Article Text

Abstract
Introduction The direct aspiration first pass technique (ADAPT) has been introduced as a rapid and safe endovascular treatment strategy in patients with ischemic stroke.
Objective To determine the technical feasibility, safety, and functional outcome with ADAPT using the new large-bore 6F SOFIA Plus catheter.
Methods A retrospective analysis of prospectively collected data from six university hospitals was performed. The following parameters of all acute stroke procedures (June 2015– January 2016) using the SOFIA Plus catheter were analyzed: accessibility of the thrombus with the catheter, recanalization success (Thrombolysis in Cerebral Infarction ≥2b), time to recanalization, procedure-related complications. Furthermore, National Institutes of Health Stroke Scale (NIHSS) scores at presentation and discharge and the modified Rankin scale (mRS) score at 90 days were recorded.
Results 85 patients were treated using the SOFIA Plus catheter. The occlusion site was the anterior circulation in 94.1%. Median baseline NIHSS score was 18. In 64.7%, ADAPT alone was successful after a median procedure time of 21 min. With additional use of stent retrievers in the remaining cases, the recanalization rate was 96.5%. No catheter-related complications such as dissections were observed. Thrombus migration to a new vascular territory occurred in 4.7% and symptomatic hemorrhage in 4.7%. After 3 months, mRS 0–2 was achieved in 49.4%. Mortality rate was 20%.
Conclusions In the majority of cases, thrombus aspiration using the SOFIA Plus catheter results in successful recanalization after a short procedure time. With additional use of stent retrievers, a high recanalization rate can be achieved (96.5%). The complication rate was in line with those of previous publications.
- Catheter
- Intervention
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Introduction
Over the past decade, advances in thrombectomy devices and catheter technology have enabled new endovascular strategies for the treatment of acute ischemic stroke. Beside the introduction of stent retrievers, an important innovation was the introduction of ADAPT (a direct aspiration first pass technique) enabled by the development of new large-bore catheters.1–3 Despite their large caliber, they are highly trackable and allow navigation directly to the thrombus site owing to their atraumatic and flexible design. At the thrombus site, aspiration is applied to engage and remove the thrombus. Passage of the thrombus is not required. In a large number of cases, rapid recanalization can be achieved without additional use of stent retrievers.2 In unsuccessful cases, the treatment regimen can be changed easily by using the large-bore catheter approach for stent retriever devices.
This study was designed to assess the safety and efficacy of the new 6F SOFIA Plus catheter (Soft torqueable catheter Optimized For Intracranial Access, MicroVention, Tustin, California, USA) as a first-line lesional aspiration catheter for endovascular stroke treatment. Compared with other aspiration catheters, it has the largest distal inner luminal diameter (0.070″), and, therefore, should offer a higher aspiration flow rate and a greater force of aspiration at the tip of the catheter.4 The main focus of our study is the technical feasibility (distal catheter navigation, recanalization success with and without additional devices), safety concerns (procedure- and catheter-related complications), and functional outcome with ADAPT.
Patients and methods
Patients
Approval of the local ethics committee of the participating centers was obtained. Prospectively collected data of six participating centers were retrospectively analyzed. All patients who underwent acute stroke procedures using the SOFIA Plus catheter between June 2015 and January 2016 were identified. At all centers, the use of the SOFIA Plus catheter for endovascular recanalization procedures was at the operator’s discretion.
Inclusion criteria for endovascular therapy were large arterial occlusions proved by CT angiography or MR angiography, no signs of major infarction (more than one-third of the middle cerebral artery territory) on CT or MRI, and baseline National Institutes of Health Stroke Scale (NIHSS) score ≥5 or aphasia if the score was <5. If eligible, patients received IV thrombolysis (IVT).
Catheter
The newly designed SOFIA Plus catheter obtained CE mark approval in Europe in February 2015. It has a hybrid braid-coil design and is available in two different lengths (125 cm or 131 cm) with an outer diameter of 6F and an inner luminal diameter of 0.070 inch from distal to proximal zones. The catheter tip has a straight configuration but is steam shapeable.
Interventional procedure
The interventional procedures were performed under general anesthesia or conscious sedation, depending on the local setting. Via transfemoral access, a 6F or 8F guide catheter (Neuron MAX 6F or Vista Brite Tip 8F) was placed in the common carotid artery (or internal carotid artery depending on the interventionalist’s preference) of the affected side or in the subclavian artery in cases of posterior circulation occlusions. Subsequently, the SOFIA Plus catheter was carefully advanced to the level of the occlusion, usually over a 0.021 or 0.027 microcatheter and a microwire. It seems that in some cases the SOFIA Plus tracks better with a 0.027 microcatheter. Different microwires were used such as Transend, Synchro2, Traxcess, Traxcess EX. After positioning the SOFIA Plus catheter with the catheter tip inside the proximal part of the thrombus, microcatheter and microwire were removed and aspiration was started using a vacuum pump or a 20–60 mL syringe trying to remove the clot. As soon as absence of flow was noted, aspiration was continued for approximately 3 min. When no flow through the system was found, the catheter was removed slowly under additional aspiration at the guide catheter. If insufficient recanalization was achieved, the aspiration attempt was either repeated aiming to engage the clot at the distal tip of the aspiration catheter or, alternatively, an additional thrombectomy device was used. The choice between these two options was at the discretion of the operator.
Evaluation of angiographic data
For analysis of the angiographic images, the following parameters were documented: time from symptom onset to the first diagnostic angiogram, site of occlusion, accessibility of the thrombus with the large-bore catheter, initial and final Thrombolysis in Cerebral Infarction (TICI) score5 ,6 with recanalization success defined as TICI ≥2b (self-assessed by the respective site), recanalization by lesional aspiration alone or requirement for additional devices, time from the first angiographic image to the completion angiogram, procedure-/catheter-related complications such as vessel dissections, periprocedural hemorrhage due to vessel perforation, and emboli to initially uninvolved vascular territories.
Evaluation of outcome data
For quantification of the neurological deficit, the NIHSS scores on admission and discharge were noted as well as the modified Rankin scale (mRS) score after 90 days. mRS at 3 months was obtained during a standardized telephone follow-up or an outpatient visit by a neurologist not involved in the initial treatment. Favorable clinical outcome was defined as mRS score 0–2.
Follow-up CT scans were obtained approximately 24 hours after symptom onset or earlier if clinical deterioration occurred. Symptomatic intracranial hemorrhage was defined according to the European Cooperative Acute Stroke Study II classification.7
Statistics
Differences between groups were tested using Student's t test for continuous variables and a χ2 test or Fisher's exact test for categorical variables, as appropriate. All tests were two-sided and assessed at a significance level of 0.05. Statistical analyses were performed using SPSS (IBM SPSS Statistics for Windows, V.22.0. Armonk, New York, USA: IBM Corp.).
Results
Patients
Table 1 gives an overview of baseline characteristics and angiographic and clinical data. Between June 2015 and January 2016, 85 patients were treated with the SOFIA Plus catheter; 47 were women (55.3%). Mean age was 72.6 years (range 20–94 years). Sixty per cent of the patients received IVT. The target lesions were in the anterior circulation (internal carotid artery terminus n=15, M1 segment n=62, M2 segment n=3) and in the posterior circulation (basilar artery n=5). Twenty patients (23.5%) presented with an unknown time of symptom onset. In the remaining patients, the median time from symptom onset to the first diagnostic angiogram was 187 min (IQR 139–222.5 min).
Baseline characteristics and overview of angiographic and clinical outcome data
In seven patients a stenotic lesion of the proximal cervical internal carotid artery required balloon angioplasty and stent implantation to gain access to the intracranial vasculature.
Evaluation of angiographic data
Pretreatment TICI was 0 in 79 cases (92.9%), 1 in 3 cases (3.5%) and 2a in 3 cases (3.5%). The large-bore catheter could be navigated without the help of a stent retriever to the occlusion site in 91.8% of cases. In seven cases (8.2%), navigation of the catheter to the thrombus was not possible owing to unsuccessful passage of the ophthalmic artery origin (n=5) or extreme vessel tortuosity (n=2). The so-called thrombus-no-touch technique (TNT) was successfully used in 56.5% in a subgroup of patients (13/23) as shown in figure 1. With this technique, navigation with a microwire/microcatheter through the occlusion is not needed for placement of SOFIA Plus inside the thrombus. Overall, TICI ≥2b could be achieved in 82 patients (96.5%). Aspiration alone was successful in 55/85 patients (64.7% of the procedures) (TICI 2b n=7, TICI 2c n=4, TICI 3 n=44) with a median recanalization time of 21 min (IQR 16–30 min) and a mean of 1.2 aspiration attempts (range 1–4). In patients with successful navigation of the SOFIA Plus catheter to the occlusion site (78/85 patients), aspiration was successful in 70.5%.
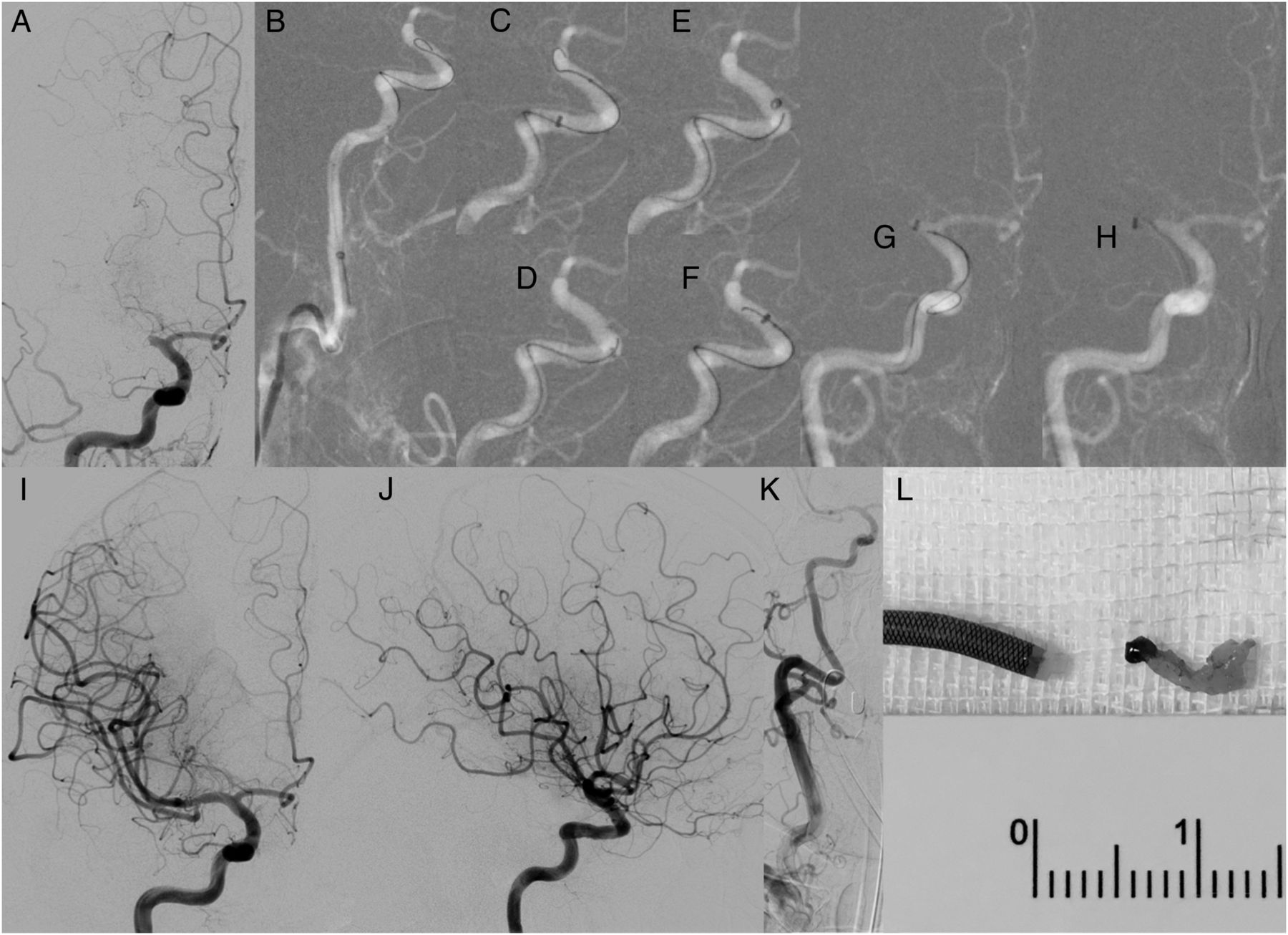
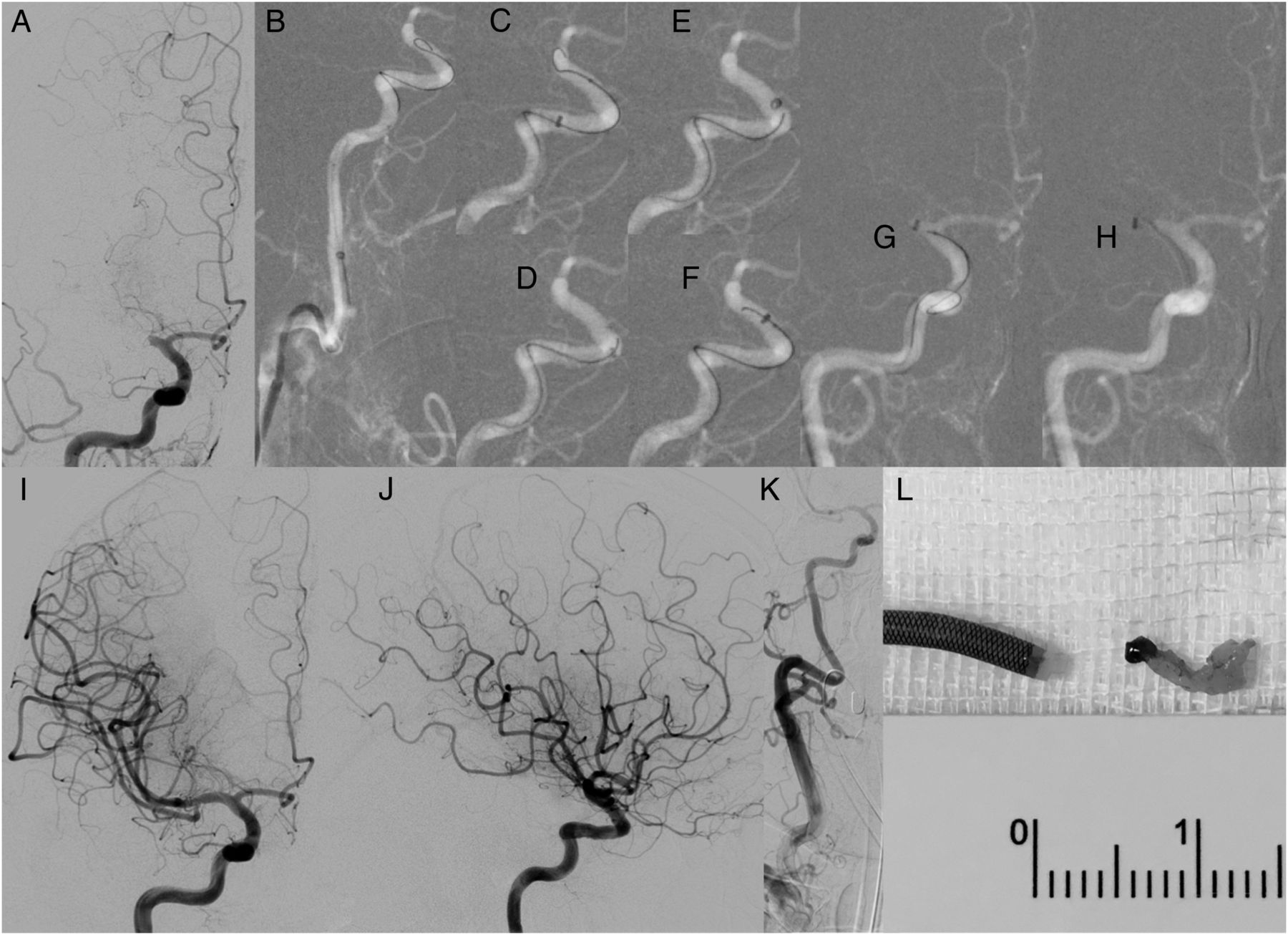{kind=link}
Septuagenarian with a National Institutes of Health Stroke Scale score of 18 and a right M1 occlusion (anteroposterior (ap) view (A)). Navigation of SOFIA Plus together with a Traxcess microwire and a Rebar 18 microcatheter along the extracranial internal carotid artery (lateral (lat) view (B)). Navigation of SOFIA Plus along the carotid siphon without the need to cross the occlusion with the microwire/-catheter system (lat view (C–F)). Positioning of SOFIA Plus within the proximal part of the thrombus, again without the need to cross the occlusion with the microwire/-catheter system (thrombus no-touch technique; ap view (G, H)). After 3 min aspiration a Thrombolysis in Cerebral Infarction score of 3 was obtained within a procedure time of 14 min (ap view (I); lat view (J)). Final angiogram of the common carotid artery showed no signs of vasospasm or dissection (ap view (K)). An almost complete ‘white’ clot was aspirated into the SOFIA Plus with a 60 cc syringe (L). After 3 months the patient's modified Rankin Scale score was 1.
In the majority of these patients (92.9%), the first aspiration attempt was successful. After sole aspiration, TICI remained unchanged (TICI 0) in five cases. In six cases, improvement to TICI 1 and in 12 cases improvement to TICI 2a could be achieved. In four patients, additional aspiration with the Sofia 5F catheter was performed in the M1/2 segments after initial aspiration with the SOFIA Plus catheter. This resulted in recanalization according to TICI 2b–3 in all of these patients. Before change of the treatment strategy and use of additional stent retriever devices, on average 1.7 aspiration attempts had been performed insufficiently. Altogether, in 30/85 patients, additional devices (Solitaire 2, Covidien/Medtronic; ERIC, MicroVention; Trevo ProVue, Stryker; EmboTrap, Neuravi; pREset, Phenox) were used with successful recanalization in 27 of these patients (TICI 2b n=13, TICI 2c n=5, TICI 3 n=9) after a median recanalization time of 53 min (IQR 40–67).
Evaluation of outcome data
Median NIHSS score was 18 at presentation (IQR 12–21.5). At discharge, the median NIHSS score of the surviving patients was 4.5 (IQR 1.8–12.25).
After 90 days, 17 patients (20%) had died.
The median mRS of the surviving patients was 2 (IQR 1–3). Favorable clinical outcome (mRS 0–2) was noted in 42 patients (49.4%).
There was no statistically significant difference in the outcome between patients who received IVT and those who did not receive IVT.
Complications
In four patients, emboli to a new vascular territory occurred during aspiration with the SOFIA Plus catheter, which resulted in additional use of a stent retriever. In four patients, symptomatic intracranial hemorrhage within the infarction area occurred in the further course. In one patient, arterial dissection at the puncture site resulted in a retroperitoneal hematoma without the need for blood transfusion.
Discussion
In recent years, ADAPT has been introduced to facilitate recanalization procedures by direct aspiration at the thrombus site.1 ,2 Briefly, a large-bore catheter is positioned directly at the occlusion site and the thrombus is removed via aspiration. It has been reported that ADAPT is effective and also improves the time to recanalization.8 These parameters are essential as good clinical outcome is known to be associated with both complete and rapid recanalization.9–12
An in vivo study by Hu et al 4 evaluated force and aspiration requirements of ADAPT. They reported that several parameters contribute to the success of ADAPT. For catheter tip corking, a high aspiration flow rate is required to pull the thrombus into the catheter tip. Then, a high catheter tip force is needed. This force is characterized as a static force that the catheter tip impacts on the thrombus, which has already been pulled into the catheter. The authors concluded that the catheter with the largest tip diameter will have the greatest tip force. At present, the 6F SOFIA Plus catheter is the only catheter with a proximal to distal inner lumen of 0.070″, and, thus, the largest available aspiration catheter.
In our current multicenter study, a relatively large number of patients were included. The thrombus site was accessible in the majority of cases (91.8%) without support of a stent retriever despite the large lumen diameter of the aspiration catheter. However, it is known that in patients with tortuous arteries, passage of the ophthalmic artery origin might be difficult or even impossible when using large-bore catheters.
As a solution, several techniques can be considered: first, a stiffer microcatheter can be used for better support. Second, a larger microcatheter can be used in order to reduce the gap between the microcatheter and the SOFIA Plus catheter at the outer curve of the entire system when navigating along the carotid siphon. Furthermore, steam shaping of the SOFIA Plus catheter tip can be performed to overcome difficulties with catheter navigation. In the literature, a special technique (the so-called ‘Rocket technique’) is recommended for atraumatic distal navigation of large-bore catheters in complicated cases.13 The authors describe the use of a coaxial system with a compliant balloon catheter and a large-bore catheter. The balloon catheter is inflated with the inflation zone overlapping the distal tip of the large-bore catheter, and then advanced together with the coaxial system to the thrombus site. Once the balloon catheter reaches the thrombus site, the balloon is deflated and the large-bore catheter can be guided to the occlusion. The Rocket technique was successfully applied in two procedures of our study. It might be an option to solve the problem with hindered ophthalmic artery origin passage in the future.
In the majority of ADAPT cases, additional devices are not required. If recanalization attempts with ADAPT technique fail or the occlusion site cannot be reached with the aspiration catheter, change of the treatment strategy is easy, because the large-bore catheter can be used as a platform for stent retrievers. In the literature, sole lesional aspiration resulted in successful recanalization in a varying percentage of cases (between 56%14 (5 MAX ACE, Penumbra) and 78%2 (5 MAX and 5 MAX ACE, Penumbra)). This variation might be caused by the operators’ decision about how many attempts at aspiration should be made before the treatment strategy is changed. In our study, successful recanalization was achieved by sole aspiration in 64.7%. In the majority of cases (92.9%), only one aspiration attempt was required. Therefore, one might hypothesize that change of the treatment strategy should be considered after the first futile aspiration attempt. With ADAPT and the optional use of additional devices, high recanalization rates have been reported (up to 96.8% TICI 2b/3 in an oral presentation introducing the ACE 64 catheter at the World Federation of Interventional & Therapeutic Neuroradiology meeting 2015).15 Correspondingly, TICI ≥2b was achieved in 96.5% in our study.
The percentage of patients with mRS 0–2 (49.4%) and the mortality rate are in line with literature reports. In the ADAPT FAST study, Turk et al 2 found an overall good functional outcome of 40% and a mortality rate of 20%.
Periprocedural embolization to initially uninvolved vascular territories is a major concern when performing endovascular recanalization procedures and contributes to an unfavorable clinical outcome.16 ,17 ADAPT lowers the risk of embolic complications, because passage of the thrombus before the aspiration is often not necessary and the thrombus is frequently extracted en bloc. In particular, the occurrence of large hard clot fragments can be reduced.18 However, it has been reported that emboli to new vascular territories occur in approximately 2–6% of ADAPT procedures.14 ,19 ,20 In our study, embolic complications were detected in 4.7% of cases. A reduction in distal embolic complications could possibly be achieved through the TNT. With this technique, navigation with a microwire/microcatheter through the occlusion is not needed for placement of SOFIA Plus inside the thrombus. This TNT technique was successfully used in 56.5% in a subgroup of patients (13/23). However, the frequency of small distal emboli following mechanical recanalization is unknown, and it is unclear whether the risk of small distal embolizations differs between recanalization techniques.
ADAPT has been reported to be associated with less symptomatic intracranial hemorrhage than the Solumbra technique (distal aspiration during stent retrieval) probably owing to less endothelial damage.21 Our overall rate of symptomatic intracranial hemorrhage of 4.7% is in line with data from other aspiration catheter studies ranging from 2.4% to 6.8%.14 ,19 ,22
We are aware of several potential study limitations. First, the study was retrospective with no control group. The angiographic images were self-adjudicated and, therefore, the results might be biased towards better TICI scores. Furthermore, we included patients with occlusions of the anterior and posterior circulation, resulting in heterogeneity of the study population.
Conclusion
The new large-caliber SOFIA Plus catheter for lesional aspiration is effective leading to recanalization success and reduced time to recanalization. In unsuccessful cases, stent retriever devices can easily be added to the treatment strategy. No complications directly related to the catheter positioning were seen. Other complications, such as emboli to new vascular territories and symptomatic intracranial hemorrhage, were in line with published reports on other aspiration catheters.
References
Footnotes
Contributors MAM, SS: study conception and design, interventions, acquisition of data, analysis and interpretation of data, drafting of the manuscript; CK, AK, EB, MS, MM, MW, JT, MK-O, WW, AM, MB: study conception and design, interventions, acquisition of data, critical revision of the manuscript.
Competing interests MAM: has received consulting honoraria, speaker honoraria, and travel support outside this work from Codman, Covidien, MicroVention, Phenox, and Stryker; MS: congress support from MicroVention, Medtronic, and Stryker, outside the submitted work; MW: has been working as a consultant for Stryker Neurovascular, has received reimbursement for lectures or travel support from Bracco, Covidien, Siemens, Stryker Neurovascular, has received grants for research projects or educational exhibits from Abbott, ab medica, Acandis, Bayer, Bracco, B Braun, Codman Neurovascular, Covidien, Dahlhausen, MicroVention, Penumbra, Phenox, Philips, Siemens, SilkRoad Medical, St Jude, Stryker Neurovascular; JT: educational grants from Medtronic, Bracco, Guerbet, and Johnson Johnson, travel grants (conferences) from MicroVention, Stryker; MK-O: grants from MicroVention/Terumo, during the conduct of the study; WW: consultant for MicroVention/Terumo; AM: consultancy for Neuravi, Penumbra, and Sequent Medical, modest honoraria; MB: board membership: DSMB Vascular Dynamics; consultancy: Roche, Guerbet, Codman; grants/grants pending: DFG, Hopp Foundation, Novartis, Siemens, Guerbet, Stryker, Covidien; payment for lectures (including service on speakers bureaus): Novartis, Roche, Guerbet, Teva, Bayer, Codman.
Ethics approval Approval of the local ethics committees of the participating centers was obtained.
Provenance and peer review Not commissioned; externally peer reviewed.