Article Text

Abstract
Background Few data are available regarding the safety and efficacy of antiplatelet (APT) pretreatment in acute ischemic stroke (AIS) patients with emergent large vessel occlusions (ELVO) treated with mechanical thrombectomy (MT). We sought to evaluate the association of APT pretreatment with safety and efficacy outcomes following MT for ELVO.
Methods Consecutive ELVO patients treated with MT during a 4-year period in a tertiary stroke center were evaluated. The following outcomes were documented using standard definitions: symptomatic intracranial hemorrhage (sICH), successful recanalization (SR; modified TICI score 2b/3), mortality, and functional independence (modified Rankin Scale scores of 0–2).
Results The study population included 217 patients with ELVO (mean age 62±14 years, 50% men, median NIH Stroke Scale score 16). APT pretreatment was documented in 71 cases (33%). Patients with APT pretreatment had higher SR rates (77% vs 61%; P=0.013). The two groups did not differ in terms of sICH (6% vs 7%), 3-month mortality (25% vs 26%), and 3-month functional independence (50% vs 48%). Pretreatment with APT was independently associated with increased likelihood of SR (OR 2.18, 95% CI1.01 to 4.73; P=0.048) on multivariable logistic regression models adjusting for potential confounders. A significant interaction (P=0.014) of intravenous thrombolysis (IVT) pretreatment on the association of pre-hospital antiplatelet use with SR was detected. APT pretreatment was associated with SR (OR 2.74, 95% CI 1.15 to 6.54; P=0.024) in patients treated with combination therapy (IVT and MT) but not in those treated with direct MT (OR 1.78, 95% CI 0.63 to 5.03; P=0.276).
Conclusion APT pretreatment does not increase the risk of sICH and may independently improve the odds of SR in patients with ELVO treated with MT. The former association appears to be modified by IVT.
- stroke
- thrombectomy
Statistics from Altmetric.com
Introduction
Mechanical thrombectomy (MT) with or without intravenous thrombolysis (IVT) pretreatment is the current standard of care for patients with acute ischemic stroke (AIS) with emergent large vessel occlusions (ELVO) with and without contraindications to IV tissue plasminogen activator (tPA).1 2 Although several factors affect clinical outcomes following MT for ELVO, successful recanalization represents the strongest independent predictor of a favorable functional outcome.3 Efficacy of recanalization may depend on thrombus composition, which is a mixture of fibrin/platelets, red blood cells, and white blood cells.4 5 Thrombi with lower density on non-contrast CT scan have been shown to be more resistant to pharmacological lysis and MT.5 Prior use of antiplatelet (APT) medications, especially aspirin, may affect clot composition and potentially improve recanalization rates in patients with ELVO treated with MT.6 7
On the other hand, there are contradictory data regarding the association of APT pretreatment with safety and efficacy outcomes of patients with AIS treated with systemic thrombolysis. More specifically, several observational studies have reported increased risk of symptomatic intracranial hemorrhage (sICH) following IVT in patients with AIS with prior APT use.8–11 Nevertheless, two recent meta-analyses independently reported that APT pretreatment in patients with AIS treated with IVT is not associated with higher odds of sICH after adjustment for potential confounders including age, stroke severity, and comorbidities.12 13 Theoretically, it may be argued that pre-hospital use of APT may increase the risk of sICH following MT especially in patients with ELVO pretreated with IVT. The limited data evaluating the relationship of APT pretreatment with early outcomes of patients with ELVO treated with MT prevents the reliable evaluation of the risks and benefits of pre-hospital use of APT in the evolving era of endovascular reperfusion therapies for AIS.
In view of the former considerations, we sought to evaluate the relationship of prior APT use with early efficacy and safety outcomes in patients with ELVO treated with MT. We also evaluated the potential effect of IV tPA pretreatment on different outcome measures after MT in patients with ELVO with APT pretreatment.
Methods
Study population
We performed a retrospective analysis of a prospectively collected database of consecutive patients with ELVO treated with MT at a tertiary care stroke center during a 4-year period (from January 2012 to January 2016).14–16 We included patients with AIS with CT angiography (CTA)-confirmed large vessel occlusions who presented within 6 hours of symptom onset and underwent MT. For patients presenting between 6 and 12 hours from symptom onset, additional imaging selection criteria were used such as Alberta Stroke Program Early CT Score (ASPECTS) ≥6 on CT head and/or good collaterals on CTA.15 CT and CTA were performed on a 64-slice scanner. CT slice thickness was 1.25 mm with acquisitions in axial, sagittal, and coronal planes with 3D reformations. ASPECTS and CTA collateral scores were calculated as previously described.17 18 Collateral scores were reported in a dichotomized fashion (good vs poor collaterals) for LVO using a methodology that has been shown to predict clinical outcome.18
Definition of baseline characteristics
Stroke severity at hospital admission was documented using the National Institutes of Health Stroke Scale (NIHSS) score by certified vascular neurologists. Baseline characteristics including demographics, vascular risk factors, pre-hospital use of APT, admission NIHSS scores, admission ASPECTS, pretreatment with IVT, admission serum glucose, admission systolic and diastolic blood pressure levels were recorded as previously described.16 19 APT use prior to hospitalization was self-reported by patients or families and verified by the pharmacy. At our center, pharmacy department personnel always verify the prescribed medication and the last refill with the patient’s pharmacy, and also check with the patient and cross-verify with the family members about administration of medications. Location of the occlusion was categorized as follows15–18: anterior versus posterior circulation occlusion, tandem occlusions (yes vs no), proximal occlusion (yes vs no). Proximal occlusion was defined as internal carotid artery (ICA) or basilar artery occlusion in the anterior and posterior circulation, respectively. Tandem occlusion was defined as simultaneous presence of both intracranial and extracranial arterial occlusions in the distribution of AIS. Diagnosis of the tandem occlusion was made via catheter angiography.
Definition of outcomes
The following safety outcomes were documented using standard definitions13 19 previously described by our group: sICH and 3-month mortality. More specifically, sICH was defined as the presence of a parenchymal hematoma type 2 on brain CT and/or MRI gradient recall echo sequence accounting for deterioration with an increase in NIHSS score of ≥4 points within 36 hours from treatment.20
The following efficacy outcomes were also documented as previously described: successful recanalization, functional independence, and functional improvement at 3 months. Successful recanalization at the end of the endovascular procedure was defined by modified Thrombolysis in Cerebral Infarction (mTICI) grades 2b or 3, which were obtained from the reports of endovascular specialists (LE, AA, and DH).15 Functional outcome was evaluated at 3 months using the modified Rankin Scale (mRS) scores by certified vascular neurologists. Functional independence was defined as mRS scores of 0–2.14 Functional improvement was assessed by the shift in the distribution of 3-month mRS scores.14 The mRS scores were obtained in person either from a post-hospital discharge clinic follow-up or from a hospital visit.14 Endovascular specialists grading the degree of reperfusion at the end of MT and vascular neurologists assessing NIHSS and mRS scores were unaware of the purposes of the study and performed treatments and assessments as part of their clinical duties. The study was approved by the institutional review boards of the participating centers (10–01003-XP).
Statistical analysis
Continuous variables are presented as mean±SD (normal distribution) and as median with IQR (skewed distribution). Categorical variables are presented as percentages with their corresponding 95% CIs. Statistical comparisons between the two groups (prior APT use vs no APT use) were performed using the χ2 test or, in the case of small expected frequencies, the Fisher’s exact test. Continuous variables were compared using the unpaired t-test or Mann–Whitney U test, as indicated. The distributions of the mRS scores at 3 months among patients with ELVO with and without APT pretreatment were compared using the Cochran–Mantel–Haenszel test. Furthermore, the associations of prior APT use with different binary outcomes (eg, 3-month Favourable Functional Outcome (FFO), recanalization, mortality, sICH) were assessed using univariable and multivariable logistic regression models adjusting for potential confounders. In multivariable analyses we tested the statistical significance hypothesis under the likelihood ratio test with a P value of <0.05. We reported all associations as ORs with their corresponding 95% CIs. Multivariable logistic regression analyses were conducted using the backward selection procedure. Finally, we evaluated the interaction of IVT pretreatment on the association of pre-hospital use with early outcomes of ELVO patients treated with MT. The Statistical Package for Social Science (SPSS) V.22.0 for Windows was used for statistical analyses.
Results
Our study population consisted of 217 patients with AIS due to ELVO (mean age 62±14 years, 50% men, median NIHSS score 16 (IQR 12–21)) treated with MT. Intracranial atherosclerotic disease was present in 70 cases (32%). In our cohort, a combination of distal aspiration and stent-retriever was used as the most common technique in 115 cases (53%). Successful recanalization was achieved in 67% of the study population. sICH occurred in 14 patients (6.5%), while the 3-month functional independence and mortality rates were 45% and 26%, respectively. Three-month mRS scores were available in 91% (n=198) of the study population.
Out of 217 patients, 146 (67.3%) were not on any APT therapy prior to hospitalization. The remaining 71 patients (32.7%) were pretreated with the following APT agents: 56 (25.8%) with aspirin, 2 (1%) with clopidogrel, 12 (5.5%) with a combination of aspirin and clopidogrel, and 1 (0.5%) with a combination of aspirin and dipyridamole. Table 1 compares the baseline characteristics of ELVO patients with and without APT pretreatment. Patients with APT pretreatment had more vascular risk factors (hypertension, diabetes, and hyperlipidemia) than the APT-naïve group.
Baseline characteristics of the study population stratified by antiplatelet pretreatment
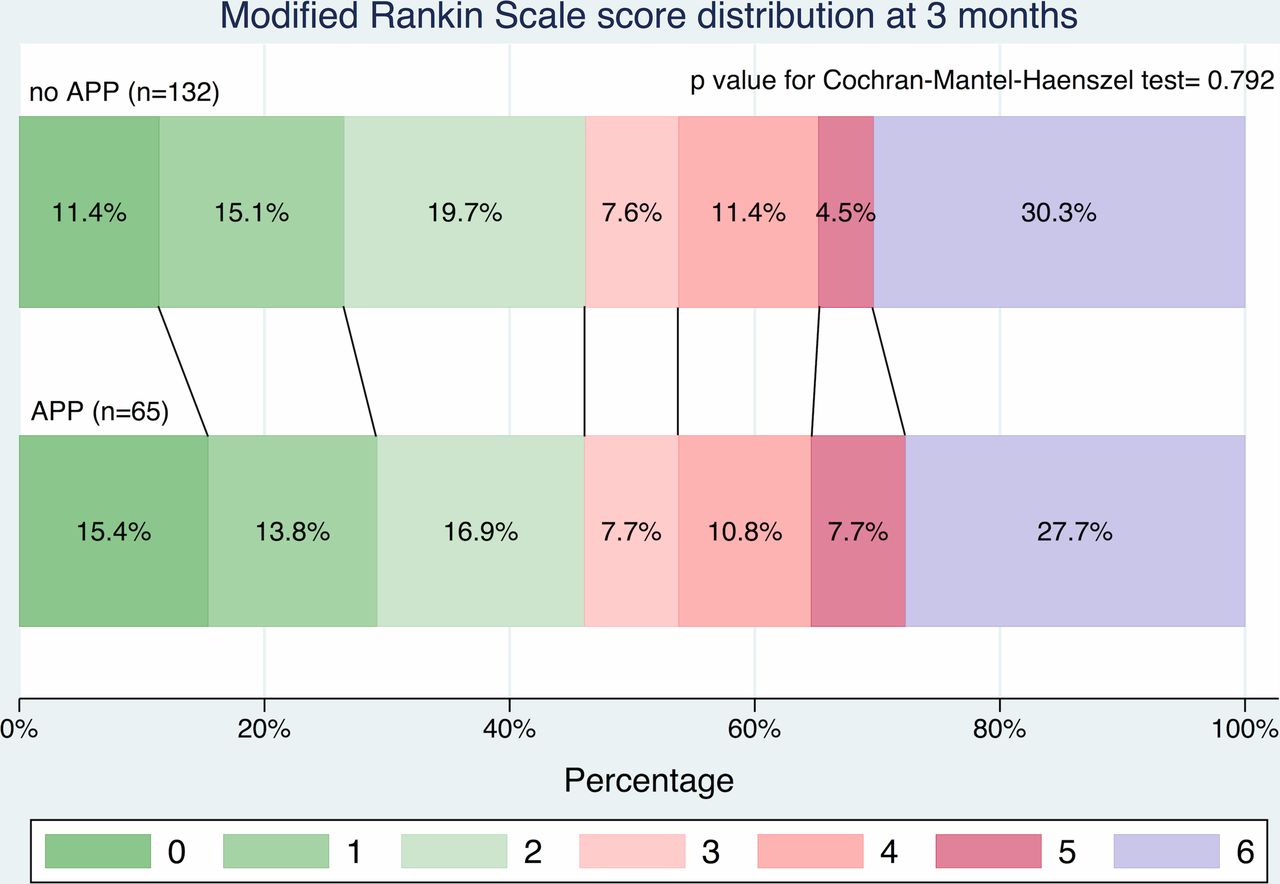
Table 2 shows comparisons of safety and efficacy outcomes in patients with and without APT pretreatment. Patients pretreated with APT had higher rates of successful recanalization (77% vs 61%; P=0.013). The two groups did not differ (P>0.8) in terms of sICH, 3-month mortality, 3-month functional independence, and 3-month functional improvement (figure 1). The median (IQR) time from groin puncture to recanalization was similar in patients with and without APT pretreatment (51 (32–57) min and 48 (35–80) min, respectively; P=0.497). Additionally, there was no significant difference in rates of sICH between pre-hospital use of aspirin and dual APT (5.4% vs 8.3%; P=0.703).
Univariable associations of safety and efficacy outcomes in patients with emergent large vessel occlusion (ELVO) with or without prior antiplatelet use
{kind=link}
Association of antiplatetet pretreatment (APP) with functional improvement at 3 months according to the shift in the distribution of the modified Rankin Scale scores. Comparison between groups was performed using the Cochran–Mantel–Haenszel test.
Table 3 depicts the associations of all baseline characteristics with successful recanalization in univariable and multivariable binary logistic regression analyses. In the initial univariable analyses, the following three variables were selected for inclusion in the final multivariable model: APT pretreatment, good collateral status, and higher baseline ASPECTS. The association of APT with successful recanalization was the only one that retained its significance in the multivariable logistic regression model. More specifically, APT pretreatment was independently associated with increased likelihood of successful recanalization (OR 2.18, 95% CI 1.01 to 4.73; P=0.048) after adjustment for potential confounders.
Univariable and multivariable logistic regression analyses of the associations of antiplatelet pretreatment and other baseline characteristics with the probability of complete reperfusion (defined as Modified Thrombolysis in Cerebral Infarction grades 2b or 3) following mechanical thrombectomy in patients with emergent large vessel occlusion
We detected a significant interaction (P=0.014) of IV tPA on the association of pre-hospital APT use with successful recanalization. APT pretreatment was associated with higher odds of successful recanalization (OR 2.74, 95% CI 1.15 to 6.54; P=0.024) in the subgroup of patients treated with combination therapy (IVT and MT), but not in patients treated with direct MT (OR 1.78, 95% CI 0.63 to 5.03; P=0.276). The rates of successful recanalization in APT-pretreated patients with ELVO receiving combination therapy and those receiving direct MT were 83% and 63%, respectively. Finally, there was no interaction of pretreatment with IVT on the association of pre-hospital APT use with sICH (P=0.519), 3-month mortality (P=0.641), and 3-month functional independence (P=0.240).
Discussion
Our study showed that the pre-hospital use of APT was associated with higher rates of successful recanalization in patients with ELVO treated with MT. This association was independent of demographics, vascular risk factors, baseline stroke severity, onset to groin puncture time, location of occlusion, admission blood pressure and serum glucose levels, IVT pretreatment, onset to groin puncture time, and early hypodensity on brain CT quantified by ASPECTS and collateral status. APT pretreatment did not increase the risk of sICH and 3-month mortality, but also was not related to functional improvement or functional independence at 3 months. Additionally, the association of the pre-hospital use of APT with increased likelihood of successful recanalization appeared to be modified by IVT. APT pretreatment increased the odds of successful recanalization in patients with ELVO treated with combination therapy but not in those treated with direct MT.
The findings of our study are corroborated by observations of a retrospective analysis showing that APT pretreatment was related to higher rates of early recanalization assessed by transcranial Doppler or digital subtraction angiography in patients with ELVO treated with IVT monotherapy.7 The rate of successful recanalization associated with APT pretreatment increased from 40% following IV tPA alone in the study by Sanak et al 7 to 63% in patients with direct MT and 83% with combination therapy (IVT and MT) in our cohort.
Several pathophysiological mechanisms may account for the observed relationship between APT pretreatment and the increased successful recanalization rate following MT for ELVO. First, APT therapies—and aspirin in particular—have been shown to alter the clot structure in vitro, resulting in the formation of clots with thicker fibers and bigger pores allowing better entanglement of erythrocytes and raising the efficacy of thrombolysis.21–23 Second, prior APT use makes the endothelial surface smoother and decreases tissue factor expression, which contributes to easier removal of clot and decreased subsequent thrombosis, respectively.24 Additionally, aspirin may interfere with inflammatory and immunological processes that contribute to thrombus formation and, importantly, the white blood cell fraction within the thrombus.6 25 Moreover, the platelet-enriched clots can lead to formation of large platelet aggregates within the fibrin network resulting in increased clot rigidity and delayed tPA-induced clot lysis.26 27 Finally, APT pretreatment may prevent early reocclusion following initial recanalization and reduce the odds of deterioration following clinical improvement.28
Notably, in the present study, patients with ELVO with prior use of APT were more likely to have vascular risk factors (hypertension, diabetes or hyperlipidemia) compared with APT-naïve patients, which can be explained by more extensive primary or secondary prevention of vascular risk factors in terms of APT use. However, these vascular risk factors were included in the multivariable model as potential confounders and did not affect the association of APT pretreatment with the increased likelihood of successful reperfusion following MT.
Our study provides further evidence regarding the safety of APT pretreatment in patients with AIS receiving systemic7 12 29 or endovascular reperfusion therapies. Pre-hospital APT use was not related to increased risk of sICH in our cohort. Our experience contradicts the findings of a recent Japanese study that reported prior APT use as an independent predictor of sICH after MT in patients with ELVO.30 However, the majority of patients with ELVO in this study underwent MT with older generation devices (MERCI retrievers) that are known to be associated with higher rates of sICH compared with newer generation devices.30 Moreover, intra-arterial thrombolysis was delivered in addition to MT in 21% of the Japanese cohort, and this may have confounded the reported association between APT pretreatment and risk of sICH. Consequently, our findings are not directly comparable to this study due to differences in study populations (Caucasians/African-Americans vs Asians), endovascular devices, and concomitant reperfusion therapies (intra-arterial thrombolysis). Further validation of our preliminary findings regarding the safety of APT pretreatment in patients with ELVO treated with MT is required in larger multi-ethnic cohorts treated with new generation devices, given the increasing concerns that pre-hospital APT use may increase the risk of symptomatic intracranial bleeding especially in ELVO patients treated with combination reperfusion therapies.31 32 Considering the fact that we did not document any increase in sICH rates and demonstrated improved recanalization rates with pre-hospital APT use in patients with ELVO, it would be interesting to evaluate the potential role of glycoprotein IIb/IIIa inhibitors (eg, abciximab) for the periprocedural management of these patients. This hypothesis is further supported by a recent study demonstrating that, in acute tandem extracranial ICA/MCA or tandem extracranial ICA/terminal ICA occlusions, extracranial stenting followed by intra-arterial abciximab and MT is feasible, effective, and safe.33
In our cohort, improvement in recanalization rates seen with prior APT use did not translate into improved functional outcomes, probably because of the moderate sample size. Moreover, the interaction of IVT pretreatment on the relationship of pre-hospital APT use with increased successful recanalization rates may have contributed to the lack of association between APT pretreatment and improved clinical outcomes, since more than one-third of our cohort (35%) were treated with direct MT.
Several limitations of the present study need to be acknowledged. First, the modest sample size and retrospective analysis of prospectively collected data are important methodological shortcomings. Second, our methods included safety and efficacy outcomes lacking central adjudication. Third, the small sample size prevented us from doing additional subgroup analysis for patients with ELVO pretreated with dual APT therapies. Fourth, we did not document reocclusion rates and thus are unable to assess the potential relationship of APT pretreatment with the likelihood of reocclusion. Fifth, APT use prior to hospitalization was self-reported by patients or families and verified by the pharmacy. Nevertheless, medication compliance could not be systematically evaluated and this concern should be taken into account when interpreting our study findings. Sixth, we did not collect data on peri-procedural blood pressure recordings, which could be an important confounding factor that may moderate the association of pre-hospital APT use with increased likelihood of successful reperfusion and sICH. Finally, the issue of selection of more appropriate outcome measures that could be more granular and reflective of antiplatelet effect (eg, number of passes needed to achieve reperfusion, histopathological analysis of clot density of retrieved thrombi) needs to be highlighted as a potential methodological shortcoming of this study. Unfortunately, these data were unavailable in our registry and the associations of APT pretreatment with these outcome measures were not evaluated.
Also, it is important to note that pre-hospital APT use was associated with successful recanalization (OR 2.74, 95% CI 1.15 to 6.54; P=0.024) in patients treated with combination therapy (IVT and MT) but not in patients treated with direct MT (OR 1.78, 95% CI 0.63 to 5.03; P=0.276). Since APT pretreatment was not related to higher recanalization rates in the direct MT subgroup, it is possible that thrombectomy techniques (stent-retrievers vs aspiration monotherapy) did not confound the reported associations. In our cohort, a combination of distal aspiration and stent-retriever was used as the most common technique in 115 cases (53%), while aspiration alone was used in only 50 patients. Given the limitations in sample size, we consider it inappropriate to conduct further subgroup analyses to detect a potential differential effect of APT pretreatment on successful recanalization according to the different thrombectomy techniques. Therefore, larger studies are needed that should also investigate the potential interaction of MT devices on the association between APT pretreatment and increased likelihood of successful reperfusion in patients with ELVO treated with MT.
In conclusion, pre-hospital APT use does not increase the risk of symptomatic intracranial bleeding and may independently improve the odds of successful recanalization in patients with ELVO treated with MT. The former association appears to be modified by IVT pretreatment, with significantly higher rates of successful recanalization in APT-pretreated patients receiving combined systemic and endovascular reperfusion therapies.
References
Footnotes
Contributors AP: Study concept and design, acquisition of data, analysis and interpretation, and critical revision of the manuscript for important intellectual content. GT: Analysis and interpretation and critical revision of the manuscript for important intellectual content. RK, MFI: Acquisition of data and critical revision of the manuscript for important intellectual content. SS, DH, ASA, CN, AA, LE: Critical revision of the manuscript for important intellectual content. NG: Study concept and design, acquisition of data, critical revision of the manuscript for important intellectual content, study supervision.
Competing interests None declared.
Ethics approval University of Tennessee IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Presented at A portion of this study’s findings has been presented at the Society of Neurointerventional Surgery Annual Meeting, 2016.