importance to inform policy making with respect to ALS management in China.
This study was conducted to provide recent estimates of the prevalence and incidence of ALS in mainland China and to investigate their patterns across sexes, age groups and geographical regions, using a nationally representative sample from 2012 to 2016.
Materials and methods
National medical insurance database
The medical insurance database we used included the Urban Employee Basic Medical Insurance (UEBMI) for working and retired employees in cities (ie, employers and employees from government agencies and institutions, state-owned enterprises, private businesses, social organisations and other private entities), and the Urban Residence Basic Medical Insurance (URBMI) for urban citizens without employment (ie, children, students, elderly people and unemployed residents).12 In 2016, the UEBMI and URBMI covered more than 95% of the entire urban population. The UEBMI and URBMI are updated on a monthly basis in all cities. The database contains information about insured individuals’ sociodemographic characteristics (nationality, household registration, birth date, etc), medical treatment records (disease names, diagnostic codes, etc) and medical expenses. This study is registered with the Chinese Clinical Trial Registry (ChiCTR), number ChiCTR1800018217.
Study population
We performed a retrospective population-based study using the UEBMI and URBMI data from 21 provinces covering 1 January 2012 to 31 December 2016. We excluded the population under 18 years old. Ten provinces (Fujian, Tibet, Tianjin, Beijing, Shanghai, Sichuan, Ningxia, Hebei, Qinghai and Xinjiang) were excluded for the following reasons: no information on the International Classification of Diseases (ICD) code or diagnostic text; reporting policy exemptions; only one insurance type covered; or absence or abnormality of crucial information (eg, primary diagnosis).
All claim records were deidentified to protect patients’ privacy.
Case identification
Hospital admissions for each health condition were identified based on the diagnostic text or ICD code. Natural language processing was applied to standardise the diagnostic text or code.
All potential patients with ALS were selected using ICD-10 (G12.2), medical terms in Chinese and English, and English abbreviations including motor neuron disease, ALS, progressive muscular atrophy, primary lateral sclerosis, progressive bulbar palsy, flail arm syndrome and flail leg syndrome.
The diagnostic text of each potential patient with ALS was then reviewed by two neurologists independently to identify actual patients with ALS. Neurologists in China made the diagnosis of ALS based on the revised EI Escorial Criteria during study period. If the diagnostic text contained words such as ‘undetermined’, ‘uncertainty’, ‘?’ and other synonyms, the patients were categorised as a subgroup named ‘patients with uncertainty of ALS’, which was used for the sensitivity analysis.
Statistical analysis
We calculated the national prevalence for each of the 4 years from 2013 to 2016. To minimise the impacts of prevalent ALS cases, we estimated the national incidence for 2016 only by setting up a 3-year wash-out period. Prevalence and incidence were also estimated by sex, age and geographical region (East, North, Northeast, Northwest, Southcentral and Southwest). Since ALS is an incurable disease, a patient was considered to always be suffering from ALS after the first diagnosis of ALS.
Both the prevalence and incidence were calculated using a two-stage approach. We calculated the prevalence and incidence in each province in the first stage. In the second stage, the national or regional average estimates were calculated by combining the estimates for each province using a random effects meta-analysis.
In the first stage, the method for estimating the prevalence and incidence in each province was as follows: the denominator (N) used to calculate the annual prevalence and incidence of ALS was the total person-years in each province in both the UEBMI and URBMI during a certain year. The numerator (M) was the number of patients with ALS estimated from the denominator population in each province, taking into account missing diagnostic information. Specifically, the total number of enrolled individuals in each province was divided into three groups: subjects with no claim records (N1), subjects with complete diagnostic information in their claim records (N2), and subjects with claim records but with missing diagnostic information (N3).
The prevalent (M1) or incident (M2) patients with ALS that we actually observed were from N2. However, realistically, a certain number of prevalent (M3) or incident (M4) patients with ALS existed in N3. To determine the real prevalence and incidence, we adopted a strategy based on Poisson regression to estimate M3 and M4. A detailed description of the strategy can be found in the online supplementary file. In the second stage, the national or regional average estimates were calculated by pooling the estimates from each province using a random effects meta-analysis. In this stage, we stabilised the variance of province-specific estimates using the Freeman-Tukey double arcsine transformation.13
One province (Gansu) was excluded from the estimation of incidence because the timespan of the data was less than 4 years. The unit for both the prevalence and incidence was per 100 000 person-years. The 95% CIs of both rates were calculated based on the Poisson distribution. We calculated the age-adjusted rates based on the 2010 Chinese national census data, the Revised European Standard Population 2013, the 2010 US population and the 2011 Australian population. Sensitivity analyses were conducted to assess the robustness of the results: (1) including all uncertain ALS cases, (2) including only observed cases to assess the lower bounds of the rates and (3) excluding the top 10% of provinces with missing diagnostic information. Student’s t-test for continuous variables and the X2 test for categorical variables were used to compare male and female patients. All statistical analyses were conducted with Stata V.15.0, and we considered a two-sided p<0.05 as statistically significant.
Results
The total number of individuals covered by the UEBMI and URBMI in this study was approximately 0.43 billion (table 1 and online supplementary etable 1). A total of 7 134 patients with ALS were identified, and the male to female ratio was 1.70:1. The mean age of male patients was 54.99 (SD=12.87) years, and that of female patients was 53.34 (SD=13.55) years (table 2). The mean age at diagnosis of all incident cases in 2016 was 56.83 (SD=13.48) years old; by sex, it was 54.90 (SD=13.71) for females and 58.03 (SD=13.21) for males. The comparison of the basic characteristics between the excluded provinces and included provinces can be seen in the online supplementary etable 2.
Supplemental material
Characteristics of the population of 21 provinces in urban China during 2012–2016
Characteristic of patients with amyotrophic lateral sclerosis in 21 provinces in urban China during 2012–2016
Prevalence
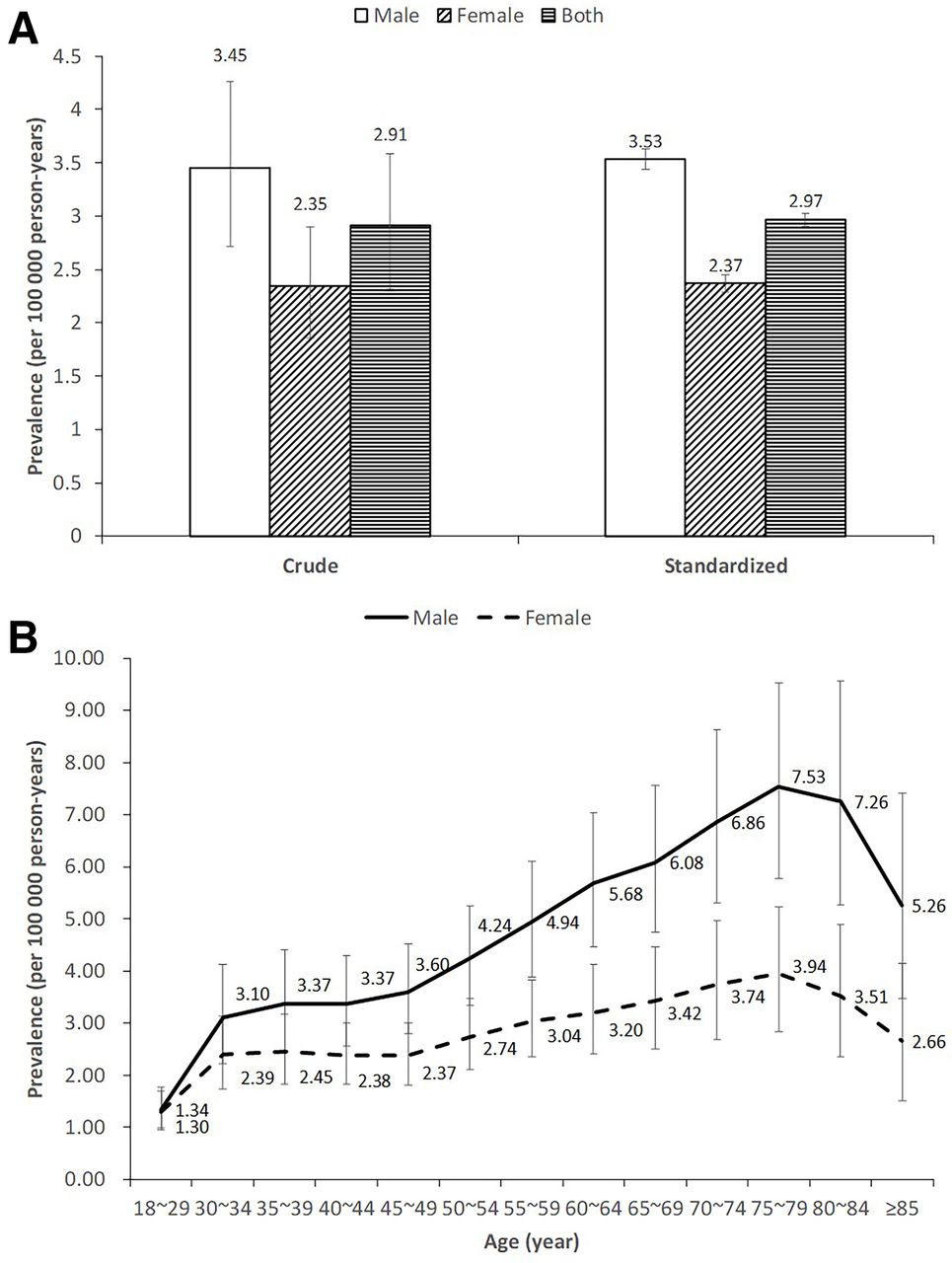
The national ALS prevalence in 2016 was 2.91 per 100 000 person-years (95% CI 2.31 to 3.58), with a higher prevalence in males than females (figure 1 and online supplementary efigure 1). The trends of prevalence with age in males and females were similar: the prevalence showed an increasing trend before peaking at 75–79 years old, followed by a drop after age 80 (figure 1). The highest prevalence appeared in the population aged 75–79: 7.53 (95% CI 5.76 to 9.53) in males and 3.94 (95% CI 2.83 to 5.23) in females (online supplementary etable 3). The prevalence in East China was the highest (5.31, 95% CI 4.27 to 6.47), followed by Southcentral China (2.84, 95% CI 1.76 to 4.18), with North China showing the lowest prevalence (1.80, 95% CI 1.54 to 2.09) (online supplementary etables 4–6). We performed a linear regression to analyse the trend in the annual prevalence between 2013 and 2016 and found that there was no statistically significant temporal trend (coef: −0.129, p=0.104). The annual prevalence during the 4 years ranged from 2.91 (2.31 to 3.58) in 2016 to 3.29 (2.51 to 4.17) in 2014.

Prevalence of amyotrophic lateral sclerosis in urban China in 2016 (the standardised prevalence is based on 2010 Chinese census data).
Incidence
The annual ALS incidence in 2016 was 1.65 per 100 000 person-years (95% CI 1.33 to 2.01) (figure 2 and online supplementary efigure 1). The incidence in males was 1.90 (95% CI 1.52 to 2.33), which was higher than that in their female counterparts (1.38, 95% CI 1.09 to 1.70) (figure 2). Similar to the trend in prevalence with age, the incidence in males reached its highest point of 3.50 (95% CI 2.79 to 4.29) in the 75–79 age group, and that in females peaked at 1.82 (95% CI 1.30 to 2.43) in the 75–79 age group (online supplementary etable 7). East China had the highest incidence (2.29, 95% CI 2.21 to 2.38) and Southcentral China ranked second (1.93; 95% CI 1.83 to 2.03). The lowest incidence was 0.57 (95% CI 0.39 to 0.79) in Northwest China (online supplementary etables 4-6).

{kind=link}
{kind=link}
Incidence of amyotrophic lateral sclerosis in urban China in 2016 (the standardised prevalence is based on 2010 Chinese census data).
Standardised rates
The standardised national prevalence based on 2010 Chinese census data was 2.97 per 100 000 person-years (95% CI 2.91 to 3.03), with 3.53 (95% CI 3.44 to 3.63) for males and 2.37 (95% CI 2.29 to 2.45) for females. Regarding the standardised incidence based on 2010 Chinese census data, the national incidence was 1.62 (95% CI 1.58 to 1.67), with the male incidence and female incidence being 1.81 (95% CI 1.74 to 1.88) and 1.23 (95% CI 1.17 to 1.29), respectively. Both rates increased slightly after standardisation based on the USA, European and Australian populations (table 3).
Standardised prevalence and incidence of amyotrophic lateral sclerosis in urban China in 2016 (units: /100 000 person-years)
Sensitivity analysis
By considering only observed cases (which was considered as underestimation), we obtained the lower bounds of the national prevalence and incidence: 2.17 per 100 000 person-years (95% CI 1.74 to 2.65) and 1.38 (95% CI 1.13 to 1.66), respectively. The results calculated by including all uncertain ALS cases or excluding the top 10% of provinces with missing diagnostic information were similar to the main results reported above (online supplementary etable 8).
Discussion
In this national study, we elucidated three primary findings. First, in 2016, the estimated age-adjusted ALS prevalence in mainland China was 2.97 per 100 000 person-years, and the incidence was 1.62 per 100 000 person-years. These estimates indicate that Chinese prevalence and incidence rates are significantly lower than those in North American, European and Asia-Pacific countries, such as New Zealand and Australia.1 2 The influence of age group was confirmed by the increase in the prevalence and incidence rates in China after the standardisation of our data to either the European, USA or Australian population.14 However, the incidence and prevalence were still lower than in the corresponding regions even after the standardisation to either the European, USA or Australian population.2 15 16
It should be noted that some studies including ours have been based on claims data while studies such as Logroscino et al 16 used registry design.2 15 We must acknowledge that each data source has its own advantages and limitations: registry studies are effective for case ascertainment but less feasible for studying rare conditions due to the difficulty of ensuring a large population. Alternatively, claims data can ensure a large sample for studies on rare diseases, but may be less accurate in terms of case identification.17 Although differences in data sources may influence the results,16–18 our study and previous studies have suggested that other factors play important roles in the onset and survival of ALS.2 15 16 19–21 The larger ageing population in developed countries may result in an increase in incidence, while better medical care and less pollution may contribute to a better prognosis and may partially explain the higher prevalence.8 22 Furthermore, the development of multidisciplinary clinics provided better medical care for the patients with ALS and improved the survival in recent years.23 In addition, the unique genetic background of Chinese population might also contribute to the lower incidence and prevalence in China.24–26 Zaldivar et al 26 reported a very interesting phenomenon, namely, the mortality rate was lowest in the population with mixed ancestry in Cuba, which was attributed to the admixture of genes in this population. Similarly, China is a multiethnic country, and marriages between different ethnic groups might also result in gene admixture in the Chinese population, with a potential protective effect against ALS.
Our results were similar to those in South Korea, and overlapped with the reported figures in Japan.1 2 27 This finding indicates that the incidence and prevalence are similar across countries in East Asia, and are independent of the Sociodemographic Index (SDI), consistent with the meta-analysis of the Global Burden of Disease Study 2016.2 The prevalence of ALS in our study was comparable with the findings from Hong Kong and Taiwan, but the incidence seemed to be higher than in these two regions and than that reported in two studies in mainland China.5 8 10 11 Our large national sample size and standardised rate calculation methodology ensured relatively stable and new results10 11 28; these results indicated that the actual number of incident patients with ALS in Asia was still higher than that in Western populations given the large population. In addition, men were more likely to have ALS than females, with a 1.4-fold increased risk, a finding consistent with previous studies in Asian and other races.1 7 29–31
The prevalence of ALS in mainland China presented a relatively stable trend during the study period. This finding was in accordance with results from Taiwan, Iceland and Norway but not consistent with the increase in prevalence in Italy and Germany.5 32–35 The relatively short period of our study might limit the possibility of detecting a significant trend; however, the stable prevalence and large number of patients with ALS should not be ignored from the perspective of disease prevention and treatment. In addition, the prevalence and incidence in East China were significantly higher than those in other regions. This phenomenon remained after age standardisation. There are substantial differences in genetic background, culture, socioeconomic levels, climate and geographical features of the residential area, lifestyle and dietary pattern among different regions in China. It has been reported that factors including economic level, medical condition, air pollutant and environmental toxin exposure can affect the prevalence and incidence of ALS.8 20 21 East China generally has higher economic level, more tertiary hospitals and more industry associated with higher environmental pollution than other regions.36 However, reasons for the geographical variation are difficult to determine from the claims data. Further investigation is required to confirm and find the causes.
Second, the age at diagnosis and the estimated age at onset were both younger in China than in other countries.1 5 8 9 29 30 37–39 In our study, the mean age at diagnosis was 56.34 years old. It is reasonable to estimate the age at onset by using the interval between age at onset and age at diagnosis, that is, the diagnostic delay, according to previous research. Previous studies reported that a mean diagnostic delay time ranging from 14.0 to 14.8 months.11 40 Correspondingly, the estimated age at onset was approximately 55 years old. The age at diagnosis in our study was similar to that reported in Taiwan,5 while the age at onset was younger than that in Japan, South Korea, Australia and New Zealand as well as Hong Kong in China, and only older than that in India.1 8 9 29 30 37–39 There are several possible explanations for the younger age at diagnosis and age at onset in China. First, the lower percentage of bulbar-onset ALS in China may result in an earlier age at onset and then an earlier age at diagnosis, because the age at onset of this phenotype is much higher than that of limb-onset ALS.40 Second, the shorter life expectancy and different age distributions in low-income and middle-income countries such as China and India may partly explain the earlier onset and diagnosis.14 40 41 Third, factors such as malnutrition may also play a role in the younger age at onset in low-income and middle-income countries,39 and the even earlier age at onset of patients in India confirms this explanation.39 Indeed, in the context of economic development and population ageing in low-income and middle-income countries such as China, the age at onset of ALS in China has already increased compared with our previous data.40
We used a large, nationally representative sample of the Chinese urban population, ensuring the estimation of both the prevalence and incidence of a rare disease. We were able to provide overall estimations of both rates and to explore age and sex patterns in these rates, as well regional differences.
This research has several limitations. First, the lack of detailed information, such as clinical characteristics and laboratory results, in the Chinese claims data precluded the possibility to stratify the diagnosis in greater detail. Second, the new ALS cases for the estimation of the incidence were defined based on a 3-year disease-free period before the index claim, which may not be sufficient. Consequently, the prevalence and incidence are close in our study, which may not lead to the short survival of ALS patients in China, especially given additional consideration that both incidence and survival of ALS are age dependent. This is consistent with a Korean study27 where the estimated incidence and prevalence rate were 1.20 and 3.43 per 100 000, respectively, but the estimated mean survival time was 50.0 months. Third, diverse missing proportions of diagnostic related variables may have affected the estimates. However, several sensitivity analyses were conducted to explore the potential influence on the estimations. In particular, the lower bounds of the rates were presented using only observed cases of ALS which could facilitate the interpretation of the findings. In addition, data from 10 provinces were excluded from our analysis due to the missing crucial information to identify ALS cases. We compared basic characteristics between the excluded provinces and included provinces. We found similar age and sex distribution, but higher gross domestic product and proportion of Chinese Han population in the included provinces. Finally, rural inhabitants are not included in the UEBMI and URBMI. Certain urban populations, such as college students and military soldiers, were not included in the study because they have different types of medical insurance. The exclusion of these groups could have affected the estimates.
In conclusion, this research is the first population-based study to investigate the prevalence and incidence of patients with ALS in mainland China. The prevalence and incidence of ALS were lower in mainland China than in developed countries. The age at diagnosis and age at onset were both younger than those in developed countries, but the sex ratio was comparable. As a country with a population of 1.3 billion, China can provide helpful and important information regarding healthcare services and disease prevention for patients with ALS worldwide.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
LX, LC and SW are joint first authors.
SZ, PG and DF contributed equally.
Contributors Conception: SZ and DF. Design: SW, LX, PG and SZ. Administrative support: SW and SZ. Provision of study material or patients: JW. Collection and assembly of data: JW, GL, LX, JF and LL. Data analysis and interpretation: LX, SW, DF, PG and SZ. Manuscript writing: LX, LC and SW. Final approval of manuscript: all authors.
Funding This study was funded by the National Natural Science Foundation (grant numbers 91646107, 91846112, 91546120, 81701248 and 81873784).
Disclaimer The authors alone are responsible for the content and writing of the paper.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the ethical review committee of the Peking University Health Science Center (IRB. No: IRB00001052-18012).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are available from National Healthcare Security Administration of China but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors on reasonable request and with permission of National Healthcare Security Administration of China.