Article Text

Abstract
Background Although it is common practice to wait for an ‘embedding time’ during mechanical thrombectomy (MT) to allow strut integration of a stentriever device into an occluding thromboembolic clot, there is a scarcity of evidence demonstrating the value or optimal timing for the wide range of thrombus compositions. This work characterizes the behavior of clot analogs of varying fibrin and cellular compositions subject to indentation forces and embedding times representative of those imparted by a stentriever during MT. The purpose of this study is to quantify the effect of thrombus composition on device strut embedding, and to examine the precise nature of clot integration into a stentriever device at a microstructural level.
Method Clot analogs with 0% (varying densities), 5%, 40%, and 80% red blood cell (RBC) content were created using ovine blood. Clot indentation behavior during an initial load application (loading phase) followed by a 5-min embedding time (creep phase) was analyzed using a mechanical tester under physiologically relevant conditions. The mechanism of strut integration was examined using micro-computed tomography (µCT) with an EmboTrap MT device (Cerenovus, Galway, Ireland) deployed in each clot type. Microstructural clot characteristics were identified using scanning electron microscopy (SEM).
Results Compressive clot stiffness measured during the initial loading phase was shown to be lowest in RBC-rich clots, with a corresponding greatest maximum indentation depth. Meanwhile, additional depth achieved during the simulated embedding time was most pronounced in fibrin-rich clots. SEM imaging identified variations in microstructural mechanisms (fibrin stretching vs rupturing) which was dependent on fibrin:cellular content, while µCT analysis demonstrated the mechanism of strut integration was predominantly the formation of surface undulations rather than clot penetration.
Conclusions Disparities in indentation behavior between clot analogs were attributed to varying microstructural features induced by the cellular:fibrin content. Greater indentation was identified in clots with higher RBC content, but with an increased level of fibrin rupture, suggesting an increased propensity for fragmentation. Additional embedding time improves strut integration, especially in fibrin-rich clots, through the mechanism of fibrin stretching with the majority of additional integration occurring after 3 mins. The level of thrombus incorporation into the EmboTrap MT device (Cerenovus, Galway, Ireland) was primarily influenced by the stentriever design, with increased integration in regions of open architecture.
- stroke
- thrombectomy
- device
- intervention
- stent
Statistics from Altmetric.com
Introduction
Acute ischemic stroke (AIS) is caused by thromboembolic occlusion of a cerebral artery resulting in the restriction of blood flow with corresponding loss of neurologic function. Recanalization strategies, including intra-venous tissue plasminogen activator (tPA) and intra-arterial approaches, attempt to re-establish blood flow to ischemic regions of the brain caused by AIS. Mechanical thrombectomy (MT), using a ‘stentriever’ device, is emerging as a promising intra-arterial recanalization strategy for AIS treatment.1–5 MT is a minimally invasive surgical procedure which exploits self-expanding stent-like technology for effective thromboembolic clot removal with immediate recanalization. During MT, a self-expanding device is deployed within an occluded cerebral artery at the site of the thrombus. As the stentriever expands, device struts subsequently embed into the clot during an ‘embedding time’, typically 5 mins, to allow the offending thrombus to become further integrated into the stentriever device. Finally, the device and thrombus are withdrawn into a guide or intermediate catheter and removed from the body. Successful recanalization of the vessel depends, in part, on how effectively the thrombus is incorporated into the device. Therefore, studying the device-clot interaction may offer insights into how to improve MT success.
Thromboembolic clots consist of a three-dimensional network of taut branched fibers in a cellular matrix containing platelets, white and red blood cells (RBC).6 Clot analogs, produced in the laboratory are typically used for in vitro evaluation of MT device performance. It is imperative that such clot analogs are representative of human thrombi. However, extensive varieties in composition are found in human AIS thrombi, from RBC-rich to fibrin-rich clot configurations, resulting in differing mechanical behaviors.6–11 In addition, the work of Chueh et al suggests common variables associated with the production of clot analogs affect their behavior such as the concentration of thrombin and radiopaque additive such as barium sulphate.12 They report the addition of thrombin results in an increased clot stiffness, while the presence of barium sulfate significantly reduces stiffness. Meanwhile, the computational work of Kim et al investigates the correlation between a clot’s structural features and its behavior: mechanical properties of clot analogs were assessed by analyzing the fibrin network response to uniaxial tensile and shear stresses.13 Validating their computational model against the experimental work of Ryan et al,14 they conclude the average stiffness of a fibrin-rich clot analog was approximately 2.6 times larger than a RBC-rich clot analog.
In a similar study, analyzing the effect of fibrin:RBC ratio on clot behavior, it was confirmed that a clot becomes less organized, less stiff, and more viscoelastic with increasing RBC content.15 It was concluded that the addition of RBCs leads to the formation of thicker fibrin fibers which, in turn, affects the fundamental properties of the clot. In a study of the frictional properties of clot analogs of varying composition, it was shown that higher friction is associated with clots of higher fibrin:RBC ratio (especially <20% RBCs) which is suggested to correspondingly affect retrieval success during MT.16 In a systematic experimental study, eight extracranial arteries in swine were occluded with RBC-rich clots while a further eight were occluded with fibrin-rich clots. It was found that arteries occluded by fibrin-rich clots demonstrated a significantly lower recanalization rate (37.5% vs 100%), a longer mean recanalization time (81.5 mins vs 15.5 mins), and a higher number of MT attempts (4.5 vs 2.75) than arteries occluded by RBC-rich clots.17 Overall, reported deviations in MT device performance can be attributed to differences in clot physical properties: these differences can be explained by the changes in microstructural fibrin and cellular variances across clot types.
Research primarily focusing on device-clot interaction remains scarce in the literature. One of the few studies on this phenomenon tested a Solitaire MT device (Medtronic, Irvine, CA, USA) in 15 swine vessel occlusions, and reported that a selected embedding time of 10 mins resulted in a gradual indentation of the clot by the stentriever struts.18 However, the probability of achieving a statistically significant recanalization improvement in the vessel peaked at an embedding time of 5 mins. The apparent advantage in waiting for an embedding time has since been confirmed using conventional angiography19 and CT imaging.20 With the exception of studies such as those completed using nanoindentation on murine thrombi to establish local small-strain elastic modulus,21 22 to the authors' knowledge no published work to date uses indentation techniques to evaluate strut-clot interaction for MT device evaluation. The current work aims to characterize the indentation behavior of five clot analogs of varying fibrin and cellular configurations subjected to indentation forces and embedding times representative of those experienced during MT. This novel testing will expand current knowledge on the effect of clot composition on MT device performance, and in particular on the precise device-clot interaction behavior of the EmboTrap MT device (Cerenovus, Galway, Ireland).
Materials and methods
Clot preparation
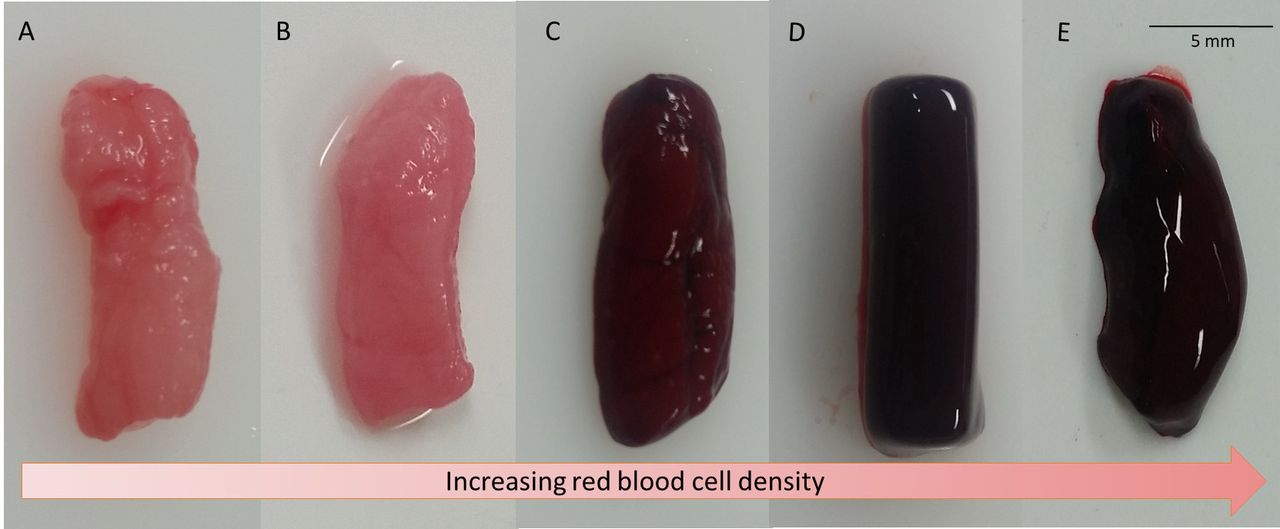
Venous whole blood was obtained by a qualified veterinary surgeon (Ash Stream Vets, Co. Mayo, Ireland) from both male and female ovine specimens, aged between 1–7 years and weighing 70–120 kg. Ovine blood was selected for clot analog production as it has been shown to be the most suitable for coagulation studies.23 Five clot analog types were produced (figure 1A–E) using the methodology outlined previously by Duffy et al.24 Immediately following collection, the whole blood was anti-coagulated in 3.2% sodium citrate solution in a 9:1 ratio (all mixing ratios were measured per volume). Centrifugation was performed at 550 g for 15 mins to separate the whole blood constituents into three distinct layers, namely, the plasma, buffy coat, and RBC layers for extraction to allow selected clot production. Clot types shown in figure 1A–B consist of a 0% RBC content by volume, i.e. containing 100% plasma. The clot analog of figure 1A, 0% RBC ‘high density’, underwent subsequent dehydration to 5% of its initial mass to produce a more densely packed fibrin network clot that is representative of a more organized mature clot. The clot analog of figure 1B, 0% RBC ‘low density’, was retained at its original mass. Clot types shown in figure 1C–E, containing 5, 40, and 80% RBC by volume respectively, represent the wide range of RBC composition reported in the literature of human thrombi.6–11 Coagulation was initiated through the introduction of 2.06% calcium chloride solution to the blood components in a 1:9 ratio. Clotted material was incubated for 30 mins in a water bath held at 37°C. Final clot test samples for indentation testing had an overall approximate size of Ø5×10 mm, which is within the range of the average size of retrieved human thrombi.25
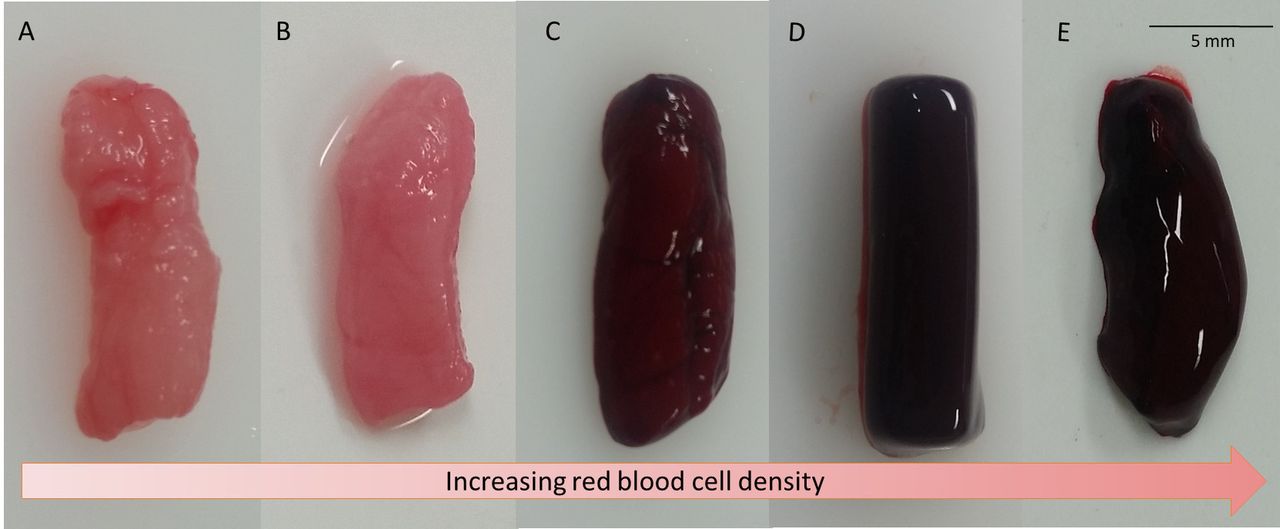
Clot analog test samples produced in this study, namely, (A) 0% RBC high-density (B) 0% RBC low-density (C) 5% RBC (D) 40% RBC, and (E) 80% RBC clot types.
Clot indentation test method
To simulate the force imposed by a stentriever strut on an occluding clot during MT, indentation testing was conducted using a Zwick universal tester in compression mode. Ten replicate clot samples were tested for each of the five clot analog types (total sample number, n=50): clots were cut to have cylindrical dimensions of Ø5×10 mm. The indenter tip was designed to approximate the profile of a single strut of a MT stentriever device, with a rectangular surface of 3 mm x 0.075 mm contacting the clot. The indenter was securely clamped in upper grips, while the clot was inserted into a custom-designed clot containment chamber secured on a flat surface at the base of the equipment. The clot containment chamber consists of a cylindrical lumen (I.D. 5 mm) and an upper steel plate containing a central slot (5×2 mm) through which the indenter could pass vertically with clearance (as shown in figure 2A). This configuration mimics a stentriever strut approaching an occluding clot during the deployment stage of a MT procedure following appropriate device placement using a microcatheter. A syringe was aligned horizontally with the proximal edge of the clot and a constant pressure of 90 mmHg was applied to simulate the average blood pressure acting on the clot (figure 2A). The force imposed on a clot by a single strut will vary depending on the MT device used. For the purpose of this experiment, a force of 12.5 mN was chosen as a typical clinically representative expansion force based on radial force testing. A 1.5 mN pre-load was applied, followed by displacement-controlled loading at 1.5 mm/min to reach the targeted 12.5 mN load (loading phase). The 12.5 mN load was subsequently held constant using force-controlled loading for 5 mins to replicate the embedding time (creep phase): see Supplementary Materials online supplementary figure S1 for full experimental data, including an illustration of loading and creep phase. Clot stiffness was measured as the initial compressive stiffness on indentation, tensile stiffness was not considered.
Supplementary file 1
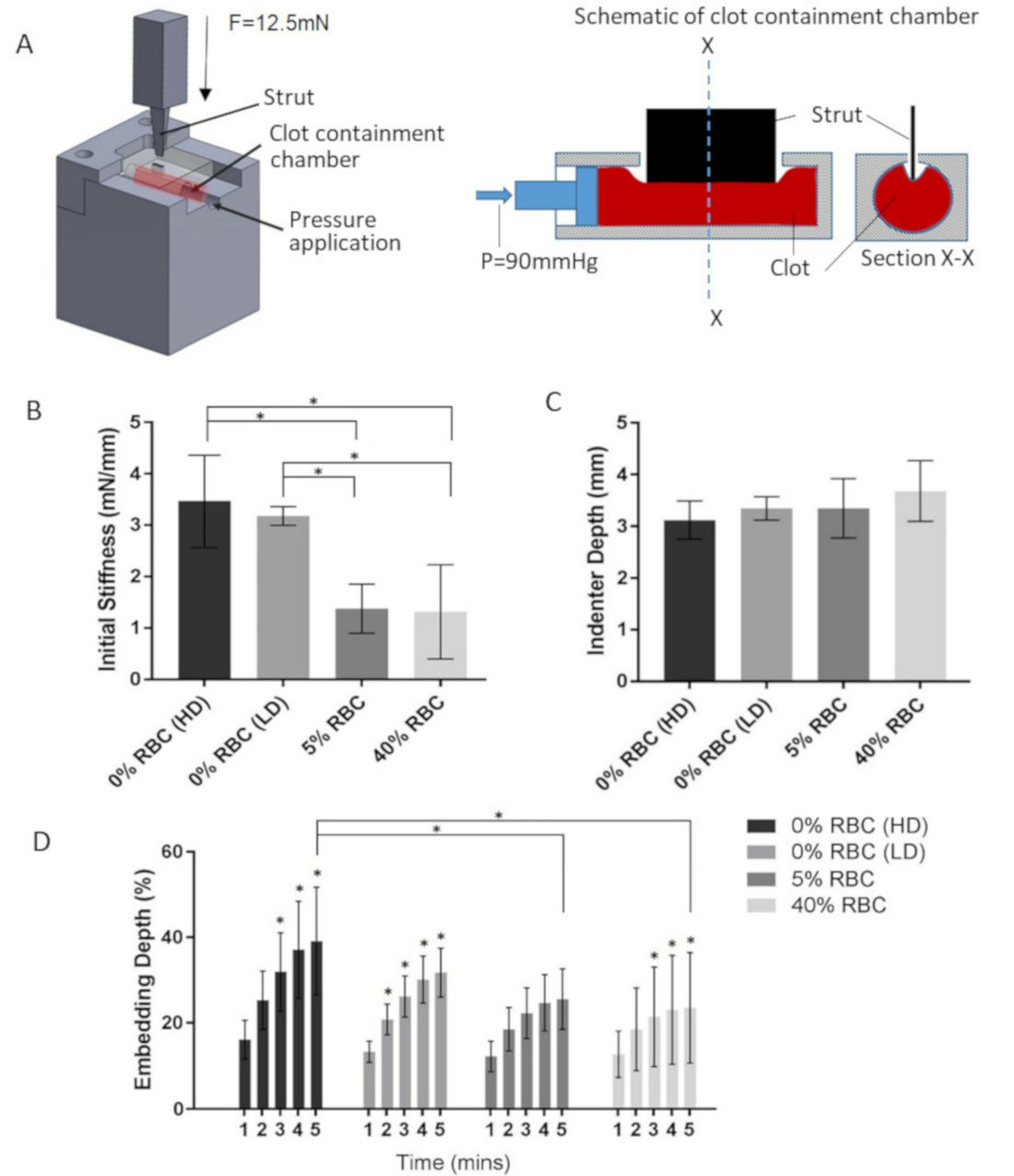
(A) Schematic diagram illustrating strut indentation test setup: a 12.5 mN force, F, is applied to a clot within the containment chamber, the clot is pressurized via pressure force, P, equivalent to 90 mmHg during testing. Resulting (B) initial compressive clot stiffness, *=P < 0.05 (C) maximum indenter depth, and (D) additional embedding depth achieved over the embedding time, *=P < 0.05. Ten replicate clot samples were used for each clot analog type tested. Data are mean ±SD deviation.
SEM imaging clot preparation and analysis
Two samples from each of the five clot analog groups were cut to cylindrical dimensions of 5 mm diameter with 10 mm length prior to preparation for SEM imaging to analyze microstructural variations pre- and post-indentation. Samples were rinsed with a 0.1M phosphate buffered saline (PBS) in preparation for fixation. The baseline samples were fixed immediately using 2.5% glutaraldehyde solution. The samples to be indented were placed in a tube (I.D. 5 mm) with an indenter tip subsequently inserted vertically into an incision in each tube. Each clot was indented by the respective initial depth achieved at 12.5 mN, as determined by the indentation testing, before fixing. Samples were left in fixative for 2 hours at room temperature, then rinsed with PBS, submerged in PBS for 5 mins and rinsed again. Dehydration of all samples was then completed by placing the samples in increasing concentrations of ethanol (50, 75, 80, 90%, and 100%) at 4°C for 5 mins. The samples were then placed in hexamethyldisilazane (HMDS) for 30 mins and allowed to air-dry prior to SEM imaging. Samples were gold-plated prior to SEM imaging. Imaging was completed using a Hitachi S-4700 microscope with a 15kV operating voltage.
µCT imaging clot preparation and analysis
One sample from each clot analog group was cut to cylindrical dimensions of 2.5 mm diameter with 5 mm length. Simulated stentriever deployment with EmboTrap MT devices (Cerenovus, Galway, Ireland) were performed in silicone tubes (I.D. 3.35 mm), each containing a clot sample from each respective group and held in a water bath at 37°C. It should be noted that while active deployment techniques, such as device advancement during unsheathing, can be used with conventional stentrievers to increase apparent efficacy,20 26 these techniques are not applicable to the EmboTrap due to its unique petal-like cage design: a ‘simple’ unsheathing technique was employed. Following an embedding time of 5 mins, the clot/device/tube assemblies were rinsed in PBS and placed in 4% paraformaldehyde (PFA) fixative for 2.5 hours. The sample assemblies were subsequently rinsed with PBS, stained with 2.5% phosphomolybdic acid (PMA) for 3 days, rinsed again and dried before µCT scanning. Finally, each sample was scanned at a 5 µm resolution (Scanco Medical µCT100). Post-processing was completed using Mimics Research v.18.0 and 3-matic Research v.11.0 (Materialise NV, Leuven, Belgium). Samples were evaluated to determine clot response to strut contact, i.e. if the device results in a deflection of the thrombus surface, or if the strut penetrates the thrombus.
The cross-sectional area of each clot was calculated for every tenth slice (or every 0.2 mm) along its full length such that the total clot volume was considered (see Supplementary Materials online supplementary figure S2). The volume of each clot in addition to an idealized stent volume, created by interpolating the contours of the stent perimeter, were segmented. With the segmented geometries overlaid, the ‘intersection’ Boolean operator was used to segment the ‘integrated clot’, i.e. the volume of clot which intersected, or integrated, into the device. In addition, due to the unique design of the EmboTrap device, specific analysis was also completed on the ‘open’ and ‘closed’ regions along the length of the device. Namely, 10 representative slices from the center of each open and closed region were isolated for analysis (as labeled in Supplementary Materials online supplementary figure S3). The resulting percentage integrated clot was normalized using the total volume of clot from each respective slice analyzed. Slices along the center of the open and closed regions, respectively, were used as the boundary zones between these regions can be subjective due to device deformation on deployment at the location of the clot.
Statistical analysis
Statistical analysis for the indentation experimental work was completed using a one-way analysis of variance (ANOVA) test, and post-hoc analysis was performed using Bonferroni’s multiple comparisons test. For the integrated clot in the ‘open’ and ‘closed’ regions of the device, a two-way analysis of variance (ANOVA) test with Tukey’s multiple comparisons post-hoc test was used to compare the means of each group to each other (n=10 slices from each open/closed region). All statistical analysis in this work was completed using GraphPad Prism v.7.0 for Windows (GraphPad Software, LA Jolla, CA, USA).
Results
Clot indentation behavior
Clot stiffness (measured as the initial compressive stiffness on indentation) was shown to significantly decrease with increasing RBC content (figure 2B) with a corresponding marginal increase in maximum depth achieved by the indenter tip (figure 2C). Interestingly, however, the additional depth achieved per minute over the simulated 5-mins embedding time (creep phase) was shown to decrease with increasing RBC content (figure 2D). The embedding depth of figure 2D represents the total depth achieved by the indenter into the clot sample over the 5-mins embedding time, expressed as a percentage of the depth at initiation of the embedding time (time, t=0). Changes in embedding depth analyzed over 1-min intervals, compared with the depth at 1 min as a control, is most evident in the 0% RBC clot analog groups: statistically significant increases in embedding depth per minute are marked in figure 2D. The benefit of an embedding time was most pronounced in the 0% RBC high-density clot analogs (representing a more densely packed fibrin network mature clot) in demonstrating a 36.35%±16.64% total gain in depth achieved by the indenter tip after the f5-mins embedding time. An inverse relationship was observed between initial clot compressive stiffness (figure 2B) and initial indenter depth (figure 2C). This is plausible as the stiffer the clot is, the less initial indentation is observed. Conversely, there is a direct relationship between initial clot compressive stiffness (figure 2B), viscoelastic behavior,(online supplementary figure S1B) and the additional depth achieved by the indenter during the 5-min embedding time (figure 2D). This infers a higher level of creep in the stiffer fibrin-rich clots. It should be noted that the resulting data from the 80% RBC clot analogs are excluded from the results shown in figure 2. These clots could not be tested due to the pressurization of the chamber, combined with the nature of the clots: the clots protruded through the central slot of the upper steel plate on pressurization, in addition the indenter tip reached the bottom of the containment chamber before the target 12.5 mN force was reached.
SEM microstructural imaging analysis
From SEM imaging of the clot analogs, the microstructure of the baseline 0% RBC clots of high- (figure 3A) and low-density (figure 3C), produced from 100% plasma, are shown to consist of an organized fibrin network. The baseline 5% RBC clot analog (figure 3E) is shown to have a heterogeneous structure containing RBCs and fibrin strands. Meanwhile, the baseline 40% and 80% RBC clot analogs (figure 3G and I, respectively) have a more uniform structure with fibrin strands located loosely around RBCs. At the indentation site of the indented clot samples, stretching of the fibrin network can be identified as the predominant mechanism of strain accommodation in lower RBC content clots (figure 3B, D and F). Conversely, with increasing RBC and decreasing fibrin content, complete rupture of the fibrin strands was identified at the indentation site (figure 3H and J). This suggests RBC-rich clots are more friable and have a higher probability of fragmentation during MT.
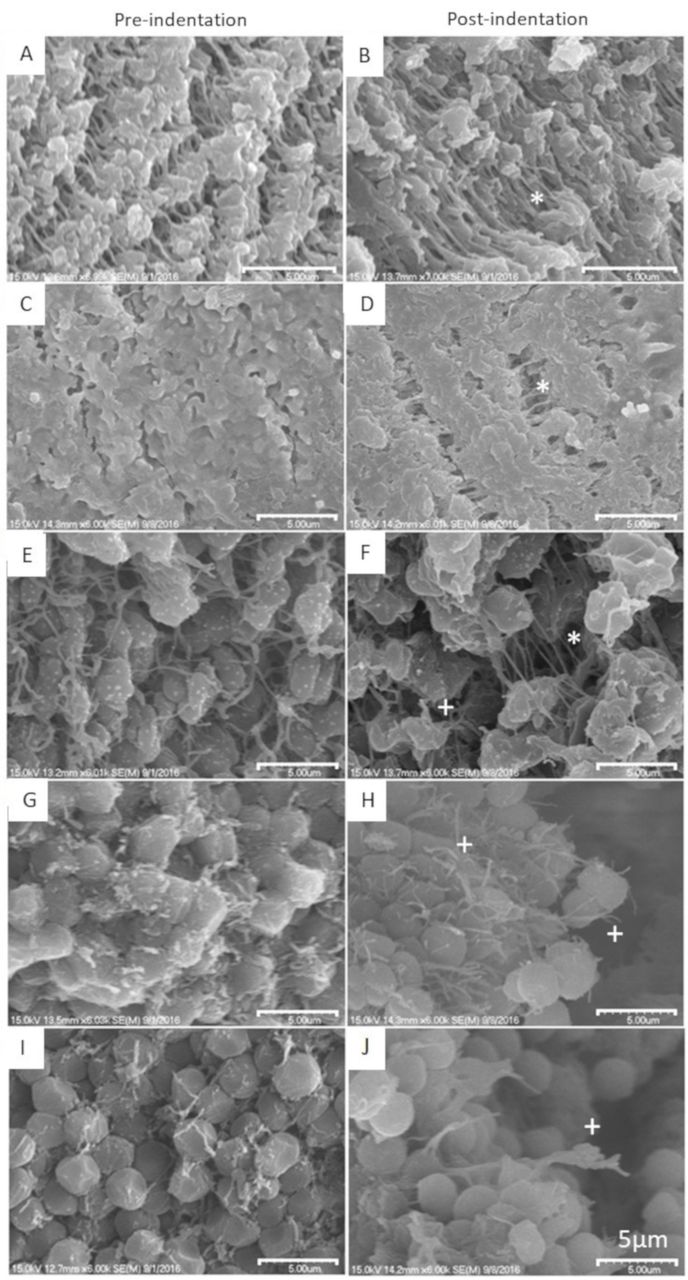
SEM imaging of the various clot analogs before and after indentation testing; (A) and (B) 0% RBC high-density clot, (C) and (D) 0% RBC low -density clot, (E) and (F) 5% RBC clot, (G) and (H) 40% RBC clot, (I) and (J) 80% RBC clot, before and after indentation testing, respectively. * indicates fibrin stretching and +represents fibrin rupture. All scale bars are 5 µm.
µCT integrated clot imaging analysis
Thus far, results pertaining to the degree of indentation achieved by a single stent strut alone have been analyzed across a range of clot analogs. The µCT imaging phase of this experimental work sought to assess clot deformation behavior as it interacts with a specific stentriever device deign, namely, the EmboTrap MT device (Cerenovus, Galway, Ireland). The magnitude of clot integration volume into the stentriever device was evaluated along the full length of the clot for each of the five clot/device assemblies. Integrated clot volume reconstructions were isolated and assessed for two regions of interest, namely the ‘open’ and ‘closed’ regions as identified in figure 4A: this portion of the study did not involve an embedding wait time. Greater average clot integration was demonstrated to occur in the lower scaffolded open regions of the device than in the more scaffolded closed regions: see also Supplementary Materials online supplementary figure S3. As shown in the results of figure 4A, a statistically significant increase in clot integration is demonstrated between the open and closed regions of the EmboTrap for both 0% RBC clot analog groups. As shown in figure 4B, the length of the occluding clot is altered on deployment of a device, with a tendency for increased length with increased cellular content. Overall there is a trend of increasing ‘integrated clot’ volume into the device with increasing RBC content (figure 4C). This observation agrees with the results of the experimental clot indentation testing which showed greatest indenter depth in the highest RBC content clots (figure 2C). In addition, corroborating the results for the fibrin-rich (0% RBC) clots, there is a decreased integration demonstrated in the high-density clot when compared with the low-density fibrin-rich clot.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Clot integration at ‘open’ and ‘closed’ regions in the EmboTrap MT device for each of the clot analogs: low scaffolded open regions leading to generally higher levels of integration than highly scaffolded closed regions. (B) Demonstrated increase in axial length of clot following device expansion increasing with RBC content. (C) Methodology used in this study for µCT segmentation and the calculated ‘integrated clot’ volume for each clot analog tested: overall level of integration increases with RBC content.
Discussion
The efficacy of removing an occluding clot during MT has been shown to be influenced by histologic characteristics: RBC-rich clots are easier to remove than fibrin-rich clots, however, RBC-rich clots are prone to fragmentation.7 15 In this work, the depth of single strut indentation in addition to the degree of device-clot integration following an embedding time of 5 mins was correlated with clot RBC content. The reported mechanical response of the clot analogs, namely the compressive clot stiffness (figure 2B) and viscoelastic behavior (online supplementary figure S1B), in this study reflecting those reported in the literature.13–15 In addition, the microstructural characteristics of tested clot analogs, achieved under SEM, also substantiate findings in the literature. Specifically, clot analogs with 0% RBCs consist primarily of a dense fibrin network while low RBC concentrations (5% RBC) show heterogeneity in the fibrin network with some interspersed RBCs. Meanwhile, clots with high levels of RBCs (40% and 80% RBC) show less organized structures with fibrin stands loosely intertwined around RBCs.15 27 28 Such similarities in observations with the literature strengthen the validity of the experimentally determined results of this study.
In this work, an increased maximum depth was demonstrated by the single indenter tip with increasing RBC content of the clot analogs. An additional embedding depth achieved by the indenter tip over a f5-mins embedding time was observed for all clot analogs up to 40% RBC: the 80% RBC clot analogs could not be tested in the same manner due to the maximum depth being reached prior to initiation of the embedding time. The benefit of an embedding time was most pronounced in the 0% RBC high density clot analogs (representing a highly organized mature clot with a network of taut branched fibrin fibers) showing a 36.35%±16.64% increase in total indentation depth over this 5-mins period. The relatively minor change in additional depth achieved with increasing RBC content of clot analogs (compared with fibrin-rich clots) may be attributed to the reduction in fibrin-stretching occurring due to the decreasing fibrin network density of the clots.
SEM observed local clot stretching in combination with µCT characterized clot elongation was reported for all clots types tested, except for the high-density 0% RBC clot which showed no sign of length change on device deployment. To the authors' knowledge, this is the first time local clot stretching, in addition to global clot length change, due to clot/device interaction has been quantitively reported. Meanwhile, SEM observations of local rupture of the fibrin network in clots indented by the single stent occurred primarily in clots with higher RBC content (most frequently observed in 40% and 80% RBC content clot analogs) suggesting these clots are more vulnerable to fragmentation than fibrin-rich clots.
A significant finding of this study was the specific nature of interaction between the EmboTrap MT device (Cerenovus, Galway, Ireland) and the occluding thrombus. The EmboTrap was selected for analysis in this study due to its unique design. Thrombectomy devices typically consist of a closed cell cylindrical design which rely on radial force to compress the occluding clot between the outside of the device and the vessel wall. Meanwhile, the EmboTrap has a dynamic segmented open cell design in which the clot is encouraged inside the device in a stable configuration between the inner channel and outer cage. On device deployment, it was identified that a local deflection of the clot surface occurred as opposed to direct penetration of the device struts through the clot. In addition, the degree of clot integration into the device decreased with decreasing RBC content. This result, in combination with the single strut indentation results, highlight the clinical importance of an embedding time when dealing with fibrin-rich clots. It was also found that a higher percentage of clot integration occurred in regions of ‘open’ architecture of the EmboTrap device: a statistically significant increase in clot integration was demonstrated in both 0% RBC clot analog groups. This highlights the importance of the device placement with respect to an occluding thrombus to improve efficacy during MT. Furthermore, through in vitro testing, this segmented design has been proven to increase the efficacy of MT through entrapment of the clot in place of clot compression against the vessel wall especially in tortuous anatomies where other more simplistic stentriever designs have shown poor success rates.29
We acknowledge the following limitations of the work: first, clot analogs were manufactured from ovine blood and may not correspond directly to the mechanical properties of human thrombi. Second, only one clot sample per clot analog group was used in the µCT testing described in this work, preventing any statistical analysis being completed on this portion of the study. Third, as no working fluid was included in the indentation test, the dynamic effect of blood flow was not captured, however, as the unloading behavior of the clot was not under investigation, adhesion effects of the indenter tip to the soft biological material of the clot was not of concern. Fourth, the loading rate is relatively slow due to a limitation of the testing equipment at low forces, however it gives a reasonable representation of the deployment behavior and eliminates early viscoelastic effects while reaching the required 12.5 mN load. Next, the design of the indentation fixture represents a single strut only, as a result the SEM work of this study does not capture variations that may occur due to differences in stentriever strut dimensions, angulation, or variation due to vessel size. In a similar manner, as only one mechanical thrombectomy device was analyzed in the µCT work of this study, general conclusions relating to thrombectomy devices cannot be made. Conclusions drawn in this study are therefore specific to the unique open cell design of the EmboTrap. Finally, data before the 1.5 mN pre-load is excluded as this pre-load was assumed to represent the point at which the indenter first contacts the clot surface.
Conclusions
In this study the indentation depth of a single strut of a MT device, as well as the additional depth achieved during an embedding time of 5 mins, was examined for a range of clot analogs of varying fibrin:RBC compositions intended to represent the diversity of AIS thrombi. This study also uses µCT imaging techniques to evaluate the specific device-clot interaction behavior between various clot analog types, of varying fibrin:RBC ratio, and the EmboTrap MT device (Cerenovus, Galway, Ireland). We can draw three conclusions from this study. First, strut contact most commonly results in surface deflections rather than clot penetration. Best integration is achieved in areas of the EmboTrap device with open architecture, highlighting the importance of device placement with respect to an occluding thrombus during MT. Second, we suggest that increasing RBC content (less dense fibrin network) leads to decreasing compressive clot stiffness, thereby enabling a small amount of fibrin stretching before eventual rupture on indentation. In addition, there appears to be a critical RBC content (between 40% and 80% RBC) in which local fibrin rupture becomes the primary mechanism of clot deformation, causing clot fragmentation to become an increasing risk factor which may lead to embolic matter. Third, the effectiveness of an embedding time is dependent on clot type and has the most clinical significance for MT efficacy for a mature fibrin-rich clot. These conclusions add to the current understanding of MT procedures and device interaction with occluding thrombi during therapeutic interventions, specifically increasing the understanding of strut indentation in different clot types.
Acknowledgments
The authors would like to acknowledge David Connolly for his assistance with the µCT scanning which was completed at the National University of Ireland, Galway.
References
Footnotes
Contributors FMW: Experimental conception and design, data collection and analysis, manuscript writing and editing. SD: Clot preparation. IM: Assisted with µCT analysis. GG: Data interpretation. PM: Data interpretation, manuscript editing. ETR: Experimental conception and design, data interpretation, manuscript editing. PMc: Data interpretation. MG: Experimental conception and design, data interpretation and manuscript editing.
Funding This work was supported by Cerenovus, Galway and the National University of Ireland, Galway.
Competing interests FMW, SD, GMG, MG report a financial relationship with Cerenovus outside the submitted work.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Please contact the corresponding author with data sharing requests.