Article Text

Abstract
Background The transradial approach (TRA) to endovascular procedures decreases access site morbidity and mortality in comparison with the traditional transfemoral technique (TFA). Despite its improved safety profile, there is a concern that TRA is less favorable for neurointerventional procedures that require large coaxial systems to manage the small tortuous cerebral vessels.
Objective To report our experience with TRA for flow diverter placement for treatment of unruptured cerebral aneurysms.
Methods We performed a retrospective review of prospective institutional databases at two high-volume centers to identify 49 patients who underwent flow diversion for aneurysm treatment via primary TRA between November 2016 and November 2018. Patient demographics, procedural techniques, and clinical data were recorded.
Results Of the 49 patients, 39 underwent successful flow diversion placement by TRA. Ten patients were converted to TFA after attempted TRA. There were no procedural complications. Reasons for failure included tortuosity in eight patients and severe radial artery spasm in two.
Conclusions In the largest reported series to date of flow diverter deployment via TRA for aneurysm treatment, we demonstrate the technical feasibility and safety of the method. The most common reason for failure of TRA was an acute angle of left common carotid artery origin or left internal carotid artery tortuosity. Overall, our data suggest that increasing adoption of TRA is merited given its apparent equivalence to the current TFA technique and its documented reduction in access site complications.
- aneurysm
- flow diverter
- intervention
- technique
Statistics from Altmetric.com
Introduction
The transradial approach (TRA) has been widely adopted by interventional cardiologists owing to a reduction in access site complications as well as patient preference and cost in comparison with transfemoral access (TFA).1–10 We have published our extensive experience with the transition of our diagnostic and elective interventional procedures to a predominantly TRA approach.11–16 However, flow diversion presents unique technical challenges to neurointerventionalists, and in particular, for TRA. Owing to the stiffness and braided configuration of flow diverting stents, deployment requires a significant forward loading force. This, in turn, necessitates the use of larger-bore access systems and frequently, intermediate catheters for additional support. These support requirements may pose a challenge for TRA given the small size of the radial artery and the lack of dedicated radial access catheter systems optimized for the unique angles in the radial approach. However, given the significant safety benefits, particularly in flow diversion cases where dual antiplatelet therapy is essential, we began to preferentially employ TRA for flow diversion when feasible. In this study we present a large series of patients who underwent TRA for flow diversion, with particular emphasis on the indications, technical nuances, and pitfalls.
Methods
Study design
Following institutional review board approval, we reviewed prospective institutional databases at two high-volume centers of consecutive transradial neurointerventional procedures involving the placement of a flow-diverting stent between November 2016 and November 2018. Patient demographics, procedural and radiographic metrics, and clinical data were recorded.
Procedural technique
All patients underwent preprocedure assessment of collateral palmar circulation via Barbeau testing.17 Patients with no return of pulse tracing on plethysmography after release of ulnar compression (‘Barbeau D’) were excluded from TRA. Additional reasons for exclusion included age <18 years, known anatomic variants, arterial occlusion, stenosis, or fistulas in the ipsilateral arm. Patients are positioned with the arm placed tightly against the hip with the distal forearm and hand in a slightly supinated position (approximately 45o) and the wrist extended with a towel roll. The hand is elevated on cushions or towels so that it lies level with the superior surface of the thigh. Crucially, the space caudal to the hand is bolstered with a radial arm board extension and pads to create a level resting surface for the catheters next to the thigh, thus preventing the catheters from falling off the table. Like TFA, access is obtained with only the anteroposterior plane in position at the head side and the table rotated clockwise 5–10 degrees to obtain angiography of the radial/brachial bifurcation.11
The periarterial tissue is infiltrated with approximately 2 mL of lidocaine and the radial artery is cannulated using an anterior or counter-puncture technique. We employ ultrasound guidance in all cases of radial access as the RAUST trial showed that use of ultrasound increased speed and efficacy of first-time cannulation.18 A 6 French (F) short transradial introducer sheath (Glidesheath Slender, Terumo, Somerset, New Jersey, USA) is placed and spasmolytic drugs (2.5 mg of verapamil and 200 μg of nitroglycerin diluted in normal saline) are given intra-arterially via the sheath. Intravenous heparin (70 unit/kg) is administered to maintain an activated clotting time of between 250 and 350.
Three general techniques are used to perform TRA with the available femoral neurointerventional catheters. Our initial technique involved a 6 F Envoy DA guide catheter (Codman Neuro, DePuy Synthes, Raynham, Massachusetts, USA) that is coaxially navigated into the target internal carotid artery (ICA) over a 125 cm Simmons-2 shaped Select diagnostic catheter (Penumbra, Alameda, California, USA) and 180 cm soft-tipped 035" hydrophilic wire (Glidewire, Terumo, Somerset, New Jersey, USA).11 More recently, we began to use the larger-bore 088" Infinity guide catheter (Stryker, Fremont, California, USA) for greater support in tortuous vessels. This is reserved for patients with a radial artery diameter >2.5 mm. In these cases the 6 F radial sheath is placed first and the spasmolytic cocktail is injected. Under road map guidance the sheath is then exchanged for the 088" ID catheter into the axillary artery without a sheath. The guide catheter is then placed into the target vessel in a telescoping fashion with a 125 cm Select Simmons-2 catheter and hydrophilic wire, as described above. A third technique, used for radial artery diameters <2.5 mm, involves placing the 6 F vascular sheath as above but rather than exchanging it for an 088" Infinity guide catheter, the sheath is exchanged for an intermediate catheter (072" Navien [Medtronic, Minneapolis, Minnesota, USA], 070" Sofia [MicroVention, Terumo, Somerset, New Jersey, USA], 060" Syphontrak [DePuy Synthes, Raynham, Massachusetts, USA]), which is then navigated directly over the glidewire into the target vessel without a guide catheter.
Flow diverter deployment
After the guide catheter is in place in the target vessel, a coaxial system of an intermediate catheter (060" Syphontrak if using 088" guide, 044" DAC or 058" Navien for 071" guide system) over a 027" Phenom microcatheter (Medtronic, Minneapolis, Minneapolis, USA) is tracked over the Synchro wire (Stryker Neurovascular, Fremont, California, USA) across the aneurysm neck. The wire is then removed and the stent is deployed through the microcatheter in the standard fashion.
Results
Procedures
A total of 49 patients (26 from Jackson Memorial Hospital/University of Miami and 23 from Washington University in St Louis) underwent initial TRA for placement of a flow diverting stent for treatment of unruptured aneurysms between November 2016 and November 2018. The average age of patients was 57.8 (range 16–81) years and most patients were female (82%, 40/49). Details of the location and laterality of the aneurysms are listed in table 1. The treatment involved catheterization of the left ICA in 29 patients, right ICA in 15 patients, left vertebral artery in 3 patients, and right vertebral artery in 2 patients. The right radial artery was used in all but three patients with left vertebral artery aneurysms, in which the left radial artery was accessed. The selection of catheter systems was determined by the two senior authors. Thirty-one percent (15/49) of cases were performed with a triaxial 088" system, 31% (15/49) with a quadraxial 071" or 072" system, and 18% (9/49) were performed with a biaxial intermediate catheter directly without a guide catheter or sheath (table 1).
Characteristics of TRA flow diversion cases
Of the 49 patients, 39 underwent successful flow diversion placement by TRA. Ten patients were converted to TFA after attempted TRA. Reasons for failure included left common carotid artery acute angle of origin in four patients, left common carotid artery and ICA tortuosity in five patients, and severe radial artery spasm in two patients (table 2).
Pertinent characteristics of patients for whom TRA failed
Placement of the TFA flow diversion device was successful in 8 of the 10 cross-over cases. In the other two cases (JMH 6 and WUSTL 16) the guide catheter could not be navigated into the LICA owing to arch tortuosity via the transfemoral trajectory, and ultimately the case was converted to clipping (JMH 6) and stent-assisted coiling of the aneurysm via TRA (WUSTL 16).
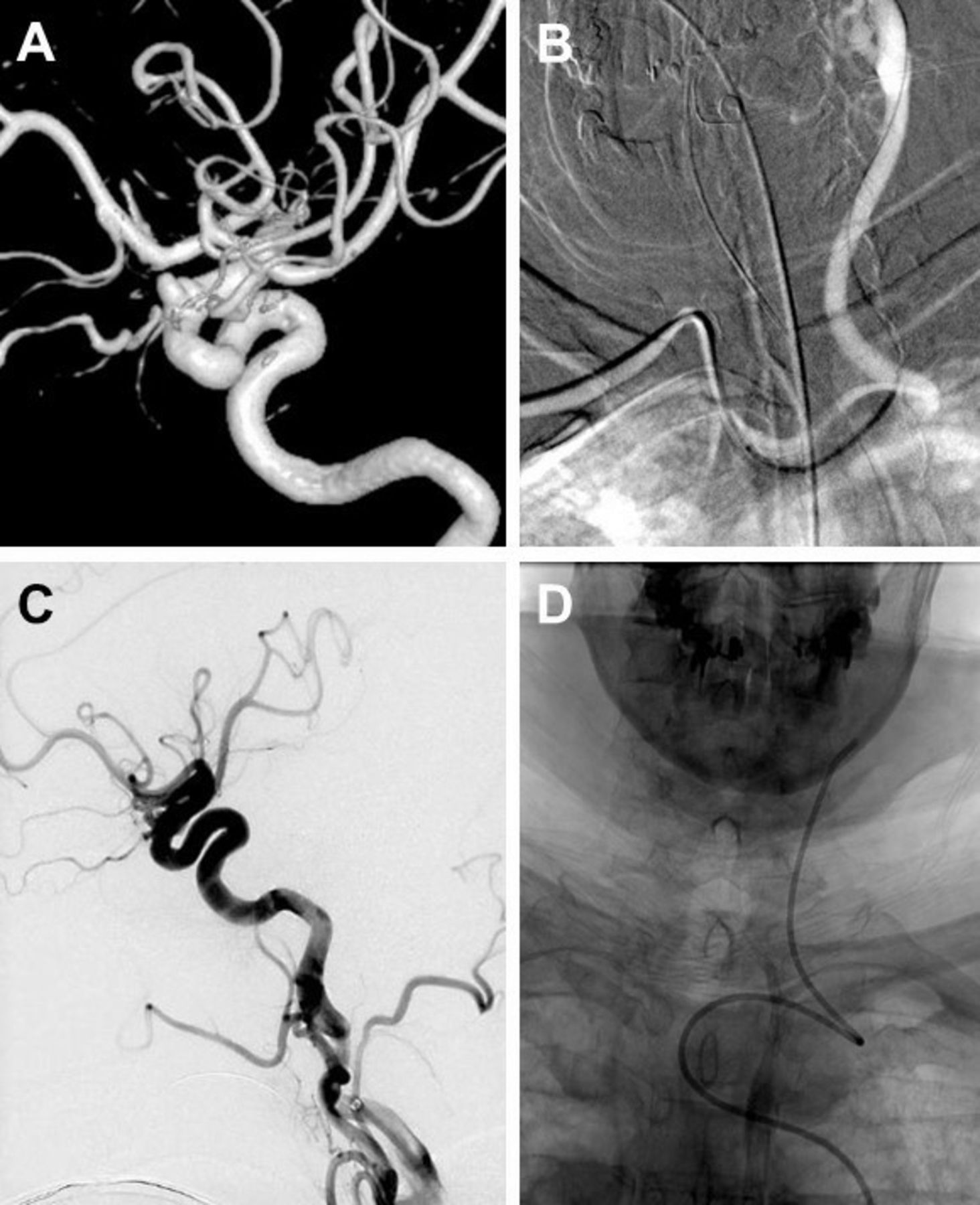
There were no procedural or postoperative neurological complications. No cases of symptomatic radial artery occlusion or access site hematomas occurred. A representative case is illustrated in figure 1.

A middle-aged patient presenting with thunderclap headaches found to have an unruptured bilobed ophthalmic aneurysm measuring 3.8×2.8 mm and 1.8×1.3 mm. (A) 3D reconstruction of the left internal carotid artery (ICA) on rotational DSA demonstrating bilobed ophthalmic aneurysm. (B) Road map guidance of the left common carotid artery from the right subclavian artery demonstrating severe kink of origin. (C) Left ICA angiogram demonstrating severe tortuosity of the left ICA. (D) Combination of proximal and distal ICA tortuosity did not allow for flow diverting deployment despite its placement in the distal artery and ICA. Thus, the case was converted to transfemoral access.
Discussion
Transradial approach advantages
Numerous randomized controlled trials in the cardiology literature comparing TRA with TFA have demonstrated an unequivocal benefit of reduced morbidity and mortality in the TRA cohort.1–7 The superficial and distal location of the radial artery confers the benefit of easy positioning, peripheral access, and reliable compression hemostasis. Additionally, as our institutional practice has transitioned to employing primary TRA for diagnostic angiography and neurointerventions, our experience echoes that of cardiology for greater patient preference and shorter hospital stays for TRA.11 However, the safety benefit of TRA is especially compelling in cases of neurointervention where large-bore systems are used and dual antiplatelet therapy and full anticoagulation is needed. This has led us to adopt TRA for flow diversion deployment. For TRA flow diversion, the precise, controlled delivery of a large and relatively rigid device into a distal deployment site presents a unique technical challenge.
There have been only three previously reported cases of successful placement of a Pipeline endovascular device for intracranial aneurysm treatment using TRA. All cases were selected owing to type III aortic arches or bovine arch configurations.19–21 These case reports highlight the favorable trajectory of TRA over TFA, particularly for left-sided carotid catheterization in patients with complex arches.12 However, the overwhelming evidence of the superior safety of TRA suggests that neurointerventionalists should consider primarily employing TRA in all cases when feasible, rather than limiting TRA to patients with complex arch anatomy. In this case series, we show that flow diversion is feasible and safe via TRA and discuss the nuances of flow diverter placement through the use of radial triaxial or biaxial systems for both anterior and posterior circulation aneurysms at various locations.
Technical nuances
We have described our approach to TRA in detail; however, transradial flow diversion poses additional challenges.11–16 Catheter selection in performing flow diversion via a transradial approach is limited by the size of the radial artery. Studies have shown that the rate of radial artery occlusion (RAO) significantly increases for radial artery diameters of <2.5 mm and with increased sheath to artery size ratio.22 The system providing the greatest stability consists of a triaxial system with an 088" guide catheter (outer diameter 2.7 mm) in the distal ICA/vertebral artery. Although the clinical relevance of RAO remains debatable, for elective cases, we are more conservative in employing a cut-off point of 2.5 mm for use of the 088" guide catheter in order to avoid problems with RAO and radial artery spasm during the procedure. For radial arteries measuring >2.5 mm in diameter on ultrasound, an 088" guide catheter is placed without a sheath into the distal ICA as described in the ’Methods' section. This larger system allows for the use of larger intermediate catheter systems (060" Syphontrak) with superior stability and trackability in tortuous vessels. Of note, the 088" Infinity Long Sheath (Stryker, Fremont, California, USA) offers unique advantages for this sheathless approach—namely, a longer stylet with less mismatch between the inner diameter of the catheter and the outer diameter of the stylet than with the NeuronMax (Penumbra, Alameda, California, USA). Significant mismatch can lead to difficulty in transition through the skin as well as sharp leading edge of the catheter that may injure the endothelium in smaller vascular structures.
In cases where the radial artery is too small to accommodate the 088" guide (<2.5 mm), we have employed a multitude of biaxial, triaxial, or quadraxial systems. Most commonly, with a short 6 F sheath placed directly into the radial artery, a quadraxial system with a 070" to 071" guide catheter is navigated into the ICA or vertebral artery, before distal navigation is completed with the intermediate 044" to 058" system introduced over the microsystem. Occasionally, subtle deformations due to tortuosity or catheter manufacturing in the 071" guide (typically an Envoy DA) can preclude use of an 058" Navien catheter, which has an outer diameter of 070". In such cases, an 044" intermediate catheter can be employed; however, the reduced stability can prevent successful navigation of the device into distal vessels. Alternatively, triaxial systems can be used in patients in whom an intermediate catheter is placed without a guide, or a 070" to 072" guide catheter is placed without a sheath into the target vessel, as described in the ’Methods' section. An intermediate catheter without a guide catheter was used only in cases where requirements for support were predictably less, based on straight anatomy on the pretreatment angiogram.
We thus tailor the technique to each individual patient, taking into consideration the laterality of the target vessel, tortuosity of the proximal and distal vessel, and size of the radial artery. In general, for patients with a radial artery measuring >2.5 mm we prefer the triaxial 088" Stryker LS (Stryker Neurovascular, Fremont, California, USA), 060" Syphontrak intermediate catheter, 027" Phenom system. When the tortuosity of the left ICA or common carotid artery (cervical loops/kinks, high riding posterior genu of cavernous carotid) is challenging or in the presence of giant aneurysms requiring long stent constructs, we proceed with the 088" triaxial system if the radial artery measures ≥ 2.5 mm on ultrasound, or TFA if the artery is < 2.5 mm. For patients with relatively straight anatomy and radial artery diameter <2.5 mm, we use the 071" systems (Envoy DA with 058" Navien or 044" DAC) or less commonly, exchange for a triaxial system with an intermediate catheter and microcatheter system for deployment of a flow diversion device.
For the next generation of flow diversion devices, we believe that failure rates of the Pipeline devices will decrease with the introduction of softer and more navigable stents alongside radial-specific access systems. However, for stents that are stiffer, the failure rate may be higher. In our study, next-generation devices, such as the Surpass Streamline flow diverter (Stryker Neurovascular, Fremont, California, USA) and similar, were not used.
TRA outcomes
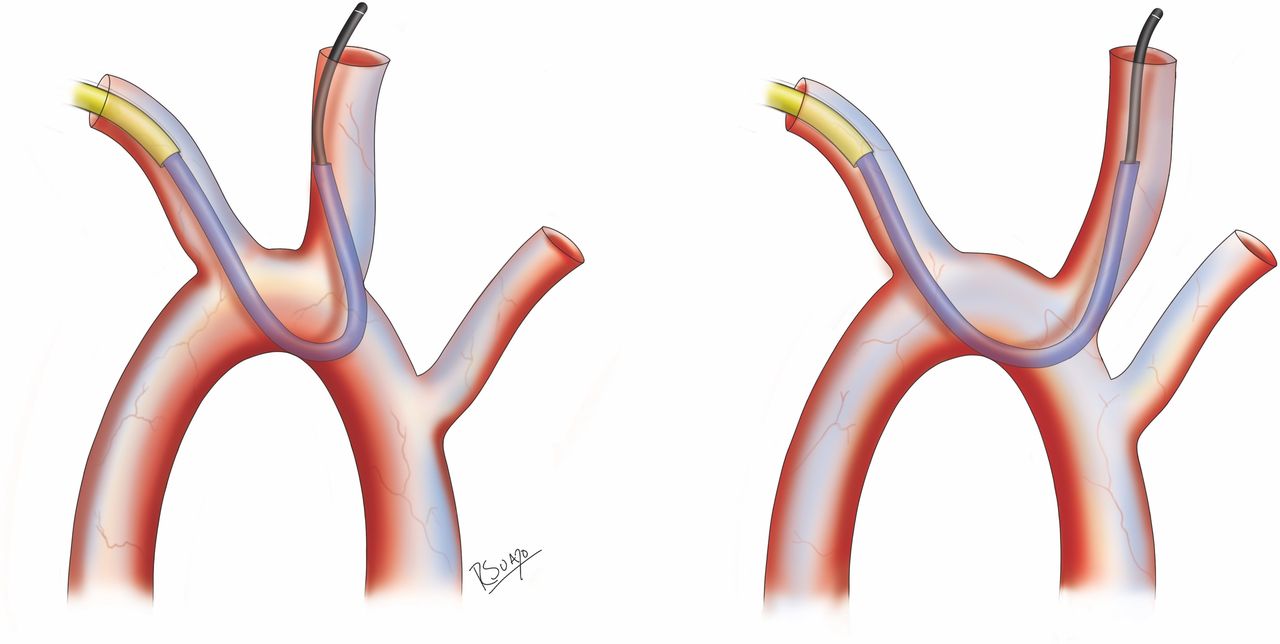
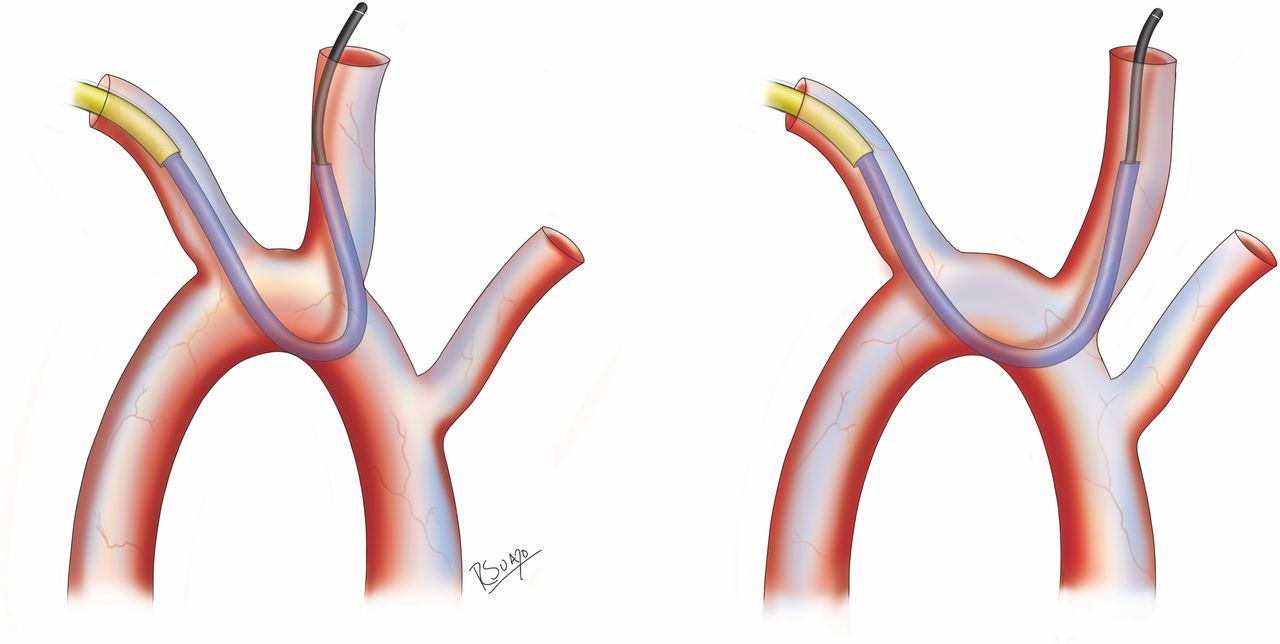
Eight patients in our series required a change from TRA to TFA due to severe proximal left internal carotid tortuosity (four patients) or steep angulation of the left common carotid artery origin (four patients). A 088" guide catheter was used in three of the cases and a 071" guide catheter system in five of the eight TRA failures. In the cases of LICA tortuosity, the system did not have sufficient support, which resulted in the whole system retracting while trying to advance the stent or an inability to advance the stent despite significant pushing of the stent pusher. In the cases of acute LCCA origin angulation, system herniation occurred when trying to navigate and maintain the guide catheter into the distal ICA. At this time, the femoral catheter transitions are not optimized for the turn upwards into the great vessels. A deep acute angle between the innominate and left common carotid artery tends to result in failure, whereas a wide-angle parabola shape is predictably stable (figure 2). Herniation occurs because the distal Simmons catheter cannot fully engage with the left common carotid artery and the proximal portion has minimal purchase in the arch. Sometimes, this can be overcome by slowly and repeatedly balancing wire advancement, Select catheter advancement, and guide catheter advancement. During this process it is necessary to unlink the collimators to visualize the catheter in the arch as the wire is being navigated distally into the ICA. However, as discussed above, even in cases where the procedure was successfully completed, we found that a 071" system was significantly less stable.
{kind=link}
{kind=link}
An acute angle between the innominate and left common carotid artery is more challenging for tracking the system into the internal carotid artery and may lead to herniation of the catheter into the arch.
In this series, only two patients required conversion from TRA to TFA due to severe radial artery spasm. In order to prophylactically combat this problem, we apply a lidocaine/prilocaine patch at least 30 min before the procedure, inject subcutaneous lidocaine, and infuse intra-arterial anti-spasmolytic agents immediately after the vascular sheath is placed. Additionally, we use ultrasound guidance to measure the radial artery and for visualization during puncture to minimize the number of attempts at cannulation. In patients who develop spasm, management can include local subcutaneous injection of nitroglycerin/verapamil, warm compress, and ulnar compression. Ultimately, while long-term serious complications from spasm are rare, this complication can result in access and procedural failure.23 24
There were no complications in our case series. No patients experienced symptomatic RAO or stenosis. Asymptomatic occlusion of the radial artery may occur in approximately 5% of cases after radial access, and is typically associated with prolonged sheath placement over 3 hours.22 25 We routinely perform Doppler ultrasound of the distal radial artery after arterial access; however, we have found no clinical consequence. No patients experienced severe pain, skin desquamation, or hand ischemia, which is an extremely rare complication even in the setting of ~5% RAO rates in the literature. There were also no neurologic complications associated with the procedures.
Limitations
This study is limited by the small number of patients and the retrospective review of our prospective database. As such, data for asymptomatic radial artery occlusion were not routinely collected, although symptomatic access site complications were encountered. Our prospective databases similarly did not initially include information about the patients who were excluded from analysis owing to Barbeau test status. Current collection protocols include these data points. Furthermore, these 49 patients represent our initial experience with transradial catheterization for deployment of a flow diversion device by two different primary operators and is subject to selection bias and technical heterogeneity. However, these promising preliminary results certainly warrant further studies.
Conclusion
This is the largest reported series to date of flow diverter deployment via TRA for aneurysm treatment. In this study, we demonstrate the technical feasibility and safety of TRA for the vast majority of aneurysms regardless of location, while also showing a decreased risk of major access site complications in comparison with TFA. The most common reason for failure of TRA was left common carotid tortuosity. However, with further experience, improvement in technology, and optimization of technique we feel increased adoption of this approach is warranted.
References
Footnotes
Contributors All authors contributed to the conception, data gathering, and drafting of the manuscript. DRY, RMS, and ECP provided manuscript oversight and administrative support. All authors critically reviewed the manuscript and approved its final submission.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests BMS is a stockholder in RIST Neurovascular. RMS is a consultant for Medtronic Neurovascular, Cerenovus, and Abbott. DRY is a consultant for Medtronic Neurovascular, Cerenovus, and Rapid Medical and Neural Analytics. JWO is a consultant for Microvention. ECP is a consultant for Stryker Neurovascular, Penumbra, Medtronic Neurovascular, and Cerenovus, and is a stockholder in RIST Neurovascular.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.