Article Text

Abstract
Background Stentrievers have resulted in faster recanalization times in patients with acute ischemic stroke. Nonetheless, when strokes occur during evenings and weekends, delays are introduced in achieving this goal. We assessed the feasibility of achieving fast and successful endovascular reperfusion in patients with stroke treated during evenings and weekends and whether this has an impact on the outcome.
Methods A retrospective review was performed of a longitudinal database of patients with acute anterior ischemic stroke treated with endovascular therapy in a comprehensive stroke center between January 2011 and December 2012. The imaging to reperfusion time was defined as the time from completion of the unenhanced CT scan to the time of angiographic successful reperfusion (TICI 2b–3). This time interval was compared between patients treated during working hours (Monday to Friday 07:00–18:00 h) and those treated in the evening outside these hours and at weekends. The 24-h NIH Stroke Scale score and 90-day favorable outcome score (modified Rankin scale ≤2) were compared between the two groups.
Results In a cohort of 110 patients, 56 (50.9%) were treated on evenings and weekends. The median imaging to reperfusion time in these patients was 111 min compared with 90 min during working hours (p=0.019). The proportion of patients with successful reperfusion (TICI 2b or 3) during the evenings and weekends was 82.1% compared with 76.7% during working hours (p=0.4). The proportion of patients with a 90-day favorable outcome was not significantly different in the two groups (64.3% in those treated during evenings and weekends vs 52.1% in working hours, p=0.2).
Conclusions Some delays were encountered during evenings and weekend hours. Despite that, it was feasible to achieve a relatively short imaging to reperfusion times during these hours, in comparison to existing literature. A target universal time metric is needed to assess the timeliness of endovascular therapy in stroke centers.
- Thrombectomy
- Intervention
- Stroke
Statistics from Altmetric.com
Introduction
Timely reperfusion therapy with either intravenous fibrinolytic agents or mechanical thrombectomy is the key to improved stroke outcome.1 ,2 Thus far only intravenous tissue plasminogen activator (tPA) administered within 4.5 h of symptom onset has definitive supportive evidence for ameliorating functional recovery.3 Despite the current equipoise surrounding mechanical thrombectomy,4 there is undoubtedly a subset of patients with acute stroke in whom there is a benefit with early mechanical clot removal. This subset may be smaller than previously estimated and may require some effort to identify but, given the time-dependent nature of ischemic pathology, the time to intervention will play a critical role in the outcome.
The literature on intravenous tPA has demonstrated improved outcome with timely treatment.2 This has led to the introduction of the door-to-needle time as an important target in evaluating the quality of care in stroke centers. Several analyzes have reported inconsistent results regarding the effect of admission during evenings and weekends on treatment delays and outcomes. While recent data from the ‘Get With The Guidelines’ show slight delays in intravenous tPA administration in patients admitted during weekends with a small but significant increase in the odds of in-hospital mortality,5 others reported that admission during weekends in comprehensive stroke centers did not appear to affect the outcomes.6–9
The effects of interventions during evenings and weekends on the timeliness and outcomes of patients treated with endovascular therapies have not been well studied. While these effects have been reported in the literature on intravenous tPA, endovascular therapies are different in many aspects—for example, team members may not be not readily available or other services such as anesthesia may be required prior to the procedure. This study aims to explore the ‘weekend and non-working hour’ effect on workflow and outcome in endovascular stroke interventions.
Methods
An analysis of a prospectively maintained single-center longitudinal database of consecutive patients with acute anterior circulation ischemic stroke who were treated with endovascular therapy between January 2011 and December 2012 was performed.
Clinical data including demographics, history and baseline NIH Stroke Scale (NIHSS) scores were obtained by the treating stroke team members. All patients underwent an unenhanced CT scan of the head followed by CT angiography prior to treatment. Baseline and 24 h follow-up CT scans were scored using the Alberta Stroke Program Early CT Score (ASPECTS) by consensus of two stroke neurologists blinded to the patients’ clinical and angiographic outcomes. In addition, 24 h CT scans were scored for symptomatic intracranial hemorrhage (sICH) defined using the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) criteria.10
General anesthesia was rarely needed. Stentrievers were used as the sole modality in all patients. The endovascular procedure angiograms were scored using the Thrombolysis In Cerebral Infarction (TICI) score. Successful reperfusion was defined as a TICI score of ≥2b. The final reperfusion time was defined as the time of the angiographic run showing successful reperfusion after the stentriever was removed. The imaging to reperfusion time was defined as the time from completion of the unenhanced CT scan to the angiographic run showing successful reperfusion in the territory of the target occluded artery. The onset to reperfusion time was defined as the time interval from the witnessed symptoms onset (or last seen normal) to the time of successful angiographic reperfusion.
Clinical outcomes included the 24-h NIHSS scores and the 90-day functional recovery measured using the modified Rankin Scale (mRS). Favorable functional recovery was defined as an mRS score of ≤2.
Statistical analysis
Variables are summarized as median (IQR) or proportions as appropriate. The working hours were defined as Monday to Friday 07:00 to 18:00 while evenings and weekends encompassed all time periods outside these hours. The baseline and treatment variables were compared among the two groups. Continuous variables were compared using the Mann–Whitney U test and proportions were compared by the Fisher exact test. The primary objective of this study was to compare the imaging to reperfusion time between patients treated during the working hours with those treated on evenings and weekends. Secondary analyzes included comparing in-hospital mortality and favorable 90-day outcome between the two groups. All testing was two-tailed and done at the 0.05 level of significance. Analyzes were performed using Stata V.11 software (Stata Corp, College Station, Texas, USA).
Results
A total of 110 patients were analyzed. The median (IQR) age of the cohort was 68 (19) years and 44.9% were women. The median (IQR) baseline NIHSS score was 17 (9) and the median (IQR) baseline CT ASPECTS score was 8 (2).
Fifty-six patients (50.9%) were treated on evenings and weekends. Table 1 shows the characteristics of the two groups. Atrial fibrillation and current smoking were overrepresented in the patients presenting on evenings and weekends. There were no significant differences in the site of occlusion or the use of intravenous tPA in these patients. Successful reperfusion was achieved in 82.1% of patients treated during the evenings and weekends versus 75% in those treated during working hours (p=0.4). Intubation was required in 11% of those treated during weekends and evenings versus 15% in those treated during working hours (p=0.5).
Characteristics of the two treatment groups
Figure 1 shows the various treatment time intervals in the two groups. Delays were noted on evenings and weekends in the median imaging to puncture time (19 min difference in medians between the two groups, p=0.004) and imaging to reperfusion time (21 min difference in medians between the two groups, p=0.019). About 6.5% of patients treated during evenings and weekends achieved an imaging to reperfusion time of 60 min or less compared with 27.8% of those treated during working hours (p=0.005). There were no significant differences in the median door-to-reperfusion time (figure 1) or time of onset to reperfusion (264 min for evenings and weekends vs 262 min for working hours, p=0.9).

Treatment time intervals (min) in the two groups.
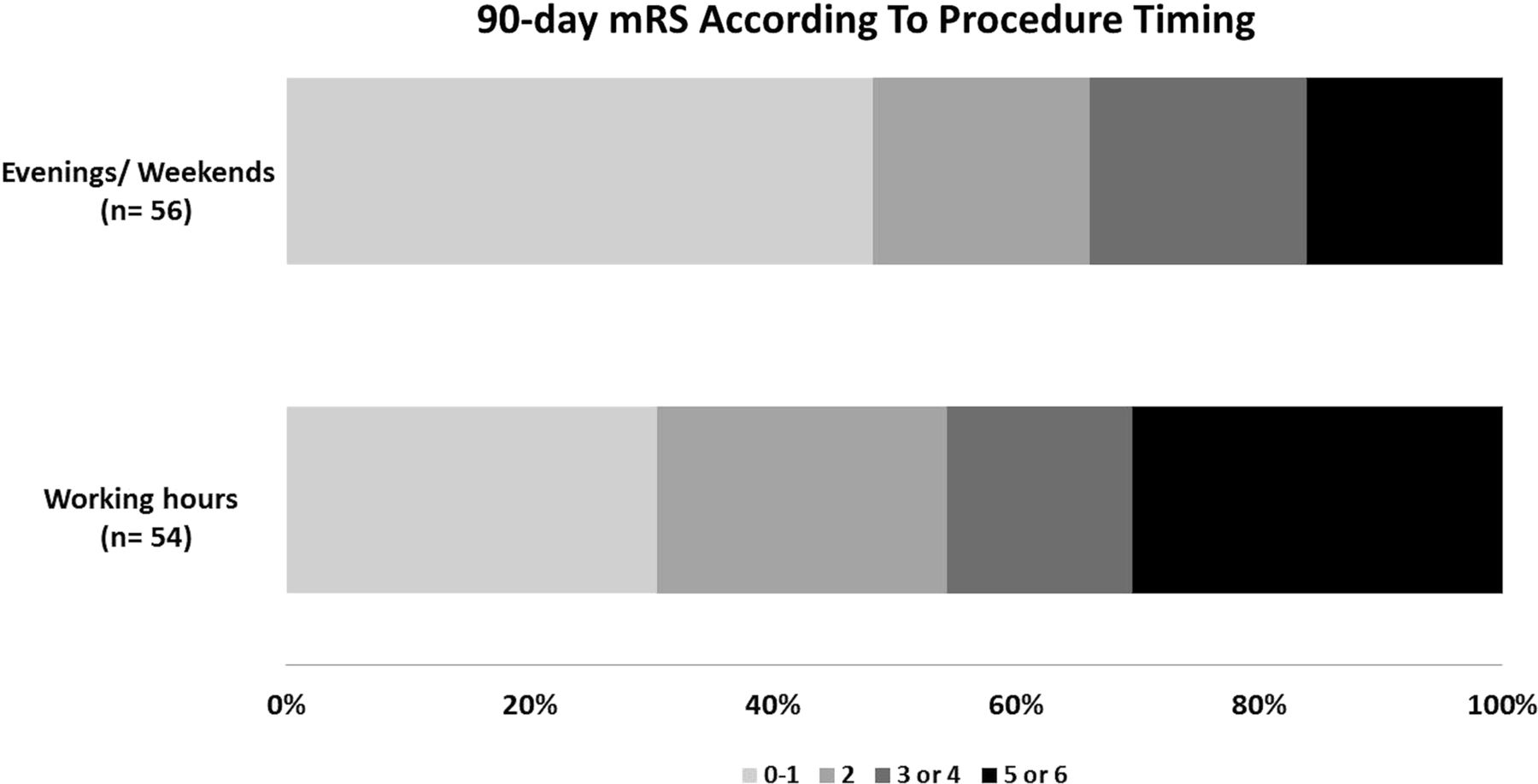
The median 24-h NIHSS score was 8 in those treated on evenings and weekends and 6 in those treated during working hours (p=0.7). There was no significant difference in the proportions of sICH (4% for weekends and evenings vs 9% for working hours; p=0.2) or in the in-hospital mortality (2% for those treated on weekends and evenings vs 5.6% for those treated during working hours; p=0.3). Independent functional recovery (mRS 0–2) at 90 days (figure 2) was noted in 64.3% of those treated on evenings or weekends and in 52.1% of those treated during working hours (p=0.2).

{kind=link}
{kind=link}
Distribution of functional outcomes using the 90-day modified Rankin Scale (mRS) in the two patient groups.
Discussion
There are multiple variables which factor into the outcome of any patient with stroke, many of which are beyond the control of the treating physicians. Time of symptom onset is one of these variables. Symptom detection and recognition, distance from emergency medical services (EMS) care, EMS triage ability, facility capabilities, time to CT scan, time to intravenous tPA, time required for transfer to comprehensive stroke center, speed of interventional procedure, patient anatomy and clot characteristics all combine into the time from symptom onset to reperfusion. However, once the patient enters the medical realm, it behoves the treating team to mitigate the detrimental effect of variables that are under their control.11 ,12
Our study shows that, in comprehensive stroke centers, delays can be minimized. It is feasible consistently to accomplish short times from imaging to successful endovascular reperfusion even during evenings and weekends. This fast reperfusion is expected to reflect favorably on patients’ outcomes.1 In the IMS III trial, the median time from CT to groin puncture was 119 min. Studies based on routine practice reported similarly long times from CT to groin puncture (1.7 h).13 Even high-volume centers (>50 endovascular stroke procedures per year) report a median CT acquisition to endovascular reperfusion time of 158 min.14 These figures point to the need for fundamental changes in the workflow of patients planned for endovascular stroke therapy.
Delays in achieving reperfusion are multifactorial. They can be attributed to the times required for the interventional team assembly, for obtaining consent for the procedure and for preparing the angiography catheters and devices. Once vascular access is obtained, reperfusion is usually achieved in a similar speed and success rate when stentrievers are used.15 Interventions that we found useful to minimize delays during these times include the presence of a stroke call team with 24-h/7-day coverage. Around-the-clock neurointerventional team coverage is essential. These elements help shape a consistent workflow that can be executed effectively regardless of the time of intervention. Our workflow depends on early notification of the endovascular team of all possible endovascular cases as patients are being transferred for imaging. An angiography tray is always ready to be used at all times and the same coaxial catheter set-up is used on all endovascular stroke cases. Finally, a continuous quality assurance process is in place to monitor and review the important interval milestones from the time patients with acute stroke arrive at the emergency door until successful endovascular reperfusion is achieved.
Controversy exists regarding the optimal time metric to assess the speed of endovascular stroke interventions.16 Unlike intravenous tPA where a door-to-needle time of <60 min is established as standard, endovascular studies continue to report multiple time metrics using different cut-offs. Some of these metrics capture various aspects of the workflow: the picture to puncture time estimates delays related to transport of patients from a distant hospital (where imaging was obtained) until the arterial puncture is obtained in the comprehensive stroke center.17 An imaging to recanalization time of ≤60 min was found to result in a limited infarct expansion on CT and a suggestion of better outcomes.18 A study conducted in three comprehensive stroke centers reported significant variability in the time from CT
scan acquisition to the time a microcatheter was positioned distal to the thrombus.19 This inconsistency in reporting makes it difficult to define a specific time metric that should be achieved. There is therefore an increasing demand for a consensus on a comprehensive time metric that captures potential delays in the in-hospital workflow of patients planned for endovascular interventions. The door-to-reperfusion time, akin to the door-to-balloon time in coronary literature, might become this benchmark metric but studies using individual patient level data from the published endovascular trials are needed to select the time cut-off that correlates with recovery. Once such a time metric is designated, studies reporting on time delays and tips to improve stroke workflow will be more relevant.20
This study has limitations that should be considered. This is a single-center study in which patients are selected for endovascular therapy based on the small core-proximal occlusion paradigm which may limit the generalizability of the results. There were some baseline differences between the study groups, with atrial fibrillation and smoking being more prevalent in the cohort treated during evenings and weekends. It is also expected that the two groups have other unknown clinical and pathophysiological differences. Whether these features contributed to different thrombus characteristics that made it more amenable to intravenous or endovascular therapies is unclear. Moreover, these differences are not expected to influence the treatment workflow. Although we observed no statistical difference in outcomes between the two groups, this might be attributed to the limited sample size. Finally, patients with posterior circulation stroke were not included in this analysis.
In conclusion, significant delays in the imaging to reperfusion times were encountered during evenings and weekends compared with working hours. Despite this, our reported imaging to reperfusion times remain relatively short compared with the existing literature. We hope that these findings will encourage future research on improving stroke workflow, especially in circumstances where delays are anticipated.
References
Footnotes
-
Contributors All authors contributed to the design, data collection, analyzes, interpretation, drafting or critical revision of this work.
-
Competing interests None.
-
Ethics approval Approval was obtained from the Conjoint Health Research Ethics Board at the University of Calgary prior to patient enrollment.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The principal investigator maintains full access to data.