Article Text

Abstract
Background Clot mechanical properties are influenced by composition and the arrangement of components within the clot. This work investigates the effects of platelet-driven contraction on blood clot microstructure and mechanical behavior, and provides insight into some implications for mechanical thrombectomy.
Methods Platelet-contracted clot analogues (PCCs) and non-contracted clot analogues (NCCs) were prepared from blood mixtures of various hematocrits (%H), that is, the volume percentage of red blood cells (RBCs) in the mixture. Mechanical testing was performed to compare the behavior of the analogues with previously tested human thromboemboli. Scanning electron microscopy and histology investigated the clot microstructure and composition. The association between clot properties and their behavior during mechanical behavior was also investigated.
Results Overall, PCCs were found to be stiffer than NCCs, across all hematocrits. PCCs with a low %H resisted complete ingestion via contact aspiration alone or complete retrieval with stent-retrievers. PCCs with a higher %H and all NCCs were fully retrievable, although the likelihood of fragmentation was increased in clots with a greater %H. Histologically, there was little difference in the RBC and fibrin content between PCCs and NCCs with the same %H. However, the microstructure of the two groups differed significantly.
Conclusion A selection of repeatable clot analogues with a range of mechanical properties have been developed for in vitro modeling of acute ischemic stroke. Platelet contraction significantly affects clot volume and microstructure, and in turn clot stiffness. The significant difference in mechanical properties and microstructure, but without an appreciable difference in histology, implies that histological studies of explanted human clots alone may not prove to be predictive of the mechanical behavior of the clots in thrombectomy.
- thrombectomy
- embolic
- device
Statistics from Altmetric.com
Introduction
Mechanical thrombectomy (MT) has recently been added to the standard of care for the treatment of acute ischemic stroke (AIS),1–3 where it greatly improves outcomes for eligible patients. MT procedures are significantly affected by the mechanical properties of the thrombus itself. Clinically relevant thrombus analogues provide a useful tool in the preclinical testing of thrombectomy devices to evaluate device design by measuring, among other things: the ability to capture and remove the occlusive thrombus, the number of attempts required, and the risk of procedure related embolism.4–8
Thrombus formation involves the inclusion of several components, mainly fibrin, red blood cells, platelets, and extracellular water.9 After solidification of the blood, platelet-driven clot contraction tightens the fibrin network by gathering fibrin strands to adhered platelets.10 The effect on the clot is a reduction of volume with expulsion of serum and a close packing of the blood components entrapped in the network. Thus, clot contraction acts to create an impermeable seal at the site of vessel injury. It has been found that the extent of clot contraction is sensitive to hematocrit—the volume percentage of red blood cells (RBCs) in the blood (%H),11 fibrinogen concentration and platelet function.
We previously described several clot analogues that can be used in the assessment of medical devices.4 Simulated thrombectomy procedures with such clots have effectively aided the evaluation of thrombectomy devices12 13; additionally, these clot analogues have been used for the assessment of specific clot attributes such as coefficient of friction,14 indentation/integration15 and appearance in medical imaging modes.16 Here we set out to report an expanded range of clot analogues, along with an analysis to advance the understanding of how platelet-driven contraction can affect the clot mechanical properties and microstructure and, in turn, how this can have implications for MT.
Materials and methods
Sample preparation
Fresh venous blood (Cummings School of Veterinary Medicine) was collected from the jugular vein of sheep. Ovine blood was chosen for the preparation of the clot samples as it has been found to be a suitable substitute for human blood for coagulation studies,17 and the clot samples produced using this methodology have been found to be histologically similar to human clots.4 Blood was collected in receiving vessels pre-loaded with ACPD (adenine citrate phosphate dextrose) anticoagulant solution. The blood was then transported to the laboratory and stored at room temperature until used. All clots were prepared within 5 hours of blood collection.
The blood was first centrifuged at 180 g for 10 min to isolate the top layer of platelet-rich plasma (PRP). The remaining blood mixture was centrifuged again at 2200 g for 10 min to collect platelet-poor plasma (PPP). The buffy layer was removed as waste to isolate the RBCs beneath.
Two families of clot analogues were produced: platelet-contracted clots (PCC), and non-contracted clots (NCC). PCCs were formed from blood mixtures with different hematocrit (%H), that is, the volume percentage of RBCs in the mixture, by mixing RBCs with PRP in controlled ratios. The same procedure was followed for the NCCs; however, instead PPP was mixed with RBCs in the same controlled ratios.
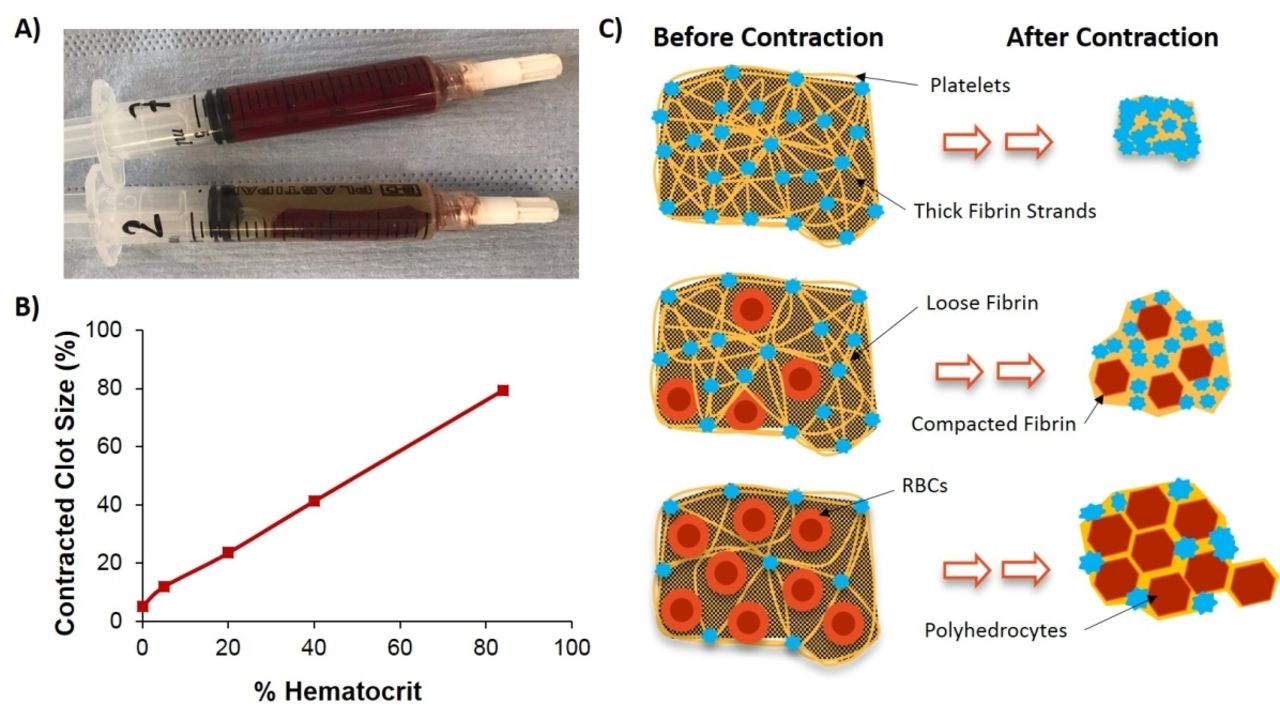
Coagulation of the blood mixtures was initiated by adding 2.06% calcium chloride solution in a 1:9 ratio. The samples were formed in cylindrical-shaped molds (figure 1A) and were placed standing vertically to mature overnight at 37°C. The extent of contraction was assessed gravimetrically by weighing the solid and liquid phases in the clot molds separately. The color of the serum was monitored to ensure the RBCs had been incorporated.

(A) Non-contracted clot (NCC) (top) and a platelet-contracted clot (PCC) with expelled serum (bottom). (B) Plot of contracted clot size (expressed as a % of the original weight of blood mixture before clotting) versus hematocrit of the blood mixture. (C) Schematic diagram depicting clot contraction and how it is limited by the red blood cells (RBCs) present. Before contraction the clots consist of a loose fibrin mesh (yellow) with RBCs (red) scattered throughout and platelets (blue) attached at junctions of thicker fibrin fibers. After contraction the fibrin compacts around polyhedron-shaped RBCs (polyhedrocytes) and serum is expelled, resulting in reduced clot volume.
Mechanical characterization
Compression testing was selected for this study as this method is sufficiently robust to allow reliable testing of a broad range of clot types, and it allowed the authors to compare the mechanical behavior of the presented clot analogues with that of previously tested human AIS samples. Tensile testing of the samples was initially attempted; however, reliable tensile testing did not prove possible and often resulted in tearing/rupturing at the grips due to the fragile nature of the clots.
A Dynamic Mechanical Analyzer (DMA, Q800; TA Instruments, New Castle, Delaware) was used to investigate the mechanical behavior of the clot analogues. The test was carried out using a submersion compression clamp in the controlled force mode and the samples (minimum of n=3 for each group) were tested in a 0.9% saline solution (Baxter Healthcare SA, Zurich, Switzerland) at 37°C. Cylindrical clot samples, with a diameter of approximately 5 mm, were cut to have an approximate height of 3 mm, as in the study by Chueh et al.5 The samples were placed in saline for 30 min before testing; 220-grit sandpaper was adhered to the compression disk to prevent the samples from slipping out during the test. The test consisted of a force ramp to 15 N at a rate of 0.5 N/min, according to Chueh et al,5 in compression.
To compare the mechanical behavior of the materials, tangent stiffnesses were determined from the slopes of straight lines fitted to the initial and final linear portions of the nominal stress-strain curves: a low strain tangent stiffness (over approximately initial 10% strain), and a large strain tangent stiffness (over approximately the final 2% strain). It is worth noting that these quantities were dependent on the specific test conditions and were used here as a convenient measure to compare mechanical performance. True stress-strain curves could not be generated for these tests as there was no reliable measurements for contact area due to the nature of the test set-up.
An additional indicator of the mechanical behavior is the onset point,5 which was obtained as the intersection point of the aforementioned two lines. Statistical analysis was carried out using the general linear model ANOVA (analysis of variance) procedure in Minitab (version 18.1). A comparison of mean onset point was performed with a Bonferroni model (α=0.05) to compare the onset point of the clot analogues with the human thromboemboli tested by Chueh et al.5
Histology
MSB staining was selected to stain for fibrin and erythrocytes.4 5 Sections of the clots were fixed in a 10% buffered formalin solution for 48 hours, embedded in a paraffin wax and cut into 5 µm sections. The sections were then dewaxed and hydrated with distilled water in preparation for staining.
Sections were photographed using an Olympus vs120 digital slide scanner. The objective lens, brightness, and height of the condenser, as well as the saturation, brightness, and contrast settings of the image acquisition software, were standardized to ensure uniformity of the digitized images. Images were acquired at 40× magnification from five randomly chosen areas of the slide. The quantification method followed was previously reported to assess the composition of human thrombi18 and clot analogues.4 ImageJ was used for quantitative analysis of the percentage fibrin and RBCs by area.
Scanning electron microscopy (SEM)
Samples were fixed with 2.5% glutaraldehyde and dehydrated in a series of ethanol concentrations up to 100%. The samples were frozen in liquid nitrogen and fractured to examine the interior surface of the clot analogues. The samples were then critical-point dried, mounted and sputter-coated with iridium.
In vitro model of AIS and thrombectomy
An in vitro model based on the human intracranial circulation was used for observational thrombectomy experiments (image of model provided in online supplementary file 1). The model consisted of the complete intracranial circulation with both carotids and vertebral arteries, complete circle of Willis, and functional anterior and posterior communicating arteries with distal circulation up to M2 and A2 (Elastrat Sàrl, Geneva, Switzerland).19
Supplemental material
Saline at 37°C was circulated through the model and the rate of flow was set to be within the range of clinically representative flow rates. To consistently target the same region of the anatomy, both PCCs and NCCs were cut to have dimensions of 3 mm×3 mm×8 mm, introduced into the model and allowed to migrate in the vessel to the target location to facilitate a distal M1 segment occlusion of the middle cerebral artery. Clots that did not reach the M1, or migrated too far distally, were discarded and replaced with a new clot to ensure consistent clot location for each procedure.
Two retrieval techniques were used to remove the clot analogues: contact aspiration with an aspiration catheter, and retrieval via stent-retriever combined with local aspiration into an intermediate catheter. An ACE 64 (Penumbra, Alameda, CA, USA) intermediate catheter was used for the former, and a 33×5 mm Embotrap II stent-retriever (Cerenovus, Galway, Ireland) and an ACE 64 intermediate catheter were used for the latter. A Medium Support 0.014 inch straight tip guidewire (Boston Scientific, Marlborough, USA) and an ev3 Rebar (ev3, Irvine, CA, USA) 0.021 inch microcatheter were used to cross the clot for the retrievals using the stent-retriever. For contact aspiration alone, the catheter was advanced to the face of the clot over the guidewire and aspiration was applied using a Hersill V7 Plus AC aspiration pump (Hersill Medical Devices, Madrid, Spain), which was set to “high”. The interaction of the clot with the devices was investigated by observing the behavior of the clot and device during retrieval. All of the clots were successfully retrieved after one pass.
Results
Gravimetric analysis of clots
For all clots, in the early stage following clotting initiation (within 30 min) the entire blood mixture was solidified into a clot. When subsequent clot contraction occurred, the extent of clot contraction was calculated by weighing the combined serum and clot together and the resultant clots alone using a gravimetric balance. Mass reduction due to contraction was calculated by expressing the weight of the clot as a percentage of the weight of the clot and serum together. No serum was expelled from the NCCs, indicating that there was no mass loss due to contraction. However, PCCs had a reduced weight due to expulsion of serum. The eventual size of the PCCs strongly correlated (R2=0.99) to the %H of the clot mixture (figure 1B). An additional gravimetric assessment of the NCCs was carried out whereby the NCCs were mechanically compressed by spinning twice in a centrifuge for 10 min at 2200 g. The final weight of these mechanically contracted clots also correlated to the %H of the blood mixtures (data provided in online supplementary file 2), thereby demonstrating that RBCs, entrapped in the clot network, were a limiting factor for the final clot volume.
Supplemental material
Mechanical behavior of clot analogues
The mechanical testing showed that all clots exhibited non-linear stress-strain behavior (figure 2A). PCCs had earlier onset points than NCCs (figure 2B), meaning that as they deformed under an applied force, they reached the point where they greatly resisted further deformation sooner (eg, the second linear part of the curves shown in figure 2A). The 20% H PCC was found to have the earliest onset point, stiffening sooner than the rest of the analogues. A non-linear dependence on hematocrit was observed.
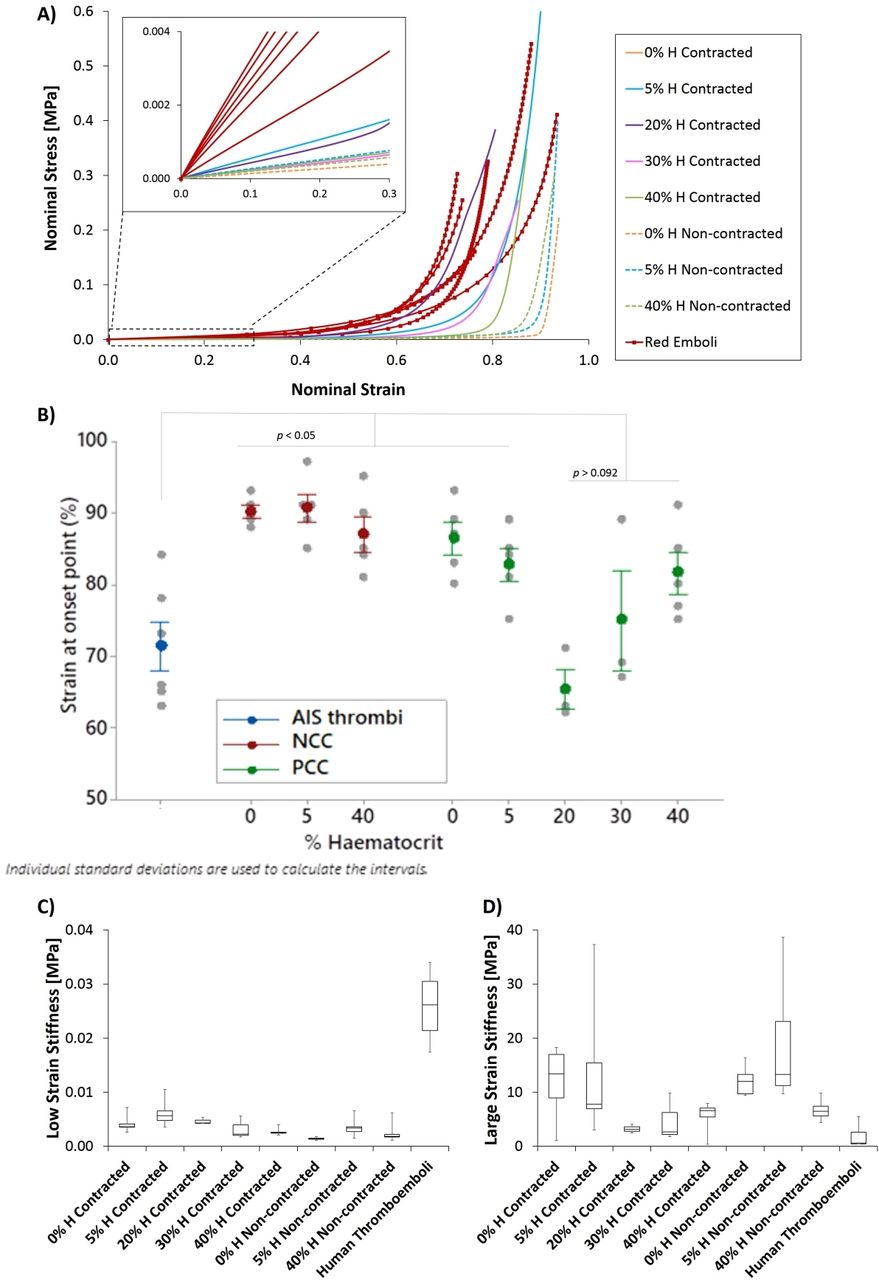
(A) Average nominal stress-strain curves for the compression testing, shown as positive values for clarity, comparing the mechanical behavior of the platelet-contracted clots (PCCs) and non-contracted clots (NCCs), with the raw data for the human red thromboemboli previously tested by Chueh et al.2 Inset shows a zoomed-in image of the behavior at low levels of strain. (B) Plot of onset point versus hematocrit, comparing the onset point of both the PCCs and the NCCs with the human thromboemboli. (C) Comparison of low strain stiffness and (D) stiffness at large strain for the PCCs and NCCs with the human thromboemboli. AIS, acute ischaemic stroke; H, hematocrit.
The mechanical behavior of the clot analogues was compared with thromboemboli tested by Chueh et al (Figure 2A–B). Both groups of analogues were found to have lower stiffnesses than the human thromboemboli at low levels of strain (<30%) (figure 2C), by almost an order of magnitude. However, all of the clot analogues were found to reach similar stiffness levels at high strain levels (figure 2D) and to span the range of large strain stiffnesses measured in the ex vivo emboli.
Composition and structure of clot analogues
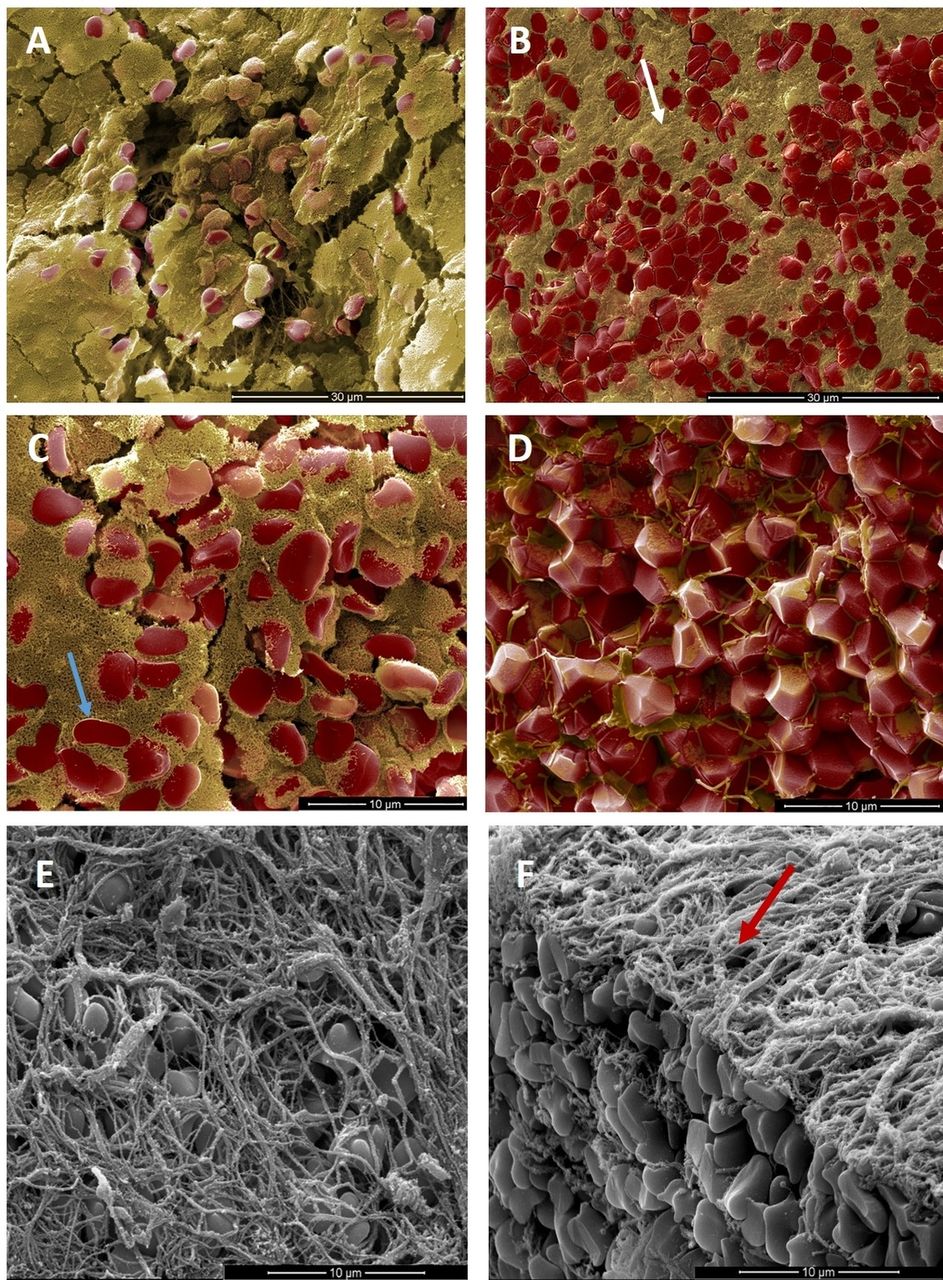
Histological examination of the clot analogues showed little difference in the fibrin and RBC content when comparing the PCCs and NCCs at the same hematocrit levels (figure 3). However, under SEM the microstructure of both groups were significantly different (figure 4A–D). Two types of fibrin fibers were observed, thick fibers (179.8±80 nm) with relatively few branches, and thin hyper-branched fibers (45.75 ±11.5 nm).20 The former was observed in abundance on the exterior of the clots and traversing the interior, while the latter was seen in the interior only. In the NCCs, the thin, highly branched fibrin occupied the spaces between the RBCs and thicker fibrin fibers (figure 4A and C). This spongy fibrin network was significantly compressed through the action of clot contraction (figure 4B and D), appearing as a thin layer on the faces of closely packed RBCs (figure 4D).

MSB staining of (A) 0% hematocrit (H) clot, (B) 5% H clot and (C) 40% H, showing fibrin (pink) and red blood cells (RBCs) (yellow). (D) Bar graph comparing the % of fibrin and RBCs in both platelet-contracted and non-contracted clots across three hematocrits.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Coloured scanning electron microscope images, showing fibrin in yellow and red blood cells (RBCs) in red, of the interior of (A) a 5% hematocrit (H) non-contracted clot (NCC) and (B) a 5% H platelet-contracted clot (PCC), with the white arrow indicating compressed fibrin. (C) Interior of a 40% H NCC, with the blue arrow highlighting a typical biconcave-shaped RBC trapped within a loose fibrin mesh. (D) Polyhedrocytes present in the interior of a 40% H PCC. (E) Large fibrin strands covering the exterior surface of the clot analogues. (F) Interior and exterior surfaces of the clot, with the red arrow indicating the outer surface.
Noticeable changes in RBC shape were also apparent. The typical biconcave-shaped RBCs were clearly observed in the NCCs, whereas the PCCs consisted of compressed fibrin structures, compacted around polyhedron-shaped RBCs, called ‘polyhedrocytes’.21 The thicker fibrin was seen to entrap the polyhedrocytes in a latticework of fibers. Imprints by the thick fibrin fibers were visible on the face of the RBCs, thus establishing that contractile forces exerted by platelets, and conveyed through the fibrin fibers, were responsible for the RBC shape change.
All of the clot analogues were found to have a fibrous layer containing thicker fibrin fibers covering the exterior of the clot (figure 4E & F). In PCCs, a higher concentration of platelets was also visible on the outside of the clot when compared with the interior.
In vitro retrieval of clot analogues
MT was simulated in an in vitro flow model using two approaches: (1) contact aspiration with an aspiration catheter; and (2) retrieval via stent-retriever combined with local aspiration into an intermediate catheter (IC). For the aspiration only technique, it was not possible to fully aspirate PCCs formed with 0% H or 5% H into the aspiration catheter; however, the clots were subsequently successfully retrieved by removing the catheter and clot en-bloc. NCCs were successfully aspirated fully through the aspiration catheter. The results from the combined approach were similar. The lower hematocrit PCCs were not fully retrieved into the IC using the stent-retriever, requiring en-bloc removal of the clot with the stent-retriever and IC.
NCCs and PCCs formed from blood mixtures with a higher hematocrit were fully retrieved into the IC, either with aspiration alone or through use of a stent-retriever. However, considerably more fragmentation was observed for the 40% H PCC compared with the 40% H NCC as they entered the IC using both techniques.
Discussion
This investigation has shown that the mechanical properties of clot analogues can be significantly altered by the activation of platelets during clotting and also by varying the hematocrit. The extent of clot contraction was found to be hematocrit-dependent, as clots formed from blood mixtures with a lower hematocrit contracted more than clots with a greater hematocrit. This is due to the incompressible RBCs present.
The clot analogues were found to have a similar, non-linear stress-strain relationship and mechanical behaviour to published data for clot material.5 7 8 22 The NCCs were found to be less stiff than the PCCs across all hematocrits. Of the PCCs, the 40% H clot had the lowest low strain stiffness. This is likely due to the lower levels of fibrin present to reinforce the matrix, combined with the increased number of RBCs present, reducing the overall stiffness. However, the clots formed from 20% H blood had a greater compressive stiffness than 0% H and 5% H clots. It is hypothesised that the ratio of fibrin to RBCs in the fibrin matrix is optimal in clots within this range of hematocrit, and the stiffness is increased potentially due to a reinforcement effect of the RBCs within the fibrin matrix. However, further testing with a larger sample size is necessary to confirm this result.
The large strain stiffnesses of the analogues were found to span the range measured for the human thromboemboli at large strains. Since MT causes large strain in the clot material, it is considered that clot behaviour at these strains (<60%) is of most interest when comparing the analogues with the thromboemboli.
Platelet contraction had the effect of increasing stiffness and, together with adjustment of the hematocrit, enables close matching of stiffness to representative thromboemboli of AIS origin. The lower stiffness of the NCCs is unsurprising considering the large volume of extracellular water (serum) in these clots. However the behaviour of the NCCs is also relevant as patients of AIS may exhibit impaired platelet function, and therefore there is a mechanism by which NCC clots can arise in vivo.23
Contracting platelets actively remodel the fibrin network by tightening the fibers, and therefore the enhanced stiffness of the PCCs can be explained by examining their microstructure. The NCCs were found to consist of a loose fibrin mesh with biconcave-shaped RBCs homogeneously dispersed throughout, whereas the PCCs consisted of compacted fibrin around polyhedrocyte-shaped RBCs. The loose fibrin mesh in PCCs can be easily deformed under compression, thus resulting in lower clot stiffness.
Polyhedrocytes have been observed in human coronary thrombi21; it is hypothesized that this shape allows for more efficient packing of RBCs,11 thus creating an impermeable seal at the site of vessel injury to prevent bleeding.10 This decreased permeability may impact the effectiveness of medical thrombolytic therapy in AIS. In vitro thrombectomy experiments reported in this study show that clot engagement with devices differed for PCCs and NCCs, with PCCs having fewer RBCs incorporated resisting full ingestion or retrieval into catheters. PCCs with a greater hematocrit appeared to be more prone to fragmentation than their NCC counterparts.
Clot composition has been assessed ex vivo4 5 24 to determine a potential relationship between thrombus histology and difficulty of clot removal. Many medical imaging studies attempting to determine the difficulty of clot removal based on predicting the composition of clots using CT or MRI have also been carried out.18 25–27 However, the quantitative histological measurement of RBC and fibrin composition in this study failed to distinguish clots based on their mechanical properties. SEM analysis of the clot microstructure clearly highlighted how clots formed from blood solutions with the same hematocrit could illicit varied mechanical behaviour. Taken together, the significant difference in mechanical properties and microstructure, but without an appreciable difference in RBC and fibrin composition, implies that histological examination of the fibrin and RBC content of explanted human clots alone should not be used in isolation as a predictor of the mechanical behaviour of the clots in thrombectomy.
A limitation of this study was the homogeneous nature of the clots, as they were prepared under static conditions in a controlled laboratory environment, whereas clots retrieved from patients tend to have irregular distribution of components. However, for the purposes of understanding the mechanical behaviour of clots it was necessary to use homogeneous samples. Nevertheless, it should be noted that clots in vivo may be heterogeneous.
There are few studies that have investigated the mechanical properties of human thromboemboli; therefore, there are limited data with which to compare our clot analogues. In this study, we compared the mechanical behaviour to one classification of thromboemboli that were retrieved from patients with AIS via aspiration.5 However, these ex vivo clots may have already experienced severe deformation during aspiration and therefore there is the possibility that their mechanical properties were altered before testing.
Conclusion
This study outlines the preparation and characterization of both PCC and NCC analogues with varying hematocrits and demonstrates the effect of clot contraction on the microstructure and mechanical behaviour of the material. Although significant differences in mechanical properties and microstructure were observed between PCCs and NCCs, histological quantification of fibrin and RBCs in these clots did not show an appreciable difference. The implication is that RBC content alone, measured by histology, of explanted human clots may not be predictive of their mechanical behaviour during thrombectomy.
As clot contraction can also affect the clot permeability, it is hypothesized that this may have an impact on the effectiveness of stroke treatments such as thrombolysis and MT. The clot analogues presented in this paper have been shown to be useful for the evaluation of different clot behaviour during mechanical thrombectomy.
Acknowledgments
The authors would like to acknowledge the support of the New England Center for Stroke Research Lab (NECStR) at the University of Massachusetts for their assistance with this study.
References
Footnotes
PEM and MG are joint senior authors.
Contributors SJ: clot preparation, study design, data collection, data analysis and interpretation, manuscript writing and editing. JC and MJG: experimental conception and design. RMC: clot preparation, study design, data interpretation, manuscript editing. PEM, JPM: interpretation of the results, manuscript editing. MG: initial concept of forming clot analogues, manuscript editing. All authors provided suggestions and feedback on the manuscript, and approved the final manuscript.
Funding This work was supported by Cerenovus, the Irish Research Council (Grant No. EPSPG/2015/92) and the NUI Galway Hardiman Research Scholarship.
Competing interests SJ reports grants from the Irish Research Council and the NUI Galway Hardiman Research Scholarship during the conduct of the study, and reports financial support from Cerenovus, outside the submitted work. RMC, MG report a financial relationship with Cerenovus outside the submitted work. JPM reports non-financial support from Cerenovus, outside the submitted work. JC reports fee-for-service consulting for Stryker Neurovascular and InNeuroCo Inc. MJG has been a consultant on a fee-per-hour basis for Cerenovus, Imperative Care, MIVI Neurosciences, phenox, Route 92 Medical, Stryker Neurovascular; holds stock in Imperative Care and Neurogami; and has received research support from the National Institutes of Health (NIH), the United States – Israel Binational Science Foundation, Anaconda, Cerenovus, Cook Medical, Gentuity, Imperative Care, InNeuroCo, Magneto, Microvention, Medtronic Neurovascular, MIVI Neurosciences, Neuravi, Neurogami, Philips Healthcare, Rapid Medical, Route 92 Medical, Stryker Neurovascular, Syntheon, and the Wyss Institute.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Please contact the corresponding author with data sharing requests.