Article Text

Abstract
Background Accurate assessment of the prevalence of large vessel occlusion (LVO) in patients presenting with acute ischemic stroke (AIS) is critical for optimal resource allocation in neurovascular intervention.
Objective To perform a systematic review of the literature in order to identify the proportion of patients with AIS presenting with LVO on image analysis.
Methods A systematic review was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines in order to identify studies reporting LVO rates for patients presenting with AIS. Studies that included patients younger than 18 years, were non-clinical, or did not report LVO rates in the context of a consecutive AIS series were excluded. Characteristics regarding presentation, diagnosis, and LVO classification were recorded for each paper.
Results Sixteen studies, spanning a total of 11 763 patients assessed for stroke, were included in the qualitative synthesis. The majority (10/16) of articles reported LVO rates exceeding 30% in patients presenting with AIS. There was substantial variability in the LVO definitions used, with nine unique classification schemes among the 16 studies. The mean prevalence of LVO was 31.1% across all studies, and 29.3% when weighted by the number of patients included in each study.
Conclusions Despite the wide variability in LVO classification, the majority of studies in the last 10 years report a high prevalence of LVO in patients presenting with AIS. These rates of LVO may have implications for the volume of patients with AIS who may benefit from endovascular therapy.
- stroke
- statistics
Statistics from Altmetric.com
Introduction
The incidence of acute ischemic stroke (AIS) remains high, and is among the most common causes of severe morbidity and mortality worldwide.1–3 The presence of a large vessel occlusion (LVO) in patients with AIS has been associated with significantly worse outcomes compared with those without occlusion of the proximal arteries.4 5 Due to suboptimal rates of recanalization following the administration of tissue plasminogen activator (tPA) in patients with LVO,6 7 resources have been quickly placed into the development of endovascular treatment as a tool for the treatment of LVO. Indeed, the advent of numerous randomized controlled trials demonstrating the efficacy of endovascular intervention has resulted in its adoption as the gold standard treatment for AIS patients presenting with LVO.8–14
Despite the critical role that LVO identification plays in both treatment selection and outcomes, there is very little agreement regarding the prevalence of LVO in patients presenting with AIS. Older studies rarely report the rates of occlusion for specific arteries,15 16 while newer investigations have been characterized by significant heterogeneity in LVO prevalence. More recently, several population-based studies have reported discrepancies between the estimated incidence of LVO and current thrombectomy volumes, thus highlighting the importance of accurate estimation in provider and hospital resource allocation.17 18
The purpose of this study was to perform a systematic review of the literature in order to assess the prevalence of LVO in patients presenting with AIS.
Methods
Search strategy
A systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.19 A search strategy was generated and employed using three computerized databases: PubMed, EMBASE, and Cochrane on June 8, 2017. The complete sequence used in the search was: (“stroke” or “cerebrovascular accident” or “CVA”) AND (“ischemic” OR “occlusion”) AND (“large vessel” or “great vessel” or “large artery”) AND (“acute” or “major”) AND (“scale” or “outcome” or “outcomes” or “instrument”). The complete genesis of search terms along with the number of corresponding references in each source is presented in table 1. A filter was used to identify articles published after 1 June 2007, thus generating studies conducted in the last 10 years.
Search terms used in the systematic review
Study selection
The title and abstract of each unique reference was examined for relevance to the research question. Studies that were deemed to be potentially relevant were subsequently examined via full-text review. Inclusion criteria consisted of (a) an adult population of patients presenting with AIS; (b) a clear definition of the arterial segments constituting LVO designation; (c) reported proportion of LVO within a consecutive series of AIS patients; and (d) original clinical research. Exclusion criteria included (a) studies reporting on patients with LVO outside a consecutive AIS cohort; (b) full-text article in a language other than English; and (c) a laboratory-based study or case report. In addition, all relevant full-text articles were examined for additional references that could be relevant to the study question.
Data extraction
Articles that met inclusion criteria were compiled and data pertaining to the characteristics of each study were subsequently collected. General information, including the year of publication, journal, number of analyzed AIS patients, and level of evidence was extracted. Additional variables pertaining to LVO, such as the definition of LVO, proportion of AIS patients with LVO, and the imaging modalities used in diagnosis were collected. When available, the time between the onset of symptoms and presentation was identified for the different case series. The characteristic of ‘acute’ stroke was attributed to patients who underwent assessment within 24 hours of the onset of symptoms consistent with cerebrovascular occlusion.
Results
Study inclusion
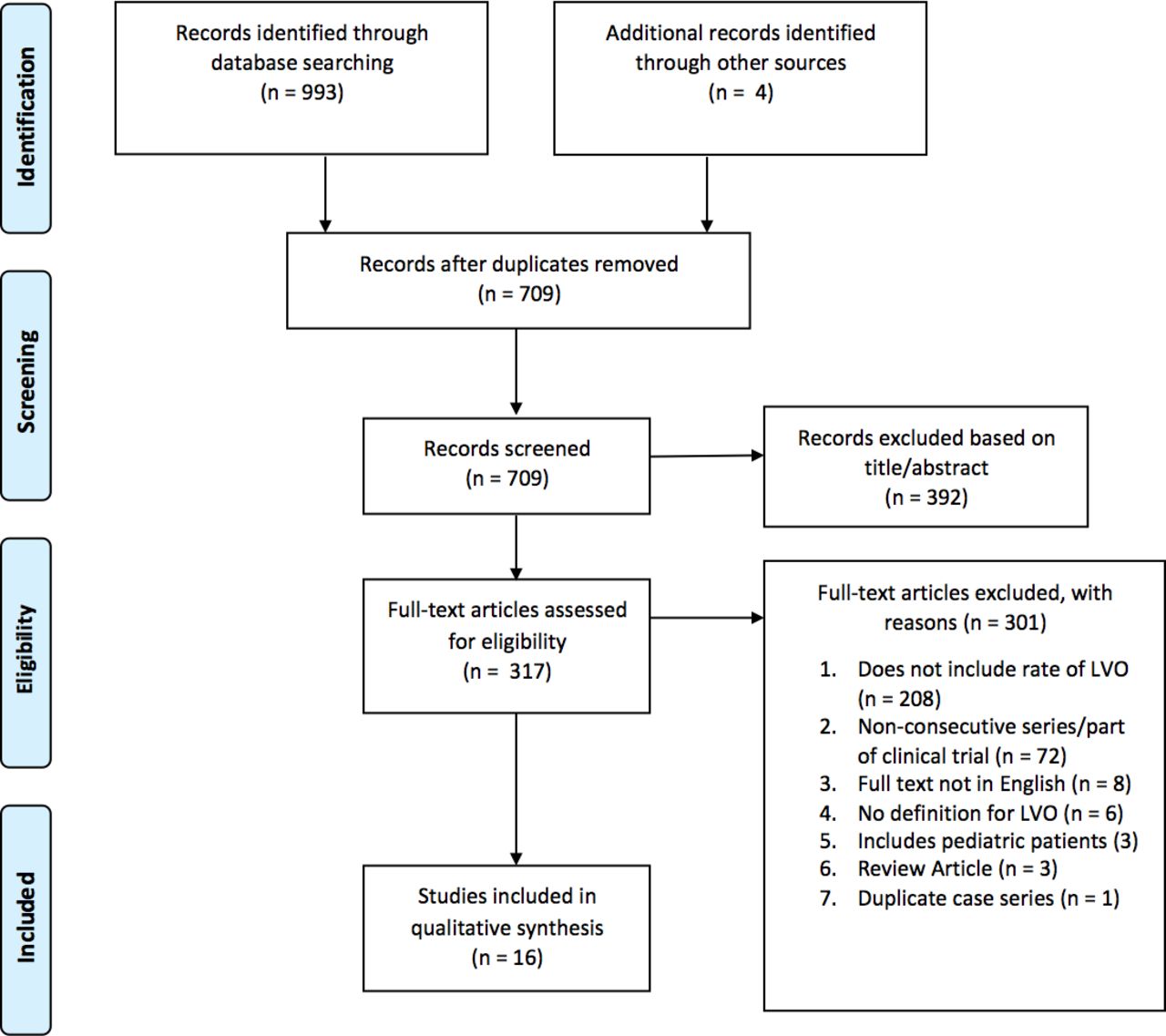
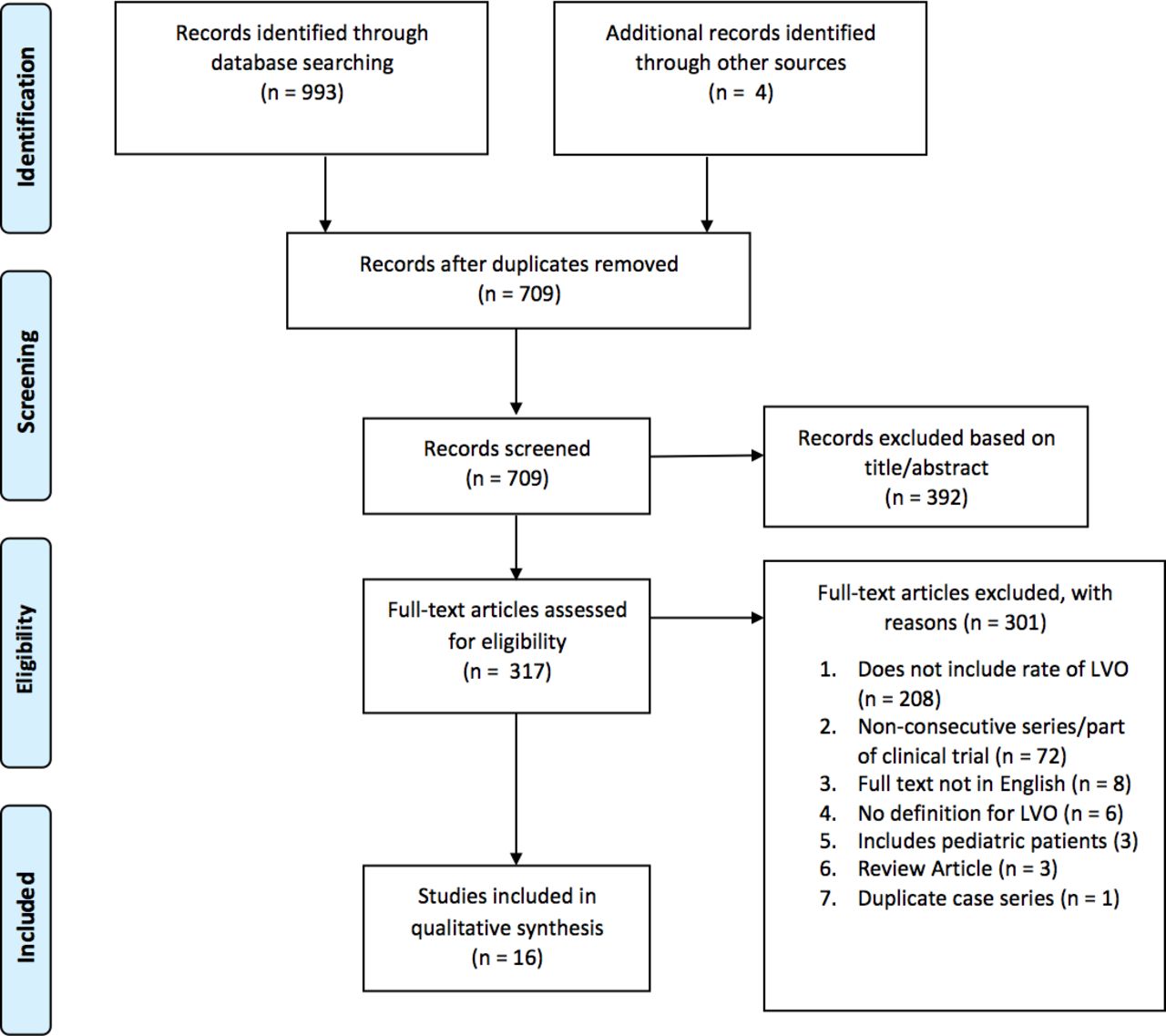
A total of 709 unique studies were identified, four of which were obtained via a manual review of the references. Of these, 392 were not deemed to be relevant based on title and abstract review. Full-text articles were excluded from this pool due to (a) lack of data pertaining to the proportion of patients with LVO (n=208), (b) a non-consecutive series or a cohort selected from a clinical trial (n=72), (c) a full-text article in a language other than English (n=8), (d) lack of a definition for LVO classification (n=6), (e) inclusion of pediatric patients (n=3), (f) a review article rather than original research (n=3), or (g) a duplicate case series. This resulted in a total of 16 studies included in the final qualitative synthesis. The complete PRISMA flow diagram is depicted in figure 1.
{kind=link}
PRISMA flow chart depicting the number of studies included at each stage of selection.
Study characteristics
The 16 studies spanned a total of 11 763 patients.5 17 20–33 Eleven investigations used prospectively collected data or registries, while five employed retrospective chart review. Nine articles were published since 1 January 2016 and seven studies were conducted between 2007 and 2016. A complete list of included articles along with the corresponding data is presented in table 2.
Characteristics of studies reporting the incidence of LVO in patients presenting with acute ischemic stroke
Definition of LVO
A total of nine unique classification schemes were used in the 16 papers. The most common definitions for LVO included the intracranial internal carotid artery (ICA), proximal middle cerebral artery (M1), distal middle cerebral artery territory (M2), or basilar artery (BA) as well as the combination of ICA, M1, or BA, each used in four different studies. Two studies defined LVO using ICA or M1,20 30 while the remaining six papers each had unique classifications.
Prevalence of LVO
The prevalence of LVO among patients with AIS ranged from 7.3% to 60.6% among the identified studies. Of the 17 groups of patients (Vanacker et al described both a derivation and validation cohort of AIS patients), the prevalence of LVO exceeded 25% in 13 (76.5%), 30% in 10 (58.8%), and 40% in 4 (23.5%) groups. The mean prevalence was 31.1% across all studies, and 29.3% when weighted by the number of patients included in each study.
Diagnostic modalities
Additional variation was observed in the image modalities used in the diagnosis of AIS and LVO. A total of eight (47.0%) groups of patients were diagnosed solely using CT angiography (CTA), seven (41.2%) were assessed via CTA or magnetic resonance angiography (MRA), one (5.9%) underwent CTA, MRA, or digital subtraction angiography (DSA), and one (5.9%) was diagnosed using CTA, MRA, or transcranial color-coded duplex sonography (TCCS).
Time to presentation
A total of seven (43.8%) studies reported on patients presenting within 6 hours following the onset of symptoms, two of which described time to presentation to be <4.5 hours. Two studies (12.5%) reported time to presentation to be within 24 hours following onset and one (6.3%) described patients who received imaging within 12 hours. The remaining articles included patients presenting at variable times following the onset of symptoms.
Discussion
The identification of AIS patients presenting with LVO has significant implications, not only in terms of functional status and post-treatment outcomes, but for the rapid triaging of patients who may be indicated for mechanical thrombectomy. Accurate estimation of the prevalence of LVO in patients with AIS is therefore important to the adequate distribution of provider and comprehensive stroke center resources. In this 10 year systematic review of the literature, the majority of the analyzed articles reported LVO rates exceeding 30%, thus highlighting a greater proportion of AIS patients who may potentially benefit from endovascular therapy than perhaps previously thought.
These high rates of LVO were reported across studies from both urban academic and rural medical centers, despite significant variability in study design as well as the definition of LVO. Given an annual estimated incidence of 691 650 AISs per year in the USA,34 rates of LVO exceeding 20% would represent substantially greater numbers of potentially thrombectomy-eligible patients than what is reflected by current procedural volumes. In a study of patients with AIS, Rai et al used institutional data to compute an LVO rate of 11%, and population analyses to estimate a national incidence of 77 569 new LVOs each year.17 The authors subsequently emphasized that the disparity between current procedural volumes and these estimates reflected a potential 2–5-fold increase in annual thrombectomy volumes. Given the more stringent LVO definitions used by the authors (ICA, M1, and BA), coupled with the low rate of LVOs compared with the majority of other studies in the literature, the disparities between the number of patients with LVOs and those undergoing endovascular therapy may be even greater than previously reported.17 In addition, the authors included cases of transient cerebral ischemia among the patients defined to have experienced ischemic stroke, which may have further contributed to the relatively decreased percentage of LVOs. These findings reflect the need for a more standardized approach to reporting LVO definitions and inclusion criteria in patients with AIS in order to facilitate the design of instruments to predict these occlusions and allow for better generalizability of regional LVO estimates. In addition, further studies pertaining to AIS treatment in the context of treatment setting (eg, rural hospital, urban quaternary care center) would facilitate these analyses. Another review examining studies reporting on patients with AIS recently reported the rate of LVO to be 38.7%, with 21.4% of patients with AIS potentially benefiting from thrombectomy therapy.35 However, the authors sought to assess rates of LVO in the context of stroke-related disability/death, and thus only included studies with Rankin scale data (n=2).
This qualitative synthesis additionally reflects the wide variety of approaches in the investigation of patients with suspected AIS. Fewer than half of the analyzed cohorts reported all of their patients undergoing CTA, with several studies describing the use of DSA and TCCS. Given the variation in the sensitivity and specificity of CTA, MRA, and TCCS in detecting different areas of occlusion,36–38 the use of varying modalities introduces additional challenges in the extrapolation of LVO volumes to other facilities. In addition, the differences in time to presentation following the onset of stroke symptoms may introduce concurrent variation that creates further difficulties in applying these LVO values to procedural volumes.
These findings should be considered in the context of their limitations. First, the inherent heterogeneity in study design precludes the ability to perform a comprehensive meta-analysis in order to gain statistical power in LVO assessment. Several studies, for example, analyze prospective registries that include patients who were specifically transferred from outside facilities, thereby potentially increasing the rate of diagnosed LVOs. Other investigations purposely exclude patients who were referred, while numerous others make no mention of this in their description of study methodology. Cumulative rates of LVO across the different studies should thus be interpreted with caution. Second, LVO volumes may not always reflect the population of patients eligible for thrombectomy. Other factors, such as the amount of salvageable brain, comorbidity burden, and functional status at baseline influence the decision to proceed with treatment.17 39 Finally, this represents a compilation of retrospective analyses over the last 10 years. Future studies representing higher levels of evidence would help provide stronger estimates of the prevalence of LVO.
Conclusions
These data demonstrate that, despite institutional variability in definitions and reporting methodology limiting the precision of estimates, the prevalence of LVO among patients with AIS is greater than previously thought. A larger proportion of stroke patients with LVO has implications for the effective allocation of hospital and provider resources for improving access in this high-risk group. Increased standardization of LVO classification would facilitate the development of predictive instruments and epidemiologic estimates for these patients.
References
Footnotes
Contributors NL designed the study, collected data, wrote the statistical analysis plan, drafted and edited the manuscript, and is the guarantor. MD, KC, IPS, ST, JTF, and JL collected data and edited the manuscript. JM designed the study, collected data, and edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KC is employed at Imperative Care, which is developing products for stroke treatment. JM is a consultant for The Stroke Project, Rebound Therapeutics, Viseon, Pulsar, Cerebrotech, Endostream, Vastrax; and an investor in Cerebrotech, The Stroke Project, Endostream, Apama, Rebound, Viseon, Neurvana, Cardinal Consulting, BlinkTBI, Serenity, NeuroTechnology Investors.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.