Article Text

Abstract
Background and purpose Multiple aneurysms have a high reported incidence, but the optimal treatment strategy is not clear. The aim of this study was to evaluate the safety and effectiveness of single-stage endovascular treatment of multiple aneurysms with a combination of various endovascular techniques.
Materials and methods Fifty-three consecutive patients with multiple intracranial aneurysms who underwent single-stage endovascular treatment for ≥2 aneurysms from June 2011 to May 2016 were included in the study. Patient and aneurysm characteristics, treatment technique, complications, clinical and angiographic outcomes were retrospectively evaluated.
Results 125 of 128 aneurysms (97.6%) were treated by the following endovascular techniques: simple coiling in 19, balloon-assisted coiling in 27, stent-assisted coiling in 33, flow diverters in 43, intrasaccular flow modifiers in 2, and a neck-bridging device in 1. Overall mortality and mortality directly related to the single-stage treatment was 15% (8/53) and 3.7% (2/53), respectively. Clinical and angiographic follow-up was available in 44 (83%) patients for 104 (83.2%) aneurysms for a mean duration of 16.2 months (range 3–51 months). According to the last angiographic follow-up, overall occlusion rates were complete in 85 (81.7%), near complete in 8 (7.6%), and incomplete in 11 (10.5%) aneurysms.
Conclusions Single-stage endovascular treatment of multiple aneurysms with combined endovascular techniques is technically feasible and increases the treatment possibility of all detected aneurysms. However, the safety of the procedure is controversial due to relatively high complication rates. In particular, in patients with bilateral internal carotid artery aneurysms, staged therapy may be used instead of simultaneous treatment with flow diverters to avoid thromboembolic events.
- Aneurysm
- Coil
- Flow Diverter
- Stent
- Balloon
Statistics from Altmetric.com
Introduction
The prevalence of intracranial aneurysms is around 2%,1 and approximately 15–34% of patients have multiple aneurysms presenting with subarachnoid hemorrhage (SAH).2 ,3 Patients with multiple aneurysms carry a higher risk than those with a single aneurysm because of the higher associated mortality and significantly poorer outcome.2 ,4 There is no clear consensus about the optimal management of multiple aneurysms but, if possible, all aneurysms should be treated because of the natural course of the disease.5 In the last decades endovascular treatment has gained popularity and become a reasonable alternative for the treatment of intracranial aneurysms.6–8 Improvements in endovascular techniques and devices such as remodeling balloons,9 stents,10 neck-bridging devices,11 flow diverters,12 and intrasaccular flow modifiers13 have provided important advances in the endovascular treatment of wide-necked and complex aneurysms and have broadened the patient selection criteria. However, in contrast to the high reported incidence, studies of endovascular treatment of multiple aneurysms are limited14–18 and have focused on coiling, while surgical management has been well studied.2 ,4 ,19 ,20 Moreover, there are no data regarding the efficacy and usage of flow diverters, intrasaccular flow modifiers, or neck-bridging devices in existing endovascular studies.
The purpose of this study was to evaluate the safety and effectiveness of single-stage endovascular treatment of multiple intracranial aneurysms with a combination of different techniques and devices.
Materials and methods
Fifty-three consecutive patients with multiple intracranial aneurysms who underwent single-stage endovascular treatment for ≥2 aneurysms from June 2011 to May 2016 were included in the study. Patient and aneurysm characteristics, treatment technique, complications, clinical and angiographic outcomes were retrospectively evaluated.
The aneurysm size, morphology, and distribution were determined via angiographic evaluation. Aneurysm sizes were classified as small (<10 mm), large (≥10 and ≤25 mm), and giant (>25 mm). Wide-necked aneurysms were defined as a dome-to-neck ratio <2:1 and/or a neck length of >4 mm. Complex aneurysms were defined as multilobulated aneurysms or an aneurysm with branches originating from the aneurysm sac.
Criteria for single-stage endovascular treatment
The decision of the treatment modality and technique to be used was made by consensus of the neurosurgical and neurointerventional physicians after careful evaluation of each patient as part of a multidisciplinary decision-making process, and the choice of single-stage treatment was based on the following criteria.
Patient-related factors
In cases with uncontrolled hypertension, smoking, associated diseases and clinical conditions which carry the risk of repeated general anesthesia, a family history of SAH, early age, planned pregnancy in female patients, and the need for hypertensive therapy in the period of vasospasm in patients with SAH, the detected aneurysms were planned to be treated in a single stage.
Aneurysm and technique-related factors
In cases with risk factors and associated symptoms in further aneurysms (size, complexity, irregular shape of aneurysmal sac or presence of bleb formation, presence of mass effect and cranial nerve palsy) and those in whom the distribution of the aneurysms was not suitable for surgical access (bilateral and/or both anterior and posterior circulation) or easily accessible with the endovascular approach (aneurysms along the same arterial tree), the detected aneurysms were planned to be treated in a single stage by the endovascular approach.
If the primary targeted aneurysm required the use of stents as well as antiplatelet therapy, the secondary targeted aneurysms were planned to be treated in the same stage so that the remaining aneurysms were not left unsecured under antiplatelet therapy. On the other hand, if the primary targeted aneurysm was treated without the use of stents and antiplatelets but the treatment of secondary targeted aneurysms required them, the procedure was planned to be staged, especially in patients with SAH. In patients with unruptured aneurysms, more complex and distal aneurysms were treated first. In patients with SAH, ruptured aneurysms were treated first. Prediction of ruptured aneurysms was evaluated using Nehl's algorithm.21 If ruptured aneurysms were not clearly detected, more complex aneurysms were treated first and the remaining aneurysms were treated in the same session.
As distinct from the current study cohort, 18 other patients with multiple aneurysms were also treated by the endovascular approach during the same study interval but were not included in the study. In five of them the detected aneurysms were treated in staged sessions (one aneurysm per stage), depending upon the prolonged procedural times and anesthesia and clinical condition of the patients, in addition to the algorithm explained above. In 13 of them only the targeted aneurysm (the ruptured aneurysm in patients with SAH or the most evident aneurysm in elective patients) was treated alone and the remaining aneurysms were left untreated depending on the morphologic features (very small size of aneurysm and smooth wall contour) and also patient-related factors such as poor clinical grade, low life expectancy due to associated comorbidities (malignancy, severe heart failure) and those aged >75 years.
Technique
All procedures were performed under general anesthesia by a standard transfemoral approach with a combination of a 6 Fr introducer sheath and 6 Fr guiding catheters. Aneurysms were treated using the following techniques and devices: single catheter coiling, balloon-assisted coiling (BAC), stent-assisted coiling (SAC) with Solitaire AB (Covidien/ev3, Irvine, California, USA), LVIS Jr (MicroVention, Tustin, California, USA), and ACCLINO flex (Acandis, Pforzheim, Germany), flow diverters (FDS) with Pipeline and PipelineFlex (Covidien/ev3), Derivo (Acandis, Pforzheim, Germany), and FRED (MicroVention), intrasaccular flow modifiers with WEB-DL (Sequent Medical, Aliso Viejo, California, USA), and neck-bridging device with pCONus (phenox, Bochum, Germany). SAC was performed with the assistance of single or double stents in a Y configuration by using the jailing technique. In cases treated with FDS, the aneurysms were either treated solely with FDS or with adjunctive endosaccular coils.
Antiplatelet medication protocol in SAC and FDS
All patients were heparinized to maintain an activated clotting time of 250–300 s during the procedure and then discontinued. Patients with unruptured aneurysms were premedicated with 100 mg aspirin and a loading dose of 600 mg clopidogrel 1 week before the procedure, followed by 75 mg daily clopidogrel and 100 mg aspirin. Thrombocyte inhibition levels were confirmed by the rapid platelet function Assay VerifyNow P2Y12 (Accumetrics, San Diego, California, USA) and an inhibition value of >30% was accepted for treatment. Patients with clopidogrel resistance were medicated with ticlopidine 2×250 mg or prasugrel 1×10 mg. In patients with SAH, 600 mg clopidogrel and 100 mg aspirin or 60 mg prasugrel alone were loaded via a nasogastric tube just before treatment and the patients were maintained on daily doses of 75 mg clopidogrel and 100 mg aspirin or 10 mg prasugrel alone. Platelet inhibition levels were also confirmed in patients with SAH after the procedure. Dual antiplatelet therapy was switched to life-long aspirin monotherapy after the control angiogram was obtained at 1 year.
The preoperative clinical condition of the patients with SAH was evaluated using the Hunt and Hess classification.22 All procedural and disease-related complications and mortality were evaluated in patients with SAH and unruptured aneurysms. Patients were regularly followed up by clinical examination initially at 1 month and then at 3-monthly intervals during the first year followed by yearly intervals. Follow-up angiographic imaging was performed at 3–12 months and then at 24–48 months. Clinical outcome was measured after procedure, at discharge, and at the time of follow-up using the modified Rankin Scale (mRS).23 Aneurysm occlusion was evaluated according to the Raymond classification in the coil embolization group as complete occlusion, neck remnant, and residual aneurysm.24 The outcome for aneurysms treated with FDS was evaluated according to the O'Kelly-Marotta (OKM) grading scale,25 and the outcome for aneurysms treated with WEB-DL was evaluated using a four-grade scale described by Lubicz et al 26 (complete occlusion, complete occlusion with opacification of the proximal recess of the device, neck remnant, and aneurysm remnant). Angiographic follow-up results were classified as stable, improved, and recanalization compared with immediate postoperative angiograms. According to the final angiographic follow-up data, aneurysm occlusion was classified as complete (no filling in the aneurysm; Raymond class I, OKM grade D, Lubicz grade A), near complete (residual filling at the neck; Raymond class II, OKM grade C, Lubicz grade B and C), and incomplete (residual filling at the aneurysm sac; Raymond class III, OKM grade A and B, Lubicz grade D).
Results
Patient and aneurysm characteristics are summarized in table 1.
Characteristics of patients and aneurysms
In 53 patients, 125 of 128 aneurysms (97.6%) were treated by a combination of the following endovascular techniques: single catheter coiling in 19 aneurysms, BAC in 27 aneurysms, SAC in 33 aneurysms (18 aneurysms with single stent, 14 aneurysms with double stents in Y configuration, 1 aneurysm stented alone without coiling), FDS in 43 aneurysms (7 aneurysms with adjunctive endosaccular coiling), WEB-DL in 2 aneurysms, and a neck-bridging device in 1 aneurysm. The treatment technique, devices used, and location of treated aneurysms are given in table 2.
Treatment technique, devices used, and location of treated aneurysms
In 50 patients (94.3%) the detected aneurysms were treated in a single stage while two-stage treatment was used in three patients (5.6%). All three patients treated in two stages presented with SAH and the decision to use two-stage treatment was based on the patients' clinical condition, morphological features of the aneurysms, and the complexity of the procedures. In the first patient with five aneurysms including the left distal anterior cerebral artery (DACA), left A1, left middle cerebral artery (MCA) bifurcation, and two mid-basilar fenestrated kissing aneurysms, four of the detected aneurysms were treated in the first stage (DACA aneurysm with SAC, MCA bifurcation aneurysm with BAC, left A1 and one of the mid-basilar aneurysms with single catheter coiling). The remaining mid-basilar kissing aneurysm was left untreated in the first stage because of its small size (2.5 mm) and the need for a complex SAC technique through the fenestrated segments which was judged to be too risky in the acute period; it was treated in a second stage after 6 months with SAC. In the second patient with three aneurysms including two right ICA and right MCA bifurcation aneurysms, the two ICA aneurysms were treated with BAC in the first stage and the MCA aneurysm was treated 1 week later in a second stage with SAC after the acute period. In the third patient with left and right paraopthalmic ICA aneurysms, the ruptured left ICA aneurysm was treated with partial coiling in the first stage and 12 days later both the partially coiled left ICA and the remaining right ICA aneurysms were treated with FDS simultaneously in a second stage after the acute period. In three patients three aneurysms were left untreated because of the very small size (<1.5 mm) in two and the unstable clinical condition during treatment in one patient. SAC and/or FDS were used in the treatment of 21 aneurysms in 14 patients in the acute stage of SAH.
Complications and mortality
The rates of any complication and complications directly related to the single-stage treatment were 20.7% (11/53; 8 (15.%) in the unruptured group, 3 (5.6%) in the SAH group) and 9.4% (5/53; 4 (7.5%) in the unruptured group, 1 (1.8%) in the SAH group), respectively. Overall mortality and mortality directly related to the single-stage treatment were 15% (8/53; 2 (3.7%) in the unruptured group, 6 (11.3%) in the SAH group) and 3.7% (2/53; 1 (1.8%) in the unruptured group, 1 (1.8%) in the SAH group), respectively. Specifically, in the unruptured aneurysm group, eight patients had complications including delayed aneurysm rupture in one patient, periprocedural aneurysm perforation in two, and thromboembolic events in five patients. In two patients one periprocedural and one delayed stent thrombosis (at day 10) were treated with tirofiban infusion successfully. However, in one patient delayed mechanical stent occlusion (at day 12) caused loss of the parent artery (figure 1). Thromboembolic complications resulted in death in two patients. One was from bilateral stent occlusion at day 5 after simultaneous treatment of bilateral ICA aneurysms (n=5) with FDS due to the discontinuation of antiplatelet therapy by the patient. The second was from a left hemispheric infarct at day 2 after treatment of the left giant ICA terminus and right ICA paraclinoid aneurysms with BAC. Of the three hemorrhagic complications, one was from delayed rupture of the giant paraclinoid ICA aneurysm at day 14 after treatment with FDS and the aneurysm was retreated with an additional FDS. The other two were from aneurysm perforation during coiling which was controlled with temporary balloon occlusion and further coiling. All these patients recovered without serious neurological deficits.
{kind=link}
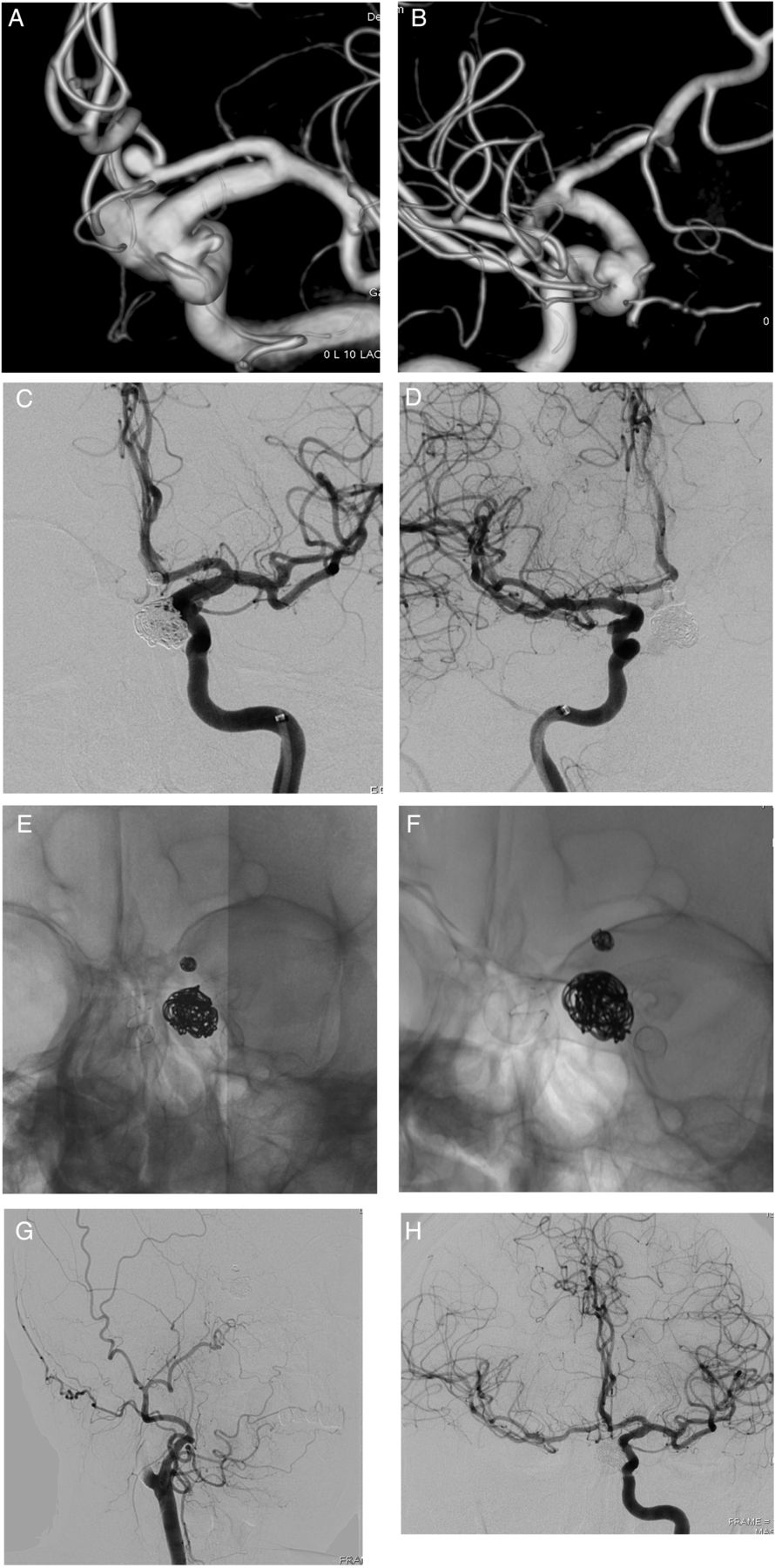
A 49-year-old woman presented with headache. (A, B) Three-dimensional reconstruction images show four aneurysms including anterior communicating artery (ACoA) and both right and left (2) paraclinoid internal carotid artery (ICA) aneurysms. (C, D) All detected aneurysms were treated in a single stage: ACoA aneurysm with single catheter coiling, two left ICA aneurysms with Pipeline Flex flow diverter stent (one with adjunctive endosaccular coiling), and right ICA aneurysm with Derivo flow diverter stent. (E) Complete opening of both flow diverter stents after treatment is shown. (F, G) Twelve days after treatment the patient had a transient ischemic attack and immediate control angiograms show delayed mechanical occlusion of the flow diverter at the proximal end which caused occlusion of the right ICA. (H) Three-month control angiogram shows stable occlusion of ACoA and left ICA aneurysms with patency of the flow diverter stent at the left ICA and right hemispheric collateral flow provided via the circle of Willis.
In the SAH group three patients had complications. One patient had parent artery occlusion 1 day after coiling of a left DACA aneurysm due to coil protrusion and was treated with tirofiban infusion and additional bailout stenting without any neurological deficit. However, in the other two patients, early aneurysm rebleeding and periprocedural spontaneous bleeding of the concomitant aneurysm resulted in death. In the first patient, after treatment of left M1 and DACA aneurysms with BAC, the patient had a puncture site hematoma followed by a sudden clinical deterioration at day 4. Rebleeding of the DACA aneurysm was seen on CT and digital subtraction angiography and platelet dysfunction was seen in laboratory tests. Despite endovascular retreatment the patient died several hours later. In the second patient with three aneurysms and diffuse SAH, it was decided to treat the more complex and bilobulated left MCA aneurysm initially as a result of inadequate identification of ruptured aneurysm. However, during treatment of the left MCA aneurysm, spontaneous concurrent acute bleeding was detected from the concomitant anterior communicating artery aneurysm which was then treated immediately. The remaining right posterior communicating artery aneurysm was left untreated due to the unstable clinical condition of the patient. However, the patient did not recover and died on day 4. Death was related to the gravity of SAH (Hunt and Hess grade IV–V) and cardiovascular and respiratory complications in three patients and refractory vasospasm in one patient. Symptomatic vasospasm requiring induced hypertensive and endovascular therapy including IA nimodipine and milrinone infusion and/or percutaneous transluminal angioplasty (PTA) was seen in nine patients. All these patients recovered without serious neurological deficit (mRS 0–2), except one in which refractory vasospasm resulted in death. Hydrocephalus requiring external ventricular drainage (EVD) and/or ventriculoperitoneal shunt (VPS) was seen in five patients.
Follow-up
Clinical follow-up and angiographic follow-up imaging was available in 44 patients (83%) for 104 aneurysms (83.2%) for a mean duration of 16.2 months (range 3–51 months). These patients had a favorable clinical outcome (mRS 0–2) at discharge and also at follow-up. In nine patients, 21 aneurysms did not have an angiographic follow-up because of death in eight and refusal in one patient. Occlusion grades and outcome of aneurysms on the basis of immediate post-treatment angiography and follow-up are summarized in table 3.
Immediate occlusion grades and follow-up results of aneurysms
According to the last angiographic follow-up data of the 104 aneurysms, overall occlusion rates were complete in 85 (81.7%), near complete in 8 (7.6%), and incomplete in 11 (10.5%) aneurysms.
Discussion
With the improvement in new endovascular techniques and devices, endovascular treatment has become a reasonable alternative for the treatment of intracranial aneurysms regardless of different locations and morphologies.6–13 Furthermore, recent studies have reported favorable mid- and long-term follow-up results of SAC, FDS, and intrasaccular flow modifiers in the treatment of intracranial aneurysms.26–28 However, in contrast to the high reported incidence of multiple aneurysms in up to 34% of patients,2 ,3 studies of the endovascular treatment of multiple aneurysms are limited and there are no data regarding the use of FDS, intrasaccular flow modifiers, or neck-bridging devices in the single-stage treatment of multiple aneurysms in existing studies, which are basically focused on coiling.14–18
Comparison with previous endovascular studies in terms of treatment techniques and complications
In one of the two recent studies with a large patient population, Jeon et al 17 treated 359 aneurysms in 167 patients with three types of combined coiling techniques. In 131 patients (78.4%), all detected aneurysms were treated with coiling only. The rate of any complication was reported as 6.6% (11/167), including thromboembolic complications, puncture site pseudoaneurysm, and ICA rupture. Treatment-related morbidity and mortality at discharge were reported as 1.8% and 0.6%, respectively. In the other study, Cho et al 18 treated 371 aneurysms in 172 patients in a single stage with different types of coiling techniques including multiple catheters, microcatheter protection, BAC, and SAC. Procedure-related adverse events were reported in eight patients (4.6%), including three instances of treatment failure, asymptomatic thrombi in four patients, and aneurysmal leakage in one patient. The procedural morbidity was reported as 0.6% and no procedure-related deaths occurred. In the current study the treatment rate of detected aneurysms (97.6%) is significantly higher than in the previous studies. This may be explained by the use of a combination of various endovascular techniques including SAC, FDS, intrasaccular flow modifiers and neck-bridging devices, which increases the possibility of treating all detected aneurysms including those with complex morphology. On the other hand, in the current study the overall complication and mortality rate was higher than in the previous studies.14–18 Our series consisted of mostly complicated and complex aneurysms that were difficult to treat with conventional simple coiling techniques and required more sophisticated modified procedures; most of the complications were not directly related to the single-stage treatment process. Furthermore, some of the complications were very uncommon—for example, delayed mechanical occlusion of the flow diverter which has not been previously reported in the literature. Complications resulting in death which was directly related to the single-stage treatment occurred in two patients, one from simultaneous stent thrombosis due to the discontinuation of antiplatelet therapy by the patient and the other from spontaneous concomitant aneurysm bleeding during treatment of a further aneurysm, which may be explained by the inadequate identification of a ruptured aneurysm.
Single-stage endovascular approach in SAH and during the period of vasospasm
Determination of ruptured aneurysms in patients with SAH is often difficult and misidentification of a ruptured aneurysm is not uncommon.29 In order to avoid the misidentified lesion being untreated, all detected and possibly ruptured aneurysms should be treated. A similar approach is acceptable for patients with unruptured multiple aneurysms in whom the risk of rupture is higher than for single aneurysms.30 Furthermore, it is not easy to estimate which aneurysm will rupture in the future. Single-stage surgery may be limited if the distribution of multiple aneurysms is bilateral or in both the anterior and posterior circulations.19 Surgical treatment may increase the risk of microinjury from arterial and brain tissue manipulation which results in poorer outcomes than in single aneurysms.4 ,19 Furthermore, in the acute stage of SAH, surgical access to multiple aneurysms is more difficult due to brain swelling and hydrocephalus in which the surgical space is reduced. Despite the technical difficulties of surgical clipping, endovascular treatment can be applied in a single session, as in the current study, regardless of the anatomic location of the aneurysms such as a combination of bilateral anterior and posterior circulation aneurysms that may not be clipped through a single craniotomy.
In patients with SAH, untreated aneurysms have a potential risk of rupture during treatment of vasospasm with aggressive hemodynamic augmentation or endovascular techniques.14 Single-stage treatment of all detected aneurysms theoretically minimizes the possible rupture risk of unsecured aneurysms during the aggressive treatment of vasospasm. In the current study, nine patients had symptomatic vasospasm requiring induced hypertensive and endovascular therapy. None of these patients had rebleeding during the treatment of vasospasm and all the patients recovered without serious neurological deficit, except one in whom refractory vasospasm resulted in death.
Technical concerns of single-stage treatment with SAC and FDS
Single-stage endovascular treatment has potential advantages if stent remodeling and/or FDS are the techniques used, in which dual antiplatelet therapy is mandatory. Securing all aneurysms theoretically decreases the fatal bleeding risk in case of rupture of unsecured aneurysms. Besides, the duration of antiplatelet therapy is reduced in single-stage treatment compared with staged procedures. On the other hand, the use of stents or FDS increases the risk of thromboembolic events. In particular, in patients with multiple aneurysms involving bilateral ICA, single-stage treatment with FDS carries the potential risk of simultaneous stent thrombosis which may cause morbidity and mortality by blocking the collateral pathways. In the current study, eight patients with bilateral ICA aneurysms were treated simultaneously with FDS in a single stage. Six patients had no adverse thromboembolic events in follow-up. However, one patient died because of bilateral stent occlusion due to the cessation of antiplatelet therapy by the patient and, in one patient, delayed mechanical stent occlusion caused the loss of the parent artery (figure 1). Staging of endovascular treatment in this group of patients may be a reasonable choice to avoid thromboembolic events, despite leaving an aneurysm unsecured under dual antiplatelet therapy.
Study limitations
This study has limitations due to its retrospective nature and lack of comparison of multimodality approaches combining surgery and endovascular treatment. Moreover, the use of different and combined endovascular techniques and varied grading scales in the same patient makes assessment of overall aneurysm occlusion rates and interstudy comparisons challenging. Furthermore, the variety and changes of technical equipment and devices during the study period might also have affected the angiographic and clinical outcomes. Even so, the results of this study may facilitate the choice of the most suitable treatment technique for patients with multiple aneurysms.
Conclusions
Our findings suggest that single-stage endovascular treatment of multiple intracranial aneurysms with a combination of different endovascular techniques is technically feasible with favorable initial and long-term occlusion grades and also increases the possibility of treating aneurysms with complex morphology. However, the safety of the single-stage treatment is controversial due to the relatively higher complication rates. Although the complications are not always directly related to the single-stage procedures, patient selection should be made cautiously and one should balance the advantages and disadvantages of the process. In particular, in patients with multiple aneurysms involving bilateral ICA, staged therapy could be used instead of simultaneous treatment with FDS to avoid thromboembolic events.
References
Footnotes
Contributors CA designed the study. CA, FA and OK collected the data and CA, MG performed the analysis. CA wrote the manuscript. CA and SA edited and reviewed the manuscript. CA is guarantor.
Competing interests None declared.
Patient consent consent forms were obtained from all patients or their relatives before the procedure.
Ethics approval This study was approved by Baskent University Instutional Review Board (Project no: KA16/98).
Provenance and peer review Not commissioned; externally peer reviewed.