Article Text

Abstract
After occlusion of flow in an artery, further ischaemic episodes are not expected due to lack of a flow conduit to carry the embolus. In the carotid stump syndrome, ongoing ischaemic events may continue due to collateral flow via the external carotid artery. We report two patients presenting with posterior circulation strokes after documented vertebral artery occlusion, due to a vertebral stump syndrome. Their presentation, the pathophysiology of cervico-vertebral anastomoses and management are described.
Statistics from Altmetric.com
The role of the carotid artery stump as an embolic source for cerebral ischaemia has been well described.1–3 When there is occlusion of flow in an artery, further ischaemic episodes are not expected1 due to lack of a flow conduit to carry the embolus. However, in the carotid stump syndrome, ongoing ischaemic events may continue despite an occluded artery. Collateral flow via the external carotid artery branches can carry proximal or distal emboli to the intracranial internal carotid artery.
To our knowledge, there have been no reports of a parallel syndrome causing stroke in the posterior circulation after vertebral artery occlusion. We report two patients who presented with posterior circulation strokes after documented vertebral artery occlusion. We describe their histories, the anatomy of the cervical-vertebral anastomotic collaterals as a pathway for ongoing ischaemia, and implications for management.
CASE 1
A 66-year-old man had transient right hemianopsia and vertical diplopia. He was placed on aspirin, but returned 6 months later with another similar episode. Magnetic resonance angiography revealed occlusion of the left vertebral artery at its origin. He was anticoagulated with therapeutic INR . Two weeks later, he had four similar transient ischaemic attacks followed by loss of the right visual field. Examination revealed a right superior homonymous quadranopsia, left heel-to-shin ataxia and wide-based gait. Magnetic resonance imaging at this time revealed acute ischaemia in the left calcarine cortex and left cerebellar hemisphere, and occlusion of the left vertebral artery at the subclavian origin.
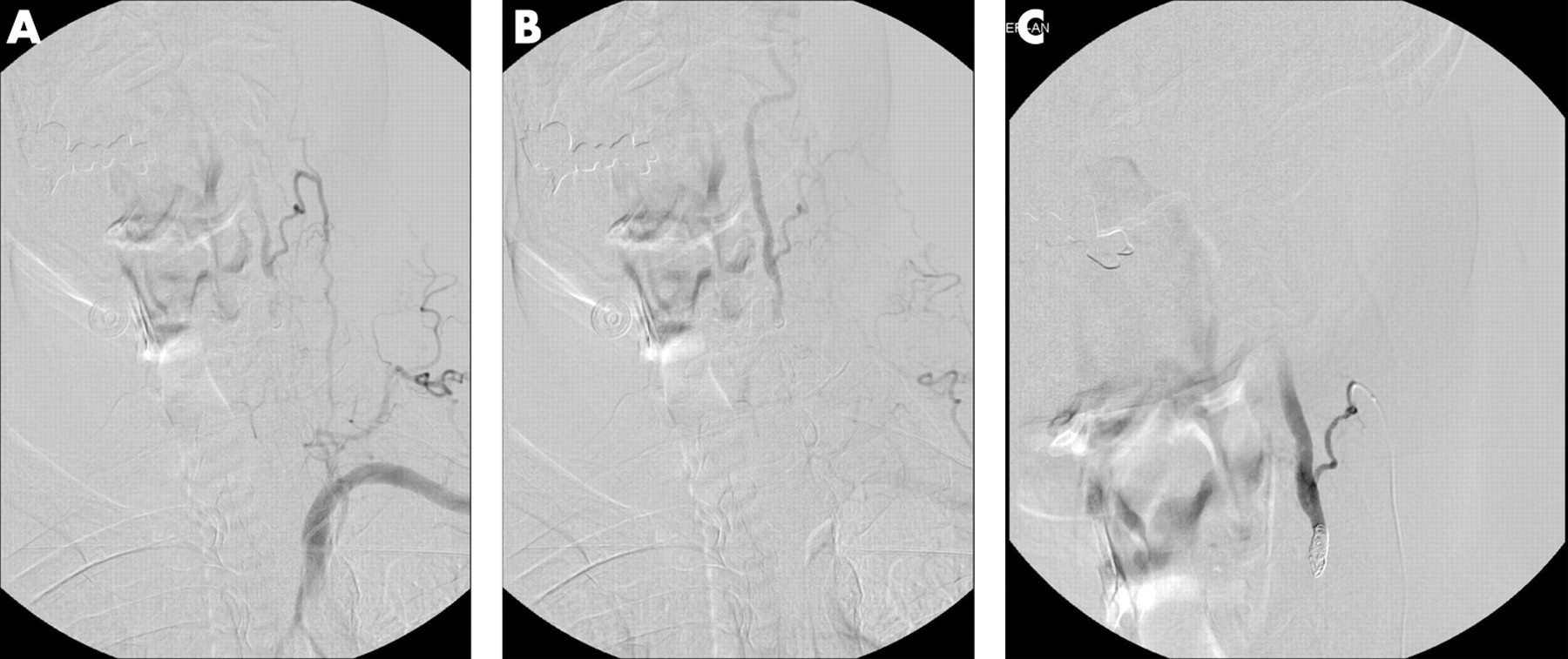
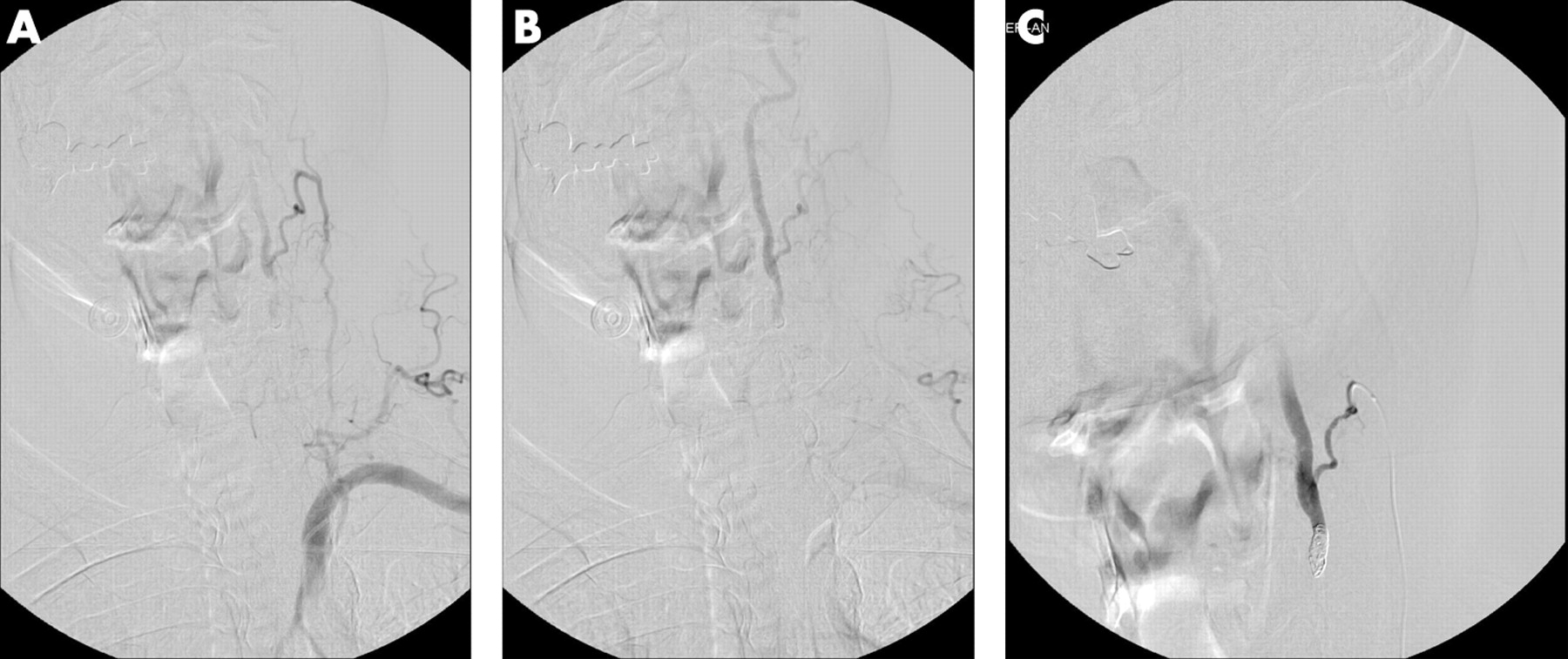
Angiography confirmed occlusion of the left vertebral artery (fig 1a), with distal antegrade flow via the deep cervical artery at C5 (fig 1b). At the distal end of the occlusion, there was a filling defect corresponding to a thrombus. The right vertebral artery was normal. The working diagnosis was recurrent ischaemic events from the vertebral artery stump or a low flow state from the vertebral occlusion.
{kind=link}
Due to failed medical therapy, an endovascular intervention was undertaken to exclude the embolic source. The deep cervical artery was catheterised to retrogradely reach the distal end of the vertebral artery thrombus. Five coils were placed to exclude the embolic source (fig 1c). The patient was placed on warfarin for 1 month, followed by aspirin. At the 1-year follow-up, he reported no further events.
CASE 2
A 54-year-old man presented with vertigo, blurred vision and gait instability. Examination revealed a left superior quadrantanopsia. Magnetic resonance imaging showed a right occipital-temporal infarct. Angiography revealed a left vertebral artery occlusion at its origin, with distal reconstitution at C1 by a deep cervical artery collateral. The right vertebral artery was co-dominant and normal in caliber. The patient was placed on aspirin.
Two weeks later, the patient developed decreased verbal output, right-sided hypoesthaesia and right facial weakness. Magnetic resonance imaging revealed an infarct in the left thalamocapsular region, left infero-occipital and temporal lobe. Angiography showed persistent occlusion of the left vertebral artery at its origin, with distal reconstitution by the deep cervical artery.
Due to the presence of antegrade flow distal to the vertebral occlusion, an intervention to occlude the distal end of the vertebral artery was undertaken. A microcatheter was navigated retrogradely via the right vertebral artery to the left vertebral artery proximal to the C1 collateral. Coils were placed to exclude the embolic source at the vertebral artery. The patient was treated with clopidogrel (for 1 year) and aspirin. At the 3-year follow-up, there were no further events.
DISCUSSION
These two cases illustrate the likely role of vertebral artery stump embolism as a mechanism to consider for patients with persistent ischaemic events in the posterior circulation after imaging confirmation of vertebral artery occlusion. We adopted “vertebral stump syndrome” because of clinical similarities to the carotid stump syndrome, in which patients experience a delayed ischaemic event distal to a documented arterial occlusion.
Anatomy of collaterals to the vertebral artery
The vertebral artery benefits from numerous potential anastomoses because of its embryological development. The vertebral artery is the result of the union of multiple metameric vascular segments. After its formation, each segmental level possesses vascular connections to cervical arteries at a metameric level, of which there are three prominent axes: the cervical, occipital and ascending pharyngeal arteries.4
The cervical axis originates from the subclavian artery and gives rise to the deep and ascending cervical arteries. The deep cervical artery usually originates from the costocervical trunk, runs posterior to the vertebral artery and anastomoses to the vertebral artery at the C5 or C6 levels.4 The ascending cervical artery usually originates from the thyrocervical trunk, courses anterior to the vertebral artery and anastomoses to the vertebral artery at C3 or C4.
The occipital artery anastomoses with the vertebral artery at C1 or C2. The ascending pharyngeal artery can anastomose with the occipital artery from its musculospinal branch. These collaterals, if well developed, may take over the supply of the proximal occluded vertebral artery, permitting a persistent antegrade flow.
Pathophysiology of stump syndrome
Three potential mechanisms explain the recurrence of ischaemic events from an artery-to-artery embolus after documented vessel occlusion: 1) embolus of stagnating clot fragments; 2) a low flow state; and 3) stump or other embolus through a collateral.
Embolisation of fragments from the distal part of the thrombus can expose a patient to new thromboembolic events. This requires persistence of an antegrade flow distal to the occlusion to transport emboli intracranially. In the setting of vertebral artery occlusion, the vertebro-basilar system favours flow reversal of the contralateral vertebral artery to perfuse the V4 segment distal to the occluded vertebral artery. Because antegrade flow for distal embolus propagation is not favoured by this flow reversal, embolisation after a documented vertebral occlusion is probably prevented by this haemodynamic state. Cervical collaterals may compete to preserve an antegrade flow that may carry a fragment of thrombus.
A low flow state induced by an occlusive thrombus is another contributing mechanism. Hypoperfusion and embolism can coexist and interact, perhaps synergistically, to cause an ischaemic event.5 In addition, reduced blood flow could reduce the washout and clearance of emboli in hypoperfused regions.5
The third hypothesis, as with the classical carotid stump, involves a thrombus formed by stagnating flow, detached by turbulent flow in the stump, carried intracranially via collaterals. In the posterior circulation, the corollary may occur with a vertebral artery occlusion, where a proximal stump would be carried intracranially via cervical artery collaterals. However, this is difficult to conceptualise because the thrombus would have to dislodge into the subclavian artery, escaping the blood flow of a major artery to embolise in collaterals. Another possibility of recurrent stroke is propagation of a thrombus other than that formed by the stump, through the collateral.
In our patients, no proximal stump was seen at the origin of either patient, hence we favour the pathogenesis of recurring stroke due to stagnating thrombus distal to the occlusion. The resolution of events following endovascular exclusion of the distal thrombus supports this hypothesis, although it is possible that the symptoms would have resolved in spite of the intervention due to the benign natural history of this condition. Although the goal of placing coils into the vertebral artery distal to the thrombus was to exclude the embolic source, we acknowledge that this coil mass could have been a new nidus for thrombus formation. An alternative therapy could have been to embolise the collateral branch to prevent antegrade flow from the left vertebral artery to the intracranial circulation, given the presence of a contralateral right vertebral artery.
CONCLUSION
In patients with posterior circulation stroke, presence of a vertebral artery occlusion does not preclude the development of further ischaemic events. A vertebral stump syndrome, analogous to the carotid stump syndrome, can explain some of these events. Endovascular exclusion of the embolic source may be considered if medical therapy has failed.
Footnotes
Competing interests: None declared.