Article Text

Abstract
Objective To report the clinical features, causes and outcome of cerebral cortical border-zone infarcts BZI (C-BZI).
Methods The authors prospectively included patients with MRI-confirmed C-BZI among individuals consecutively admitted in Stroke Unit.
Results Forty-five patients presented C-BZI out of 589 with MRI-confirmed cerebral infarcts (7.6%). Particular clinical characteristics existed in C-BZI in comparison with other cerebral infarctions as a whole, including: (1) frequent transient symptoms at onset (27% vs 9%; p<0.001) and low severity score (NIHSS=3.1±3.0 vs 5.2±6.1; p=0.02); (2) early seizures in first 2 weeks (7/45 (15.6%) vs 12/544 (2.2%); p<0.001), even when focusing only on other infarctions involving the cerebral cortex (15.6% vs 4.3%; p<0.01); (3) heterogeneous clinical presentation but specific transcortical aphasia allowing a clinical suspicion of BZI before MRI; and (4) frequently associated internal carotid disease (69%), with subsequent early surgery in 75% of the cases. Following adapted care in stroke unit, C-BZIs' prognosis appeared good (Rankin score ≤2 at D90) for 82% of the patients.
Conclusion Some clinical features are overrepresented in such infarctions, including initial transient symptoms preceding the onset of a completed deficit, transcortical aphasia and early seizures. Despite lower initial severity, C-BZIs justify early management in stroke unit, often followed by carotid surgery, leading to an overall good prognosis.
- Watershed infarct
- border-zone
- transient ischaemic attack
- endarterectomy
- early seizures
- transcortical mixt aphasia
- carotid stenosis
- prognosis
- aphasia
- cerebrovascular disease
- movement disorders
- dysphagia
- metabolic disease
- stroke
- multiple sclerosis
- cardiology
- amyloid
- neuropathy
- peripheral neuropathology
- paraproteinaemia
Statistics from Altmetric.com
- Watershed infarct
- border-zone
- transient ischaemic attack
- endarterectomy
- early seizures
- transcortical mixt aphasia
- carotid stenosis
- prognosis
- aphasia
- cerebrovascular disease
- movement disorders
- dysphagia
- metabolic disease
- stroke
- multiple sclerosis
- cardiology
- amyloid
- neuropathy
- peripheral neuropathology
- paraproteinaemia
Introduction
The concept of border-zone infarcts (BZI) was first discussed in the 19th century.1 Following the 1940s and 1950s, Zulch and Behrend reported the typical topographical areas of BZI and hypothesised their haemodynamic mechanism.2 BZIs are frequent, accounting for about 10% of all brain infarcts.3 They are defined by their topography involving an area localised at the junctions between two adjacent but non-anastomosing arterial territories. Two distinct supratentorial watershed areas have been described: superficial and deep. ‘Superficial’ or ‘cortical’ BZIs are located between the cortical territories of middle cerebral artery (MCA) and either anterior cerebral artery or posterior cerebral artery. ‘Deep’ or internal BZIs are located between the MCA deep and superficial arterial systems.4–6 More recently, two distinct etiopathological mechanisms for BZIs, haemodynamic and micro-embolic, have been proposed in relation to their location, more likely haemodynamic for deep BZIs and embolic for cortical BZIs.7–10 However, differentiating haemodynamic and micro-embolic mechanisms in the setting of large-artery stenosis is notoriously difficult. Future studies combining brain imaging of local perfusion, diffusion-weighted MRI and cerebrovascular reactivity mapping using fMRI, and ultrasound detection of microembolic signals might help to resolve these issues.7 ,10–12
Previous studies describing BZIs were essentially retrospective, mostly based on CT imaging and/or mainly focused on pathophysiological studies with little clinical description.5 ,6 ,8 ,13–21 The objective of our study was to describe the clinical features, causes and outcome of the C-BZIs, based on systematic MRI in consecutive ischaemic stroke patients prospectively recruited in our stroke unit. Part of the study includes retrospective analysis of prospectively collected data.
Material and methods
The present study is based on 589 consecutive patients with MRI-confirmed brain infarcts out of 1220 admissions for stroke or suspicion of transient ischaemic attack in our stroke unit between June 2007 and February 2010. Initial diagnostic studies systematically included routine laboratory work-up, ECG and cerebral MRI within 24 h after admission. MRI protocol included axial T1-weighted, FLAIR, diffusion-weighted imaging (MR-DWI), gradient-echo sequences, intracranial time-of-flight (TOF) and cervical vessels magnetic resonance angiographies (MRA). All 1220 consecutive individuals have been investigated by cerebral MRI, except 17 (because of pacemaker, heart valves, aneurysm clip, metallic foreign body or severe claustrophobia (MRI in 98.6%). Among our cohort, 857 patients presented various acute cerebrovascular diseases, including 589 MRI-confirmed cerebral arterial infarctions. The other 268 patients suffered from various other acute cerebrovascular diseases (mostly transient ischaemic attacks, intracerebral haemorrhages or cerebral vein thrombosis). The remaining patients presented stroke mimics (mostly seizures/postictal paresis, hypoglycemias, complicated migraines, conversion disorders and various myelopathies or brain tumours (n=363; not shown). Baseline characteristics, cardiovascular risk factors and NIHSS score22 of the 589 patients with MRI-confirmed acute cerebral infarction on MR-DWI are indicated in table 1. Based on the results of diagnostic studies, causes were classified according to TOAST classification.24 Cerebral infarctions were also classified according to vascular territories determined by MR-DWI.
General data of our 589 consecutive patients with MRI confirmed infarcts according to their locations
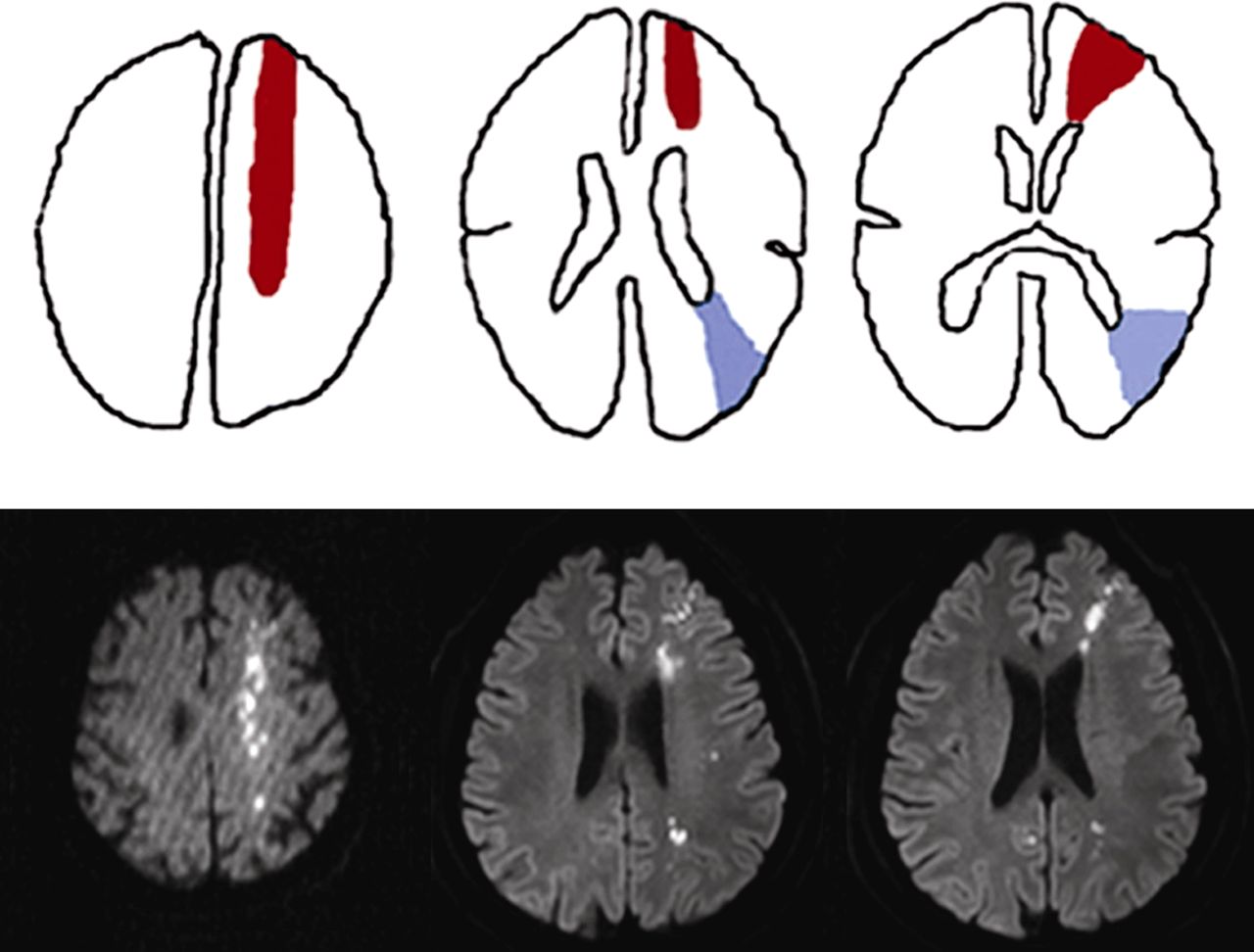
Cortical BZIs were defined on MRI using the classical criteria (figure 1). MRI analysis was performed by two of the authors (GS and RS) experienced in neuroimaging of stroke patients, and blinded to patient information. We reviewed the MR-DWI data retrospectively, and selected images that matched the hemispheric cortical border-zone areas according to the commonly used templates.4 ,5 When opinions were conflicting, MRI data were discussed together with a third neuroradiologist (DD), and consensus was reached between all three observers. Two types of superficial C-BZIs were considered in this study: anterior C-BZIs, that is, between the superficial territories of MCA and anterior cerebral artery and posterior C-BZIs, between the superficial territories of MCA and posterior cerebral artery. Exclusively, deep internal BZIs, defined as white-matter infarction between the MCA deep and superficial arterial systems were excluded because of the difficulty in differentiating them from lacunar infarcts due to small-vessel diseases (perforating arteries infarcts). We included them in the deep hemispheric infarcts (see tables 1 and 2).

{kind=link}
Examples of cortical border-zone infarcts (C-BZIs) upper panel: schematic representation of border-zone territories. Superficial (cortical) anterior and posterior BZIs are represented in red and blue, respectively, according to classical criteria (Damasio et al., 1983; Bogousslavsky et al., 1986).4 ,5 Lower panel: examples of superficial anterior and posterior BZI on diffusion-weighted MRI, based on classical cartographies, shown in upper panel.
Demographics and clinical data in patients with MRI confirmed—hemispheric cortical BZI compared with other cerebral infarctions
Etiologic investigations in patients with cerebral ischaemic events systematically included cervical and trans-cranial Doppler, echocardiography and ECG monitoring at least during 48 h. Language and swallowing disturbances were assessed within the first 48 h following admission. Language was assessed with LAST scale.25 Additional investigations were performed when necessary (complementary biological tests, lumbar puncture, transoesophageal echocardiography, and more rarely cerebral angiogram). Carotid stenosis was evaluated by systematic combination of MR-angiography and duplex echography using ECST method. If results were not concurring, CT angiography was also carried out (using NASCET method). Patients' demographic characteristics including age, gender, hypertension, diabetes mellitus, dyslipemia, current tobacco smoking, initial stroke severity based on NIHSS, involved vascular territories and causes of stroke were prospectively entered in our database (tables 1 and 2).
On the top of the above-mentioned prospectively collected data, we retrospectively reviewed for this study: (1) for all patients with MRI-assessed cerebral infarctions, the occurrence of previous transient ischaemic attacks (TIAs) within 2 weeks of stroke onset, and the occurrence of early seizures, defined as happening within the first 14 days following stroke onset, and (2) for patients with C-BZIs, initial clinical features and outcome based on Rankin score at 3 months.26
Patients with C-BZIs were compared with patients with other cerebral infarctions using Fisher's exact tests for categorical variables, and Student's t test to compare averages.
Results
Cohort characteristics
Among the 589 consecutive patients with MRI-confirmed cerebral infarctions, 45 had hemispheric C-BZIs (7.6%) (tables 1 and 2). C-BZIs were anterior in 22 patients, posterior in five, and both anterior and posterior in 18. They were bilateral in five. Age, gender, hypertension history, diabetes mellitus, hypercholesterolaemia and current tobacco consumption did not significantly differ between patients with and without C-BZIs. NIHSS scores at admission were significantly lower in the C-BZI group (3.1±3.0 vs 5.2±6.1; p=0.02) (table 2).
Clinical features
Transient symptoms before the infarct occurred more frequently in patients with C-BZIs (27%) than in others (9%) (p<0.001). A fluctuating course with waxing and waning deficits occurred in 3 C-BZI patients. Clinical signs of C-BZIs were various, as indicated in table 3. A particular pattern of language disorder was observed. Aphasia was present in 13 C-BZI patients among the 21 left-sided C-BZIs, all right-handed patients. It was initially always a transcortical mixed aphasia with expressive disturbances (naming difficulties including paraphasias), altered lexical and syntaxic comprehension, while repetition was preserved. Aphasia evolved towards a transcortical motor aphasia (reduced speech with short sentences, paraphasia, preserved comprehension and repetition) in left anterior C-BZIs, and towards a transcortical sensory aphasia (altered lexical and syntactic comprehension, preserved naming and repetition) in left posterior C-BZIs. Aphasia rapidly improved with a full recovery at day 10 in 77% of patients. Other symptoms included hemiparesis (29%), brachiofacial weakness (27%), dysarthria (18%), ataxia (18%), hemianopsia (9%), quadranopsia (4.4%), headache (4.4%), confusion (4.4%), isolated arm or leg weakness (4.4% and 2.2%), pseudo-radial weakness (2.2%), optic ataxia (2.2%), dysexecutive syndrome (2.2%) (table 3). Patients with bilateral C-BZIs did not present peculiar symptoms, and were not more severe (mean initial NIHSS: 2.8±2.7).
Clinical signs of cortical border-zone infarctions (BZI)
Early seizures
Early seizures were more frequent in C-BZIs (15.6%) than in other infarcts (2.2%; p value<0.001), even when only focusing on other infarcts involving the cerebral cortex (12/282; 4.3%; p value<0.01). In C-BZIs, seizures occurred at stroke onset in three patients, and during the following 2 weeks in four.
Causes
Causes of C-BZI are indicated in table 4. The most frequent was ipsilateral internal carotid artery (ICA) disease, present in 31 patients (69%), that is, atheromatous ICA bulb stenosis in 22 patients, occlusion in five and siphon stenosis in four patients. Carotid stenosis was ≥60% in 21 patients, including 12 over ≥80%. One C-BZI with carotid occlusion revealed giant-cell arteritis. Three patients had MCA stenosis (7%). Four patients had cardiac diseases (11%; heart failure with atrial fibrillation in one, isolated atrial fibrillation in one, and ischaemic cardiomyopathy with ejection fraction <40% in two). Three patients had several associated causes indicated in table 4, and no cause was found for four patients. Concerning the five patients with bilateral C-BZIs, causes were ICA stenosis (n=2) or occlusion (n=1), cardioembolic disease (n=1) and no cause was identified in one patient.
Causes of cortical borderzone infarcts (C-BZI)
Treatment
No patients with C-BZI could receive IV rtpA fibrinolysis because of contraindications (such as late arrival or oral anticoagulation on vitamin K antagonist treatment). Following admission, all C-BZI patients were monitored during the last 48 h in our acute stroke unit with bed rest until cervical and trans-cranial Doppler or MRA provided information about extra- and intracranial arterial status. They received usual treatments such as aspirin and statins. Eighteen of the 22 patients with proximal ICA stenosis underwent endarterectomy, which was performed within the first 6 days in 13. Two out of the three patients with MCA stenosis had angioplasty with intracranial stenting.
Outcome
Rankin score at 3 months was ≤1 in 35 patients (78%). In others, Rankin scores were 2, 3, 4 or 5 for 2, 3, 4 and one patients at D90, respectively. Mean Rankin score was 1.0±1.4. There was no mortality at third month. Concerning our five patients with bilateral C-BZIs, their mean Rankin score at D90 was 1.4±1.9 (NS).
Discussion
Cortical BZIs were found in 7.6% of our consecutively recruited patients with MRI-confirmed infarcts, consistent with the approximately 10% observed in previous clinical and autopsy studies.3 ,5 ,6 ,8 ,15 Demographic characteristics and cardiovascular risk factors in C-BZI patients were not different from those previously reported.5 ,6 ,8 ,15 Compared with other infarcts as a whole, C-BZIs had a lower mean NIHS score (3.1±3.0) and a higher frequency of transient symptoms before onset or at onset (27%), also in accordance with previous reports.5 ,6 ,8
Previous clinical data reported lower limb weakness and frontal syndrome associated with either transcortical motor aphasia in left anterior C-BZI, or dyscalculia in right anterior C-BZI, while brachiofacial weakness, quadranopsia and hypoesthesia were reported in posterior C-BZIs, associated with Gerstmann syndrome in the left ones.15 Our results are more heterogeneous with symptoms mimicking MCA infarction in roughly one-fourth of our patients. Dysphasia was frequent and had a distinct clinical and outcome pattern, with initial transcortical mixed aphasia, evolving according to location to transcortical motor or sensitive aphasia, of excellent long-term prognosis, confirming ours and the data of others.23 ,27 Our five patients with bilateral C-BZIs differ from previously reported cases by the absence of pseudo-bulbar or pseudo-brainstem syndromes, syncopes, limb shaking or cortical blindness.5 ,6 ,15 ,19 Lastly, this larger series confirms our observation that early seizures are significantly more frequent in C-BZIs than in other infarcts with cortical involvement.28
C-BZIs were mostly associated with ipsilateral internal carotid disease (69%), in accordance with previous series (from 58% to 84%).5 ,6 ,15 ,17 ,29–32 Among the 24% of patients without arterial ICA or MCA stenosis, there were often several intricate causes leading to haemodynamic compromise, such as bradycardia, atrial fibrillation, hypotension, dehydration, anaemia or heart failure pointing to the importance of monitoring blood pressure and cardiac function, and of maintaining sufficient brain perfusion. Following adapted care in stroke unit, C-BZIs' prognosis appear to be excellent with a mean Rankin score at third month around 1 in our series and in a previous study of 75 C-BZI patients.8
Our study has several strengths, including systematic MRI for all individuals admitted in our stroke unit. Our study has several limitations. Although we identified C-BZI using MR-DW imaging, the exact location of cerebral infarcts was sometimes difficult to determine, because of the inter-individual variability of vascular arterial territories.33 Our use of two blinded MRI reviewers likely reduced such difficulties. Bias from the recruitment has also to be discussed. Although our study is based on consecutive patients entering an acute stroke unit, our patients had less severe underlying arterial conditions than some previous C-BZI series, in particular, with only 16% with intracranial stenosis (n=3 MCA and n=4 siphon stenosis) compared with 28% of C-BZI patients in Asian series.8 Similarly, only five patients (11%) had ipsilateral ICA occlusion which has a poorer short-term prognosis associated with in-hospital death, neurological worsening and a bad functional outcome.34
In summary, our study emphasises distinct HC-BZI features including: (1) frequency of transient symptoms at onset and of early seizures in first 2 weeks after stroke; (2) heterogeneity of clinical presentation, but with a specific transcortical type of aphasia; (3) good prognosis with low initial severity score and good outcome, and (4) frequency of ipsilateral internal carotid stenosis.
Acknowledgments
We thank Professor M-G. Bousser for helpful discussions and critical review of this manuscript.
References
Footnotes
Competing interests None.
Ethics approval Local ethical committee.
Provenance and peer review Not commissioned; externally peer reviewed.