Article Text

Abstract
Objective We aimed to investigate the role of pretreatment collateral status in predicting the efficacy and safety of endovascular treatment (EVT) in acute ischaemic stroke due to cervical and/or cerebral arterial occlusions.
Methods Relevant full-text articles published since 1 January 2000, investigating correlations between collateral status and any efficacy or safety outcome in patients undergoing EVT in cohort or case–control studies, or randomised clinical trials, were retrieved by PubMed and manual search. Two authors extracted data from eligible studies and assessed study quality. Risk ratios (RR) were pooled for good versus poor collaterals for outcomes based on a random-effects model. Sensitivity and subgroup analyses were conducted.
Results In total, 35 (3542 participants) and 23 (2652 participants) studies were included in qualitative review and quantitative meta-analysis, respectively. Overall, good pretreatment collaterals increased the rate of favourable functional outcome at 3 months (RR=1.98, 95% CI 1.64 to 2.38; p<0.001), and reduced the risks of periprocedural symptomatic intracranial haemorrhage (RR=0.59, 95% CI 0.43 to 0.81; p=0.001) and 3-month mortality (RR=0.49, 95% CI 0.38 to 0.63; p<0.001), as compared with poor collaterals, in patients with acute ischaemic stroke under EVT. No individual study could alter the estimate of overall effect of collateral status, but there were moderate to significant heterogeneities between subgroups of studies with different modes of EVT, different arterial occlusions and different collateral grading methods.
Conclusions Good pretreatment collateral status is associated with higher rates of favourable functional outcome, and lower rates of symptomatic intracranial haemorrhage and mortality, in patients with acute ischaemic stroke receiving endovascular therapies.
Statistics from Altmetric.com
Introduction
During the past decade, numerous clinical trials have been investigating the effects of endovascular treatment (EVT), with or without prior intravenous thrombolysis, in treating acute ischaemic stroke attributed to intracranial or extracranial large artery occlusions. In early 2013, the results of three major randomised clinical trials (RCTs) comparing EVT versus standard treatment for intravenous thrombolysis in acute ischaemic stroke were published but failed to establish the superiority of EVT over intravenous thrombolysis in determining the 90-day function outcomes of patients enrolled. These trials included Interventional Management of Stroke (IMS) III, SYNTHESIS Expansion: A randomized Controlled Trial on Intra-Arterial Versus Intravenous Thrombolysis in Acute Ischemic Stroke, and Mechanical Retrieval and Recanalization of Stroke Clots Using Embolectomy (MR RESCUE), in which trials a large portion of the patients randomised in the EVT arms were treated with intra-arterial thrombolytic therapy and/or first-generation mechanical clot disruption devices (such as the Merci Retriever and the Penumbra System).1 Evidence from another two contemporary RCTs indicated that newer-generation stentrievers might lead to better angiographic and clinical outcomes in treating patients with acute ischaemic stroke than the first-generation retrieving devices, with the comparisons of Solitaire Flow Restoration Device versus Merci Retriever in the Solitaire With the Intention For Thrombectomy (SWIFT) trial and Trevo versus Merci retrievers in the Thrombectomy REvascularization of Large Vessel Occlusions in Acute ischemic Stroke (TREVO 2) trial.2 ,3 Further, a series of most recently completed RCTs have proved EVT to be more effective than usual medical care with or without intravenous thrombolysis, which, in contrast with the three previous trials, used stentrievers in a majority of the patients randomised in the EVT arm. Such trials include the Multicenter randomized Clinical Trial of Endovascular Treatment for Acute ischemic Stroke in the Netherlands (MR CLEAN),4 the Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times (ESCAPE) trial,5 the Extending the Time for Thrombolysis in Emergency Neurological Deficits–Intra-Arterial (EXTEND-IA) trial,6 the Solitaire With the Intention For Thrombectomy as PRIMary Endovascular Treatment (SWIFT PRIME) trial,7 and the Endovascular Revascularization With Solitaire Device Versus Best Medical Therapy in Anterior Circulation Stroke Within 8 Hours (REVASCAT) trial.8 The results of these trials are encouraging and patients may benefit from more advanced mechanical thrombus retrieving devices.1 ,4
However, with patients with heterogeneous stroke recruited under relatively simple selection criteria in most of the trials, the application of different EVT methods might not be the only factor to explain the different outcomes of individual patients in each trial, or the differences in overall outcomes among these trials. Other patient-specific characteristics, such as the collateral status, have been found to be diversely distributed in patients receiving EVT, and have been repeatedly noted to be independently associated with angiographic and clinical outcomes of such patients.2 ,9 For instance, post hoc analysis of the IMS-III trial showed diverse collateral profiles in patients treated by EVT, among whom those with a more robust collateral circulation had significantly better recanalisation, reperfusion and functional outcomes.9 Moreover, post hoc analysis of the SWIFT trial showed similar collateral spectrum and significant predictive values of collateral grades for a favourable functional outcome at 90 days throughout the trial (adjusted OR 4.63, 95% CI 2.03 to 10.54; p<0.001), as well as in each arm of the trial (Solitaire arm and Merci arm).2
To further verify the impact of collateral status on the efficacy and safety of EVT in acute ischaemic stroke, we carried out the current systematic review and meta-analysis to comprehensively review and synthesise the currently available relevant evidence. We hypothesised that good pretreatment collaterals might be associated with a higher rate of favourable functional outcome at 3 months and lower rates of periprocedural symptomatic intracranial haemorrhage (sICH) and 3-month mortality, in patients with acute ischaemic stroke treated with intra-arterial thrombolysis and/or mechanical clot disruption, with or without prior intravenous thrombolysis.
Methods
The systematic review and meta-analysis was carried out and reported according to the Meta-analysis Of Observational Studies in Epidemiology (MOOSE)10 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)11 statements, with the review protocol as detailed below.
The primary efficacy outcome was favourable functional outcome, defined as modified Rankin Scale (mRS) of 0–2, at 3 months. The safety outcomes included: (1) sICH reported within 1–7 days after EVT, confirmed by imaging exams and clinical manifestations, and defined in accordance with the definitions used in individual primary studies and (2) mortality at 3 months.
Search strategy
We searched PubMed on 5 March 2015 for potentially eligible studies, with full text articles published in English since 1 January 2000. Briefly, the search terms included ‘stroke’, ‘collateral*’, ‘endovascular*’, ‘thromboly*’, ‘intra-arterial*’, ‘mechanical*’ and ‘thrombectomy’. The detailed search strategy is presented in online supplementary table S1. In addition, we also performed a manual search of references from pertinent reviews and original articles.
Study selection
The titles and abstracts of all records by PubMed and manual search were reviewed and screened by one author (XL), to exclude irrelevant items. The full text of the remaining items was carefully reviewed by the same author to select eligible primary studies for inclusion in qualitative and/or quantitative analyses. A final decision was made by consulting with another author (HF), especially for publications that were in doubt.
Any study meeting the following criteria was included in the current systematic review: (1) cohort or case–control study, or RCT in humans, with some or all of the patients reported in the study undergoing EVT (including intra-arterial thrombolysis, mechanical clot disruption and retrieval, and angioplasty with or without stenting), with or without prior intravenous thrombolysis; (2) patients were treated by EVT within the hyperacute phase of acute ischaemic stroke, while the exact time windows might differ among studies, which was up to 24 h at most; (3) the sample size of patients receiving EVT was ≥10 and (4) the study reported the correlations between pretreatment collateral status and efficacy and/or safety outcomes in patients under endovascular treatment. For articles based on RCTs, the treatment arms could be different modes of EVT, or EVT versus intravenous therapy or placebo. In addition, when more than one article from the same centre, or based on the same study, with obviously overlapping patients involved, simultaneously met the aforementioned inclusion criteria, only that article with the largest sample size of patients undergoing EVT was included by consensus of two authors (XL and HF). Case reports, case series with less than 10 patients or conference abstracts were excluded. Among all the primary studies included in the systematic review, only those reporting correlations between pretreatment collateral status and at least one of the three efficacy and safety outcomes as defined above were included in the quantitative meta-analysis.
Data extraction and quality assessment
For all studies included in the systematic review, data extraction and study quality assessment were independently conducted by two authors (XL and HF), with disagreement resolved by consensus. The following data were extracted from each primary study, if available, using a predefined standardised form: author, year of publication, countries or regions, number of study centres, sample size of patients receiving endovascular treatment to be analysed in the current study, patients’ characteristics, time window for patient selection for endovascular treatment, occlusive arteries involved, mode of EVT, imaging modality and methods to grade collateral status, and the correlations between dichotomised collateral status and the three efficacy and safety outcomes as defined above. Study quality was evaluated by the Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses, with a score of ≥6 or <6, respectively, being considered as Quality A or B.
Data synthesis and analysis
Data synthesis and analysis were performed using the Cochrane Review Manager (V.5.2). Two-sided p values of <0.05 were considered statistically significant in tests for the estimated effect of collateral status on individual outcomes, while p values of <0.10 were used in heterogeneity tests. The overall effects of good collateral versus poor collateral on the three individual outcomes investigated were estimated based on data from the included primary studies, and presented as risk ratios (RR) and 95% CI based on the DerSimonian and Laird random-effects model. Between-study and/or between-subgroup heterogeneities were analysed by Cochrane's Q (χ2) and I2 statistics. Potential publication bias of primary studies with various sample sizes was evaluated by the funnel plot.
Sensitivity analysis was conducted for the primary efficacy outcome (favourable functional outcome, mRS 0–2, at 3 months) by using the jackknife resampling method, which was omitting one study each time to detect the influence of individual studies on the estimate of the overall effect. Moreover, exploratory subgroup analyses were performed for the primary efficacy outcome to reveal differences between subgroups divided by different predominant ethnicities, mean age, percentages of male patients, baseline median National Institutes of Health Stroke Scale (NIHSS), modes of EVT reported in the primary studies (intra-arterial thrombolysis only, mechanical therapies only or intra-arterial thrombolysis plus mechanical therapies), imaging methods to grade collateral status, anterior or posterior circulation stroke, and intracranial or extracranial arterial occlusions.
Results
Study selection and description
Study screening procedures are illustrated in online supplementary figure S1. For potentially eligible studies published in English between 1 January 2000 and 5 March 2015, 289 records were identified. Then 192 records were excluded by reviewing the titles and abstracts, and another 62 records were excluded by reviewing the full text for reasons as listed in online supplementary figure S1. Thus, there were 35 primary studies, with 3542 participants in total, included in the systematic review, while 23 of them (2652 participants) reporting correlations between pretreatment collateral status and the three specific outcomes as aforementioned were included in the meta-analysis.
Detailed characteristics of the 35 studies are shown in online supplementary table S2. Among the 35 primary studies, three were post hoc analyses of one or both arms of RCTs,2 ,9 ,12 and the others retrospectively reported data from prospectively registered single-arm clinical trials or other cohort studies. The quality of three studies was graded as <6 of the NOS, due to the inadequate follow-up and low comparability of the cohorts. The included studies were carried out in different countries or regions: 11 studies (1434 participants) in Europe,13–23 10 (707 participants) in Asia,24–33 8 (435 participants) in North America12 ,34–40 and 1 (87 participants) in Australia,41 and the remaining 5 were cross-continental studies (879 participants).2 ,9 ,42–44 Concerning the mode of endovascular treatment, 8 studies (454 participants) reported correlations between collateral status and efficacy and/or safety outcomes in patients receiving intra-arterial thrombolysis;12 ,13 ,22 ,24 ,25 ,34 ,39 ,40 also, there were four studies (421 participants) in patients receiving mechanical therapies, including mechanical clot disruption with or without urgent angioplasty/stenting,2 ,20 ,30 ,44 while other studies reported such data in cohorts with various modes of EVT.
Various methods were used in the included studies to grade pretreatment collateral flow by using different imaging modalities. For the collateral grades being correlated with outcomes, 12 studies used the American Society of Intervention and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) collateral flow grading system45 by digital subtraction angiography (DSA),2 ,9 ,17 ,18 ,27 ,31 ,32 ,37 ,38 ,42–44 mostly defining ASITN/SIR collateral grades of 3–4 and 0–2 as good and poor collaterals, respectively; 11 studies used other grading methods by DSA;12 ,14–16 ,22 ,25 ,26 ,33–35 ,39 9 studies used different grading methods on CT angiography (CTA);13 ,19 ,20 ,23 ,28 ,30 ,36 ,40 ,41 and the other studies used CT perfusion or combined grading methods with different imaging modalities.21 ,24 ,29
Primary efficacy outcome
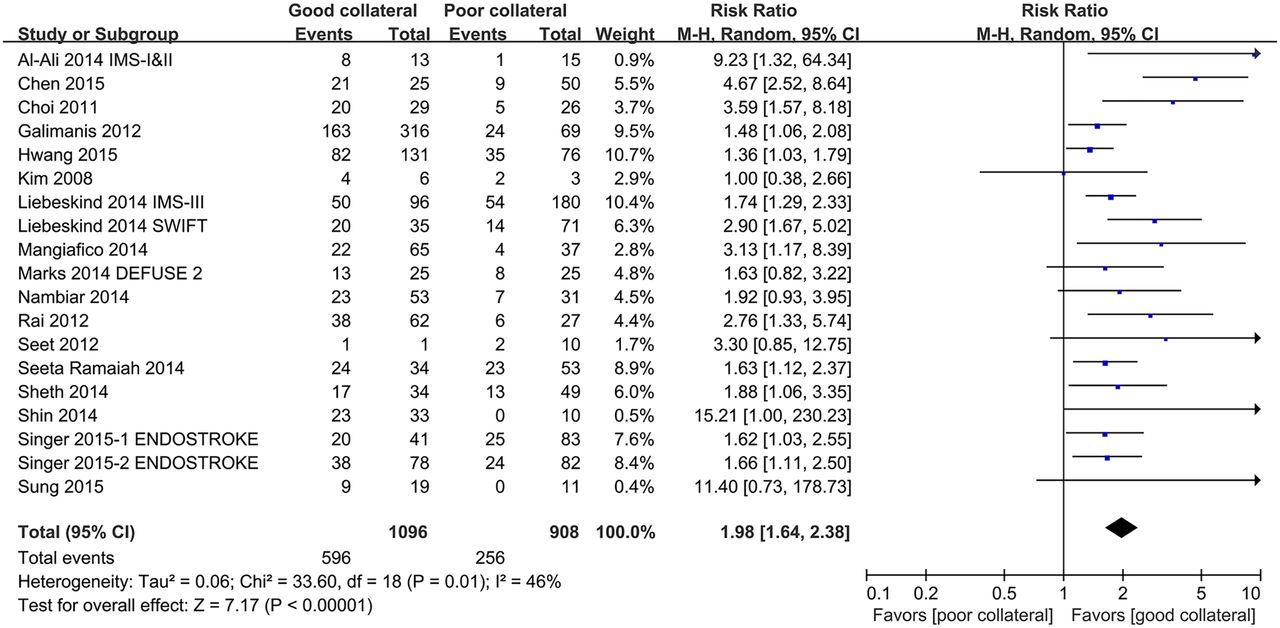
Overall, 19 studies with 2004 participants were analysed for the primary efficacy outcome of favourable functional outcome (mRS 0–2) at 3 months. Visual inspection of the funnel plot did not identify significant publication bias. In these studies, 1096 and 908 patients were regarded as having good or poor collaterals in total, and the rates of favourable functional outcome were reported to range from 25% to around 60% in individual studies. Pooled analysis of the 19 studies showed that the presence of good pretreatment collateral status nearly doubled the rate of favourable functional outcome at 3 months in patients receiving endovascular treatment, with or without prior intravenous thrombolysis, as compared with poor collateral circulation (RR=1.98, 95% CI 1.64 to 2.38; p<0.001; figure 1). However, there was moderate between-study heterogeneity (Cochrane's Q=33.60, p=0.01; I2=46%). In the jackknife resampling procedure for sensitivity analysis, none of the individual studies showed a significant influence on estimates of the overall effect size (figure 2).

Forest plot showing individual and overall risk ratios of good versus poor pretreatment collateral status for favourable functional outcome (modified Rankin Scale 0–2) at 3 months, in patients with acute ischaemic stroke receiving endovascular treatment, with or without prior intravenous thrombolysis.

Sensitivity analysis for favourable functional outcome at 3 months by jackknife resampling procedures.
The results of subgroup analyses are shown in table 1. The estimates of effect size significantly differed between subgroups with different modes of EVT investigated in the primary studies (Cochrane's Q for between-subgroup heterogeneity=18.00, p<0.001; I2=88.9%). The RRs of good versus poor collateral status were, respectively, 4.45 (95% CI 2.76 to 7.18) and 3.23 (95% CI 1.46 to 7.16) in studies specifically reporting correlations between collateral status and 3-month favourable functional outcome in patients receiving intra-arterial thrombolysis or mechanical therapies (with or without angioplasty and stenting), and 1.64 (95% CI 1.44 to 1.86) in the 14 studies with different EVT modes among participants, or hybrid endovascular therapies in individual participants. There was also significant heterogeneity between subgroups of studies reporting such correlations in patients treated by EVT for arterial occlusions of different cervicocerebral arteries (Cochrane's Q for between-subgroup heterogeneity=2.66, p=0.10; I2=62.4%). In particular, there existed significant heterogeneity among studies using different imaging methods to grade collateral flow (Cochrane's Q for between-subgroup heterogeneity=11.14, p=0.01; I2=73.1%), while there was no significant between-study heterogeneity within the subgroup of studies using the ASITN/SIR collateral flow grading system on DSA to correlate with the 3-month favourable functional outcome (RR=1.68, 95% CI 1.44 to 1.96; Cochrane's Q for between-study heterogeneity=7.22, p=0.41; I2=3%). There was no significant between-subgroup heterogeneity in subgroup analyses by other factors as listed in table 1.
Subgroup analyses for the primary efficacy outcome of modified Rankin Scale 0–2 at 3 months
Safety outcomes
There were, respectively, 11 (1686 participants) and 10 (1049 participants) studies analysed for the safety outcomes of sICH reported within 1–7 days after EVT, and mortality at 3 months. No significant between-study heterogeneity was detected for these two outcomes, and no significant publication bias was revealed by funnel plots.
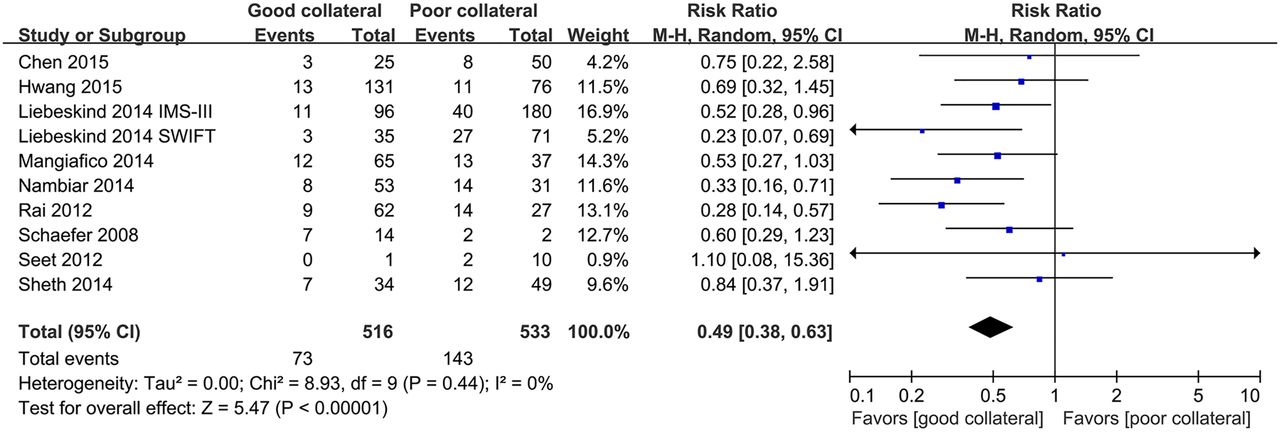
In most of the included studies, sICH was defined as intracranial haemorrhage confirmed by imaging examinations performed immediately after EVT treatment, within 1 day, or at 7 days, accompanied by an increase of at least four points in the NIHSS score at the time of the imaging examination. Throughout the 11 studies analysed, sICH occurred in 5% to 27% of participants in different studies with different time points to define sICH. Overall, the presence of good pretreatment collateral dramatically reduced the risk of sICH within 1–7 days after EVT by around 40% (RR=0.59, 95% CI 0.43 to 0.81; p=0.001; figure 3). Mortality at 3 months was reported to be around 20% in nine of the studies included in the analysis, while it was reported to be 56% in one small study. The presence of good collateral status almost halved the risk of death at 3 months (RR=0.49, 95% CI 0.38 to 0.63; p<0.001; figure 4).

Forest plot showing individual and overall risk ratios of good versus poor pretreatment collateral status for symptomatic intracerebral haemorrhage reported within 1–7 days after endovascular treatment for acute ischaemic stroke.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing individual and overall risk ratios of good versus poor pretreatment collateral status for mortality at 3 months, in patients with acute ischaemic stroke receiving endovascular treatment.
Discussion
In this systematic review and meta-analysis, we reviewed and synthesised relevant evidence in the recent 15 years, regarding the influence of pretreatment collateral status on the efficacy and safety of EVT in acute ischaemic stroke with cervical and/or cerebral arterial occlusions. We demonstrated that good collaterals prior to EVT could significantly enhance the rate of favourable functional outcome at 3 months in such clinical scenarios and, in the meantime, dramatically reduce the risk of periprocedural symptomatic intracranial haemorrhage and 3-month mortality.
Among the studies included in quantitative analysis, diverse endovascular therapies were involved, such as intra-arterial thrombolysis with urokinase or a recombinant tissue plasminogen activator, emergent angioplasty and stenting, mechanical employment of a coil thrombus retriever, an aspiration device or a stentriever, and intravenous intra-arterial bridging therapies. Significant heterogeneity was revealed between subgroups of studies with different modes of EVT. Moreover, patients’ characteristics also differed among included studies in ethnicities, age, sex, stroke severity and locations of cerebral ischaemia and arterial occlusion. The pooled estimates of the effect of collaterals on the primary efficacy outcome in each of the subgroups, as well as in the sensitivity analysis, consistently favoured good pretreatment collaterals for a higher rate of 3-month favourable functional outcome. More robust collateral flow compensation to brain areas with restricted blood flow due to acute blockage of cervicocerebral arteries may lead to a favourable penumbral pattern, enhance the rates of recanalisation and reperfusion, mitigate reperfusion injury and result in a smaller final infarct size,2 ,46 ,47 which could partly explain the identical trend of the favourable effects of good collaterals on clinical outcomes throughout studies with diverse characteristics.
Traditional clinical trials in treatment of acute ischaemic stroke commonly used demographics and clinical features as primary inclusion criteria to recruit patients, while recently attention has been paid to pathophysiological and imaging information of potentially eligible patients. For instance, the MR RESCUE trial,48 as mentioned above, and several newly completed trials, published in 2015,5–8 adopted collateral grades, penumbral patterns or infarct core assessment in enrolment criteria. Such a shift in the paradigm of patient enrolment in EVT trials is encouraging, especially with the positive findings in adjunctive EVT plus best medical care versus best medical care alone, in improving functional outcomes of acute anterior circulation in patients with ischaemic stroke in recent trials. For instance, the inclusion criterion of a small infarct core and prospectively defined moderate-to-good collateral circulation in ESCAPE,5 and evidence of salvageable tissue on perfusion imaging in EXTEND-IA,6 or the exclusion criterion of evidence of a moderate/large infarct core in the SWIFT PRIME and REVASCAT trials.7 ,8 As the significance of collateral circulation in determining the tissue fate and clinical outcomes is being increasingly noticed and addressed in the treatment of acute ischaemic stroke, the current evidence, however, has been almost exclusively built on retrospective studies or post hoc analyses of prospective studies. Hence, vigorous prospective observational studies are needed to verify the ultimate prognostic values of individual collateral status in outcomes of patients undergoing EVT, to further consolidate the basis for launching RCTs using collateral assessment as an important criterion for patient recruitment. A further step could be randomised clinical trials with a two-way factorial design, to test if the collateral status could alter the favourable treatment effects of EVT over other treatment methods as demonstrated in most recently published trials.
Another significant issue was revealed in this systematic review and meta-analysis, which had in fact been raised before,45 ,47 which was the heterogeneity in collateral grading methods. Heterogeneous collateral grading methods employed in the included studies might have interfered in the synthesis of their results, as indicated in the relevant subgroup analysis. However, studies using the ASITN/SIR collateral grading system by DSA showed homogeneous effects of collateral circulation on the 3-month functional outcome, which was consistent with the recommendation to use this method for collateral flow grading on DSA, by the Cerebral Angiographic Revascularization Grading (CARG) collaborators, Stroke Imaging Repository (STIR) Revascularization working group, and STIR Thrombolysis in Cerebral Infarction (TICI) task force.47 With rapid advances in non-invasive imaging for collateral assessment, for instance, time-resolved CTA,19 more studies in a prospective manner validating the reproducibility of such grading methods, as well as their reliability in correlating with outcomes of endovascular treatment, are warranted, and consensus on using non-invasive imaging to grade collaterals is imperative. Such efforts could help lay the foundation for horizontal and longitudinal comparisons of relevant study findings in the future.
One important limitation of the current review was the diversity of included studies in certain aspects as mentioned above, and the retrospective nature of most of the studies. Second, some of the included studies primarily investigated the correlations between collaterals and outcomes among patients treated by endovascular or intravenous therapies, while only the participants undergoing EVT therapies were analysed in this systematic review and meta-analysis. Third, all subgroup analyses were exploratory, and we did not perform meta-regression to detect the potential influence of covariates due to the relatively small number of studies included in quantitative analysis; therefore, interpretation of the results of subgroup analyses should be cautious, and more studies are needed to further verify the factors found in this study to lead to heterogeneous effects of collaterals on outcomes of patients undergoing EVT. In addition, only full-text articles published in English were included, and only one author reviewed and screened titles and abstracts of all records retrieved, though another author was consulted for items in doubt, which may be subtly biased in study inclusion in the current systematic review.
In summary, the current systematic review and meta-analysis demonstrated that good pretreatment collaterals improve the 3-month functional outcome, and reduce the risks of periprocedural symptomatic intracranial haemorrhage and 3-month mortality, in patients with acute ischaemic stroke under endovascular treatment for cervicocerebral arterial occlusions. Baseline assessment of collateral flow could be considered as part of the pretreatment workup of EVT patients as a way of providing prognostic information. Our findings, however, do not indicate that patients with poor collateral flow should not receive endovascular treatment. At the present stage, vigorous prospective studies on collateral grading, especially using non-invasive imaging, and its role in determining tissue fate and clinical outcomes in patients receiving endovascular treatment are still in great need.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figure
- Data supplement 2 - Online table S1
- Data supplement 3 - Online table S2
Footnotes
Contributors XL, LL, KSW and DSL designed and initiated the study. XL performed the literature search. XL and HF screened eligible studies, extracted data and assessed the study quality. XL and CM carried out statistical analyses. All authors interpreted the data. XL and DSL drafted the manuscript. TL, CM, ZM, LL and KSW critically revised the manuscript.
Funding This work was partly supported by the Chinese University of Hong Kong (Focused Investment Scheme B) and the Institute of Innovative Medicine, Chinese University of Hong Kong, Hong Kong.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.