Article Text

Abstract
Purpose The aim of our study was to assess the technical success and the safety of this new low-profile flow diverter Silk Vista Baby (SVB) by evaluating the intraprocedural and periprocedural complication rate.
Material/methods Clinical, procedural, and angiographic data were analyzed.
Results: 41 consecutive patients (28 women; age average 50.5 years) with 43 aneurysms were treated with SVB. Aneurysm sizes were classified by their maximum diameter, with an average size of 9.5 mm (range 2–30 mm). Thirty-four cases were unruptured. five aneurysms previously ruptured, had recurrence after the initial coiling. There were two ruptured cases. Aneurysms' locations were: M1 segment (five cases), M2 segment (three cases), M3 segment (one case), middle cerebral artery (MCA) bifurcation (six cases), carotid-T (two cases), anterior communicating artery/A1/A2 (11 cases), pericallosal artery (four cases), supraclinoid ICA (two cases), PCom (one case), V4 segment (three cases), PCA (three cases), SCA (one case), and PICA (one case). We had five intraprocedural complications which resolved without clinical consequences and three events postprocedural events. Initial occlusion rates were: eight aneurysms (18.6%) were completely occluded, five aneurysms (11.6%) showed near-complete occlusion, four cases (9.3%) showed incomplete filling, and 26 cases (60.4%) showed persisting filling. The mRS score at discharge from the hospital did not change from the admission mRS score.
Conclusion Our study demonstrated that the use of the new low-profile flow diverter, SVB device, for the treatment of intracranial aneurysms is feasible and technically safe.
- flow diverter
- aneurysm
Statistics from Altmetric.com
Introduction
In the past decade, flow diverters have been widely used for the treatment of intracranial aneurysms. Their safety and efficacy have been demonstrated in numerous clinical studies and several large clinical series.1 2
Based on their ability to reconstruct the parent artery, indications of their use are constantly extending from giant aneurysms to small aneurysms and to aneurysms located on small vessels.3 Innovation including improved cathether technology and simplified device delivery systems have enabled more distal treatment above the circle of Willis and beyond. However, few publications have reported treatment-related outcomes of flow diversion in this location, and the efficacy and safety of this technique remainsunclear.4
The Silk Flow diverter (Balt Extrusion, Montmorency, France) received its CE mark approval in 2008. The first-generation implant was made of four strands of platinum and 44 strands of nitinol.5 6 The second-generation, so-called SilK+, received the CE mark in 2012: still available, the device is made of 48 wires with higher radial force, eight platinum wires, and four platinum coils, providing 35%–55% metal coverage when expanded to its nominal diameter with a porosity of 45%–60%.6 The Silk+ device is compatible with 0.021’ and 0.025”microcatheters, 90% reseathable, and its safety and efficacy have been demonstrated in a clinical series with more than 1500 patients treated with the device.7
The most recent and smaller version of the device, the Silk Vista Baby (SVB), is the only FD deliverable through a.0.017’ microcatheter and received the CE mark in 2018. The implant is made of 48 DFT wires (Drawn Filled tubing matching nitinol with a platinum core into a single wire) which allow a full radiopacity without additional platinum wires compared with its predecessors. It is 90% resheathable and it has been designed for vessels from 1.5 to 3.5 mm.
We present a multicenter retrospective series of 41 consecutive patients with 43 aneurysms treated with the new SVB. The aim of our study was to assess the technical success and the safety of this new device by evaluating the intraprocedural and periprocedural complication rate after its use in several European institutions.
Material and methods
The study involved a retrospective review of multicenter data regarding a consecutive series of patients with intracranial aneurysms, treated with the SVB between June 2018 and November 2018. Institutional Ethic Committees approved this study.
Clinical, intra/periprocedural, and angiographic data, including aneurysm size and location, device/s used, technical details, initial angiographic occlusion, and clinical data were analyzed.
Intra and periprocedural and complications were evaluated. Clinical outcome was evaluated prior to treatment and at discharge using the modified Rankin scale.
Forty-one consecutive patients (28 women and 13 men: age average 50.5 years) with 43 aneurysms were treated with SVB. table 1. All procedures were performed following written informed consent.
Baseline characteristics
Aneurysm sizes were classified by their maximum diameter, with an average size of 9.5 mm (range 2–30 mm). Thirty-four cases were unruptured. Of these, 24 cases were asymptomatic incidental, eight cases presented with headache, one patient had motor aphasia and seizures only, and one patient had homonymous hemianopsia. Five aneurysms previously ruptured and had recurrence after the initial coiling. There were two cases acutely treated with SVB after a subarachnoid hemorrhage (SAH): a case with three aneurysms located at a diplastic M2 superior branch of MCA and another case with a fetal PCom wide-necked aneurysm.
Platelet function tests were not mandatory and were performed in only 20/41 procedures, with no hiporesponders to aspirin and clopidogrel documented.
In 29 cases aspirin and clopidogrel were administrated prior to intervention, Eleven cases received aspirin and ticacrelor, and one case was intraoperative managed with Integrilin and continued with aspirin plus ticagrelor. Dual antiplatelet therapy was continued at discharge.
Available SVB sizes range from 2.25 to 3.25 mm diameters with lengths between 10 and 25 mm. The device has been designed for vessels from 1.5 to 3.5 mm in size.
SVB were deployed through a Headway 17 microcatheter (MicroVention, Tustin, CA, USA) in 35 cases, Vasco-17 (Balt, Montmorency, France) in five cases and one case with Echelon-10 (Medtronic Neurovascular, Irvine, CA, USA).
No cases were deployed through double lumen-balloons following manufacturer’s recommendations. Device deployment using a push-pull technique did not differ from the previous generation as previously reported.
While 13 cases were done using the triaxial system with intermediate catheters (Navien 058 (Medtronic Neurovascular, Irvine, CA, USA) (eight cases), Sofia 6F ((MicroVention, Tustin, CA, USA) (nine cases), Fargo Max (Balt, Montmorency, France) (three cases), and Benchmark((Penumbra, Alameda, CA) (one case), 20 procedures were done without intermediate catheters.
Any clinical events during the postoperative course were noted. Patients' demographics, aneurysm location, type of aneurysm (saccular, dissecting, fusiform), previous treatment, size, rupture status at presentation, degree of occlusion, and clinical and/or technical complications were noted.
Initial occlusion rates were graded according to the O’Kelly–Marotta (OKM) grading scale for assessment of cerebral aneurysms treated by flow diversion (considering aneurysm filling as: A total, B sub- total, C entry remnant, D no filling; and the degree of stasis into one arterial, two capillary, three venous phase).
Results
This series included 43 intracranial aneurysms located at the M1 segment (five cases), M2 segment (three cases), M3 segment (one case), middle cerebral artery (MCA) bifurcation (six cases), carotid-T (two cases), anterior communicating artery/A1/A2 (11 cases), pericallosal artery (four cases), supraclinoid ICA (two cases), PCom (one case), V4 segment (three cases), PCA (three cases), SCA (one case), and PICA (one case). Thirty aneurysms were saccular, five dissecting and eight fusiform/dysplastic. table 1
A total of 49 stents were deployed properly in the 41 cases, that is, an average of 1.19 devices per case in this series. All devices were placed properly and no devices needed to be removed. Among the 41 procedures, recapture and repositioning were performed in 12 cases. In three procedures the operators decided to recapture the device despite an initial full opening, in order to improve the wall apposition
The devices opened instantaneously in all cases but two: a case that required angioplasty for fully opening of the proximal-end (after recapture several times for reposition) and proximal-end ‘fish-mouth unopening’ in a fusiform SCA aneurysm which required a second overlapped device for a complete expansion.
Multiple SVB were used in six cases out of 41: In three cases two devices were overlapped for a better neck coverage after malposition of the first device. In another case mentioned above, two devices were overlapped after unopening (‘fish-mouth’) of the first implant. In the two cases of fusiform aneurysms, three devices were necessary to reconstruct the artery. Coadjuvant coiling were performed in 13 cases.
The stented parent vessels had an average diameter of 2.28 mm (range, 0.9–3.6 mm) proximally and 2 mm (range, 0.8–3.4 mm) distally. Fluoroscopy-time average was 34 min (range from 11 min to 139.8 min)
Intraprocedural events
We had five intraprocedural complications (table 2) which resolved without clinical consequences: one acute covered branch occlusion after stent deployment which resolved after increasing arterial pressure in a pericallosal aneurysm; one parent artery vasospasm in the M2 segment acute ruptured case; and one vasospasm in an unruptured AcoA, both solved with i.a nimodipine; one distal branch perforation with microwire while treating a pericallosal aneurysm which resolved spontaneously; and a clot formation in the case that angioplasty was needed for proximal-end opening, solved with the balloon plus i.v integrilin. There were no aneurysm rupture, dissections, nor stent thrombosis.
Intraprocedural complications
Periprocedural events
Three events were documented postprocedure. There was a central venous catheter infection requiring antibiotics in the ruptured MCA case, one heavy headache managed with steroids in a 15 mm saccular A1–A2 aneurysm, and one groin pseudoaneurysm resolved with compression.
Initial aneurysm occlusion rate
Intraoperative angiographic occlusion rate is summarized in table 3
Immediate angiographic results. O’Kelly–Marotta (OKM) grading scale
Immediately after stent deployment, eight cases (18.6%) of aneurysms were completely occluded (OKM score D), five aneurysms (11.6%) showed near-complete occlusion (OKM score C), four cases (9.3%) showed incomplete filling (OKM B), and 26 cases (60.4%) showed persisting filling (OKM A).
The median length of hospital stay was 4.7 days (range 2–32 days) The mRS score at discharge from the hospital did not change from the admission mRS score.
Discussion
The new SVB device is the lower-profile flow diverter available, deliverable through a 0,017’ microcatheter. Our preliminary results demonstrate the intra and periprocedural safety and technical success of the device.
Endovascular therapy has become the first-line treatment for most types of intracranial aneurysms, however, endovascular coiling can be challenging especially in wide-necked or complex aneurysms. The major drawback of endovascular therapy is the high rate of aneurysm recanalization.1
There is a significant number of data supporting the use of FD in intracranial aneurysms but most of them are retrospective case series of prospectively maintained databases, or studies mixing the use of different FDs which present with different properties.2 There are also studies presenting data on different locations of the aneurysm in the intracranial circulation.3 Moreover in 2017 Bescke et al reported the results of a five-year follow-up of complex internal carotid artery aneurysms treated with the Pipeline Embolization Device (PED) for uncoilable and failed aneurysms, and demonstrated that the aneurysm occlusion at angiographic follow-up was progressively increasing over time.8
The Silk Flow diverter received CE mark approval for clinical use in January 2008. The first-generation device was a closed cell, self-expanding stent made of 48 braided nitinol and four platinum microfilaments which provided 35%–55% metal coverage when expanded to its nominal diameter. It had a porosity of 45%–60% and a pore size of 110–250 mm. The platinum strands with two flared ends acted as radiopaque markers.6
Most of the technical complications associated with the first generation were related to the lower radial force, some of them with clinical consequences.
In 2010, Lubicz et al 9 published the first prospective study in 29 patients with 34 aneurysms. They reported two cases where the stent could not be delivered because of very high friction within the catheter and one device was removed after parent artery occlusion during the partial delivery. Four procedural complications were reported without clinical consequences: not fully expanded within a stenotic segment requiring a Winspang stent, one asymptomatic occlusion after a secondary dissection with the guiding catheter, an acute A2 occlusion in the AcoA aneurysm, and one acute stent occlusion in a giant partially thrombosed giant fusiform cavernous aneurysm. Of 26 treated patients' clinical outcome at discharge worsened in two patients. Also in 2010, Byrne et al10 published the first international multicenter registry in 70 patients, reporting difficulties in Silk deployment in 15 patients and parent artery thrombosis in eight procedures.
In 2012, Briganti et al11 published the larger retrospective series including 295 aneurysms, 151 treated with Silk. They showed 14 technical complications, five deployment failures, five incorrect positioning, and four instent clotting. Ischemic or thromboembolic events occurred in 13 patients (4.8%).
In 2017, Pumar et al12 published a retrospective multicenter analysis of 157 patients treated with the Silk device between 2008 and 2013, showing 6.3% of incorrect deployment. They reported unopening in eight cases, four leading in acute stent thrombosis.
In 2012, the second-generation, so-called Silk+, received the CE mark. The device was developed with flared ends, lower porosity, higher radial force, and eight platinum markers. Less technical complications were reported with Silk+ compared with the first generation. In 2015, Lubicz et al13 published their 5five-year experience in 58 patients with 70 aneurysms. They showed an immediate neurologic morbidity rate of 1.9%, no procedure-related mortality, and overall permanent neurologic morbidity of 5.5%. All clinical complications were reported in the subgroup of patients treated with the first generation.
Endovascular treatment using a flow diverter for aneurysms located beyond Willis or in small vessels is still in debate. In 2014, Martínez-Galdámez et al14 published a multicenter study of 25 patients of distal aneurysms treated with the Pipeline embolization device. They reported three technical complications with no clinical consequences: one acute branch occlusion resolved after increasing arterial pressure; one slow opacification of the inferior trunk of the MCA which resolved with an intrarterial reopro; and one focal subarachnoid hemorrhage secondary to distal perforation with the microwire during an exchange maneuver. Two minor clinical events (8%) and one major event (4%) occurred, and no mortality (0%) were reported.
In 2018, Cagnazzo et al15 published 17 distal anterior cerebral artery saccular aneurysms treated with flow-diverter stents (12 cases with PED, three with Silk+, and two with FRED). Three patients showed ischemic complications in the perioperative period and there were two major strokes related to stent thrombosis. Caroff et al16 reported less promising results in a retrospective review of 15 saccular MCA bifurcation aneurysms treated with FDs showing a procedure-related morbidity reaching 21%.
In a recent series of 42 patients treated with FRED JR devices deployed in small and distal vessels, the overall rate of ischemic complications was close to 11% and the incidence of ischemic events among patients with distal ACA was nearly 10%. No technical complications were described.17
In 2018 Yan et al4 conducted a meta-analysis which demonstrated that FD treatment of small vessel aneurysms was technically feasible and effective with a 70% complete occlusion rate. Procedure-related morbidity and mortality rates were 9% and 4% respectively.
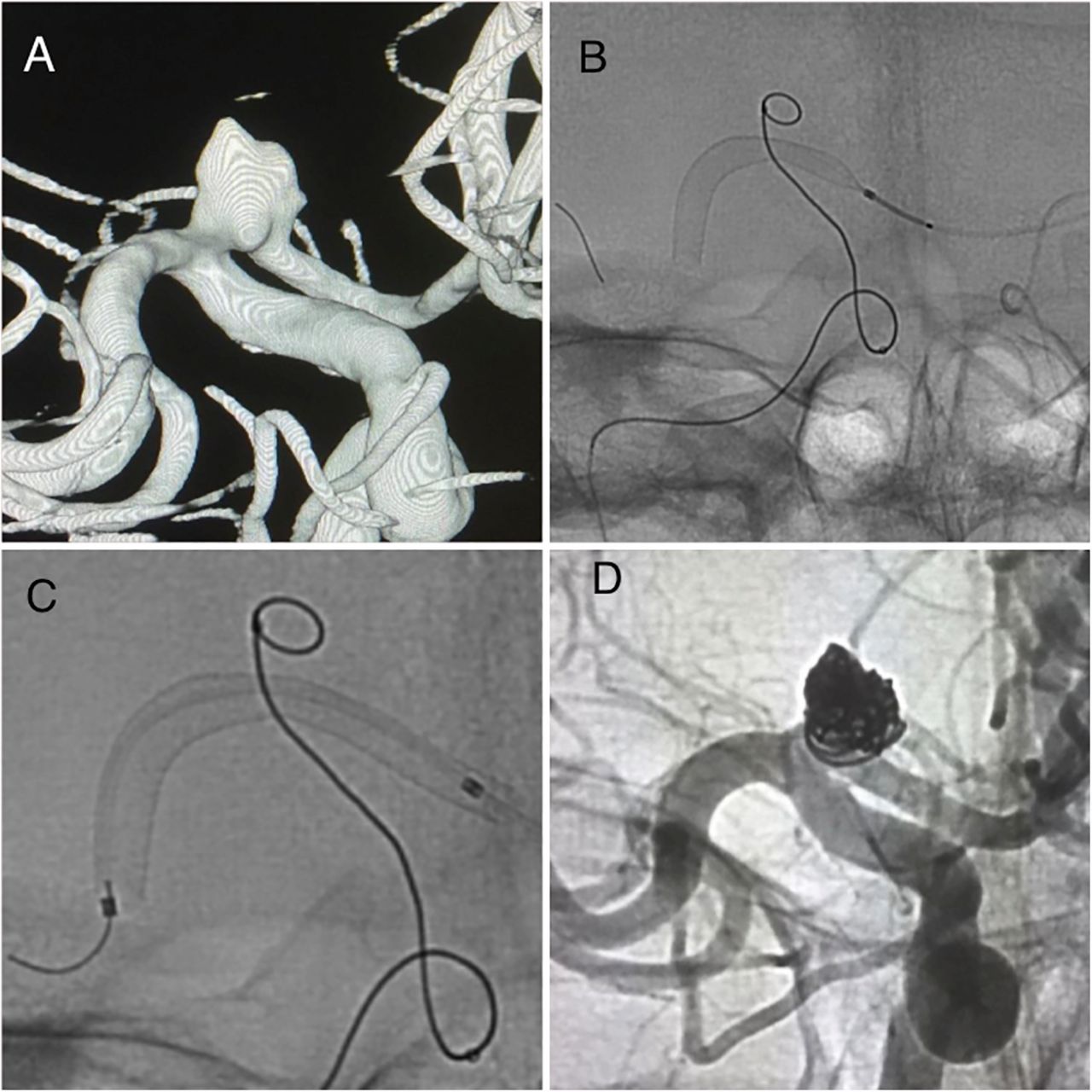
Recently, during 2018, the new lower-profile version of the device designed for small vessels, SVB, received the CE mark. The device has an improved design compared with its predecessors which makes the procedure technically easier related to several factors: visibility, trackability, and deployment. Despite this the device is nitinol made, all the wires have a platinum core (DFT) allowing a full visibility under fluoroscopy (figure 1). This is one of the main differences with its previous generations, where visibility was based on platinum wires. In our series, the stent full radiopacity was technically helpful which ensured the device apposition/opening, especially in curves, where braided stents may present unidentified flattening or unopening, and then preventing potential thromboembolic complications. Although the device is designed for vessels from 1.5 to 3.5 mm, in our series the parent artery diameter range from 0.9 to 3.6 mm with no clinical complications. No clinical neurological events were reported in the procedural and periprocedural periods. Despite most of the cases being located beyond Willis, intermediate catheters were used in around 50% of the cases and no exchange maneuvers were needed, factors which have been also reported as a potential source of complications during endovascular procedures.18

Unruptured 7 mm ICA bifurcation saccular aneurysm. (A) 3D reconstruction. Based on the anatomy, horizontal SVB deployment was selected. (B,C) Bilateral approach was done, with a jailed microcatheter for coadyuvant coiling. Horizontal SVB deployment was performed without the use of intermediate catheters. The implant was fully visible under fluoroscopy because of its 48 DFT wires. (D) Final run showing occlusion of the aneurysms and patency of the stent and covered branches.
A potential disadvantage of flow-diverter stents in the treatment of distal intracranial aneurysms is the use of larger and stiffer microcatheters with internal diameters of 0.021–0.027 inches into small-sized intracranial arteries. In order to avoid that, flow diversion with low-profile braided stents have been proposed as an alternative to FDs. In 2017 Aydin et al19 published a retrospective multicenter analysis of 20 aneurysms treated with the Leo Baby stent as monotherapy. They reported one case of unopening and stent thrombosis which required full removal in a dissecting/fusiform PICA aneurysm. The immediate angiographic results were one complete occlusion of one aneurysm (OKM grade D), three aneurysms with stagnated partial filling (OKM grade B2–3) (15%), and stagnated filling of 11 aneurysms (OKM grade A2–3) (55%).
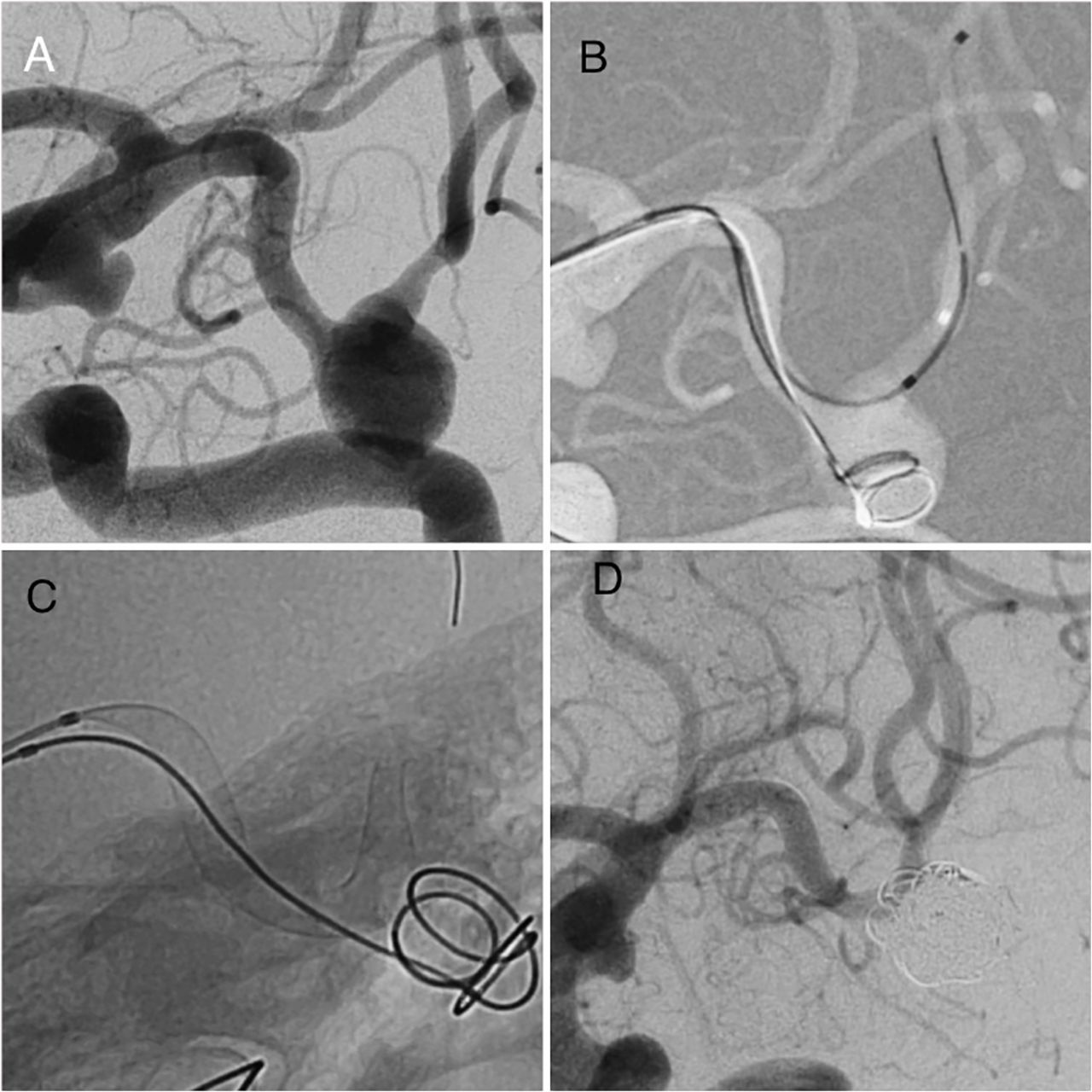
In our opinion, SVB combine the two main advantages of FDs and low-profile stents, in terms of occlusion rate and deliverability, respectively. Also because of the lower profile of the device, coadjuvant coiling were done in 13 cases without friction, without modifications on arterial angulation, and with an average fluoroscopy time of 34 min. figures 2 and 3.

DSA. (A) Unruptured 9 mm left MCA aneurysm, M1 segment. DSA. Small PCom aneurysm is also seen. (B,C) SVB assisted-coiling was achieved without friction. The device fully opened and is well adapted to the parent artery diameters. (D) Final run showing complete aneurysm occlusion with no complications.

{kind=link}
{kind=link}
{kind=link}
DSA and 3D reconstruction. (A,B) Unruptured 7 mm rounded fusiform PICA aneurysm. (C) A SVB device 2×15 mm opened fully despite the parent artery angulation. (D) Final run showing stagnation and a major intraneurysmal flow reduction.
The major limitations of our case series are the retrospective design and the limited follow-up. The results appear promising, but larger series with longer-term follow-ups are needed to corroborate the effectiveness of this treatment method and its superiority to other techniques.
Conclusions
Our study demonstrated that the use of the new low-profile flow diverter, SVB device, for the treatment of intracranial aneurysms is feasible and technically safe.
References
Footnotes
Contributors All authors have contributed to the concept, authorship, and final review of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Ethics approval Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.