Article Text

Abstract
Background Optimal technical approaches of large-vessel anterior circulation acute ischemic strokes with concomitant extracranial internal carotid artery tandem occlusions is controversial.
Purpose This systematic review and meta-analysis evaluates: the overall outcomes of patients with tandem occlusions treated with second-generation mechanical thrombectomy devices; differences in outcomes of extracranial versus intracranial first approaches; and differences in outcomes of extracranial stenting at time of procedure versus angioplasty alone.
Methods MEDLINE, EMBASE, and the Web of Science was searched through September 2017 for studies evaluating patients presenting with acute tandem occlusions of the extracranial ICA and intracranial ICA, and/or proximal MCA treated with second-generation mechanical thrombectomy devices. Outcomes were pooled across studies using the random-effects model and expressed as cumulative incidence (event rate) and 95% CI.
Results Thirty-three studies were included in analysis. Overall mRS≤0–2 at 90 days was 47% (95% CI 42% to 51%). No statistical difference was seen in 90-day mRS≤0–2 for patients treated with extracranial versus intracranial first approaches, 53% (95% CI 44% to 61%) vs 49% (95% CI 44% to 57%) (P=0.58). No statistical difference was seen in 90-day mRS≤0–2 for patients treated with extracranial stenting versus angioplasty alone, 49% (95% CI 42% to 56%) vs 49% (95% CI 33% to 65%) (P=0.39). No other statistical differences in outcome or safety were identified.
Conclusions Nearly half of all tandem occlusion patients treated with mechanical thrombectomy have good neurological outcomes. No statistical differences in outcome are identified between extracranial first versus intracranial first approaches, nor extracranial stenting versus angioplasty alone.
- stroke
- thrombectomy
- stent
- thrombolysis
- technique
Statistics from Altmetric.com
Introduction
Tandem occlusions (TOs) involving occlusion of the cervical internal carotid artery (ICA) and concomitant intracranial large-vessel occlusion (LVO) of either the intracranial ICA and/or proximal middle cerebral artery (MCA) have poor response to IV thrombolysis alone,1 and are known to be a predictor of poor outcome after thrombolysis.2 In recent years, endovascular thrombectomy has become the standard of care in treating large-vessel anterior acute ischemic stroke (AIS),3 though most positive trials do not specifically evaluate patients with concomitant stenosis of the extracranial circulation.4
Optimal treatment strategies in this scenario are controversial. First, it remains unclear if intracranial or extracranial lesions should be treated first. Proponents of the intracranial first approach argue in favor of reduced time to recanalization, while proponents of the extracranial first approach argue in favor of improved collateralization while the intracranial thrombectomy is being performed. Second, it remains unclear if extracranial lesions are best managed with stenting or angioplasty only at the time of initial treatment. Proponents of the carotid stenting approach argue in favor of a definitive treatment at time of initial procedure, while proponents of the angioplasty-only approach argue that the necessary antiplatelet regimen following carotid stenting inappropriately increases the risk of periprocedural hemorrhage. As a consequence, there has been diversity in the proposed endovascular approaches of tandem occlusions including: intracranial mechanical thrombectomy (MT) alone; intracranial MT followed by angioplasty and/or stenting of the ICA occlusion; and angioplasty and/or stenting of the ICA occlusion followed by intracranial MT.5 In order to better understand outcomes of various treatment strategies for patients with tandem occlusions, we performed a systematic review and meta-analysis for the purposes of evaluating: the overall outcomes of patients with tandem occlusions treated with second-generation mechanical thrombectomy devices; differences in outcomes of patients with extracranial treatment first compared with intracranial treatment first approaches; and differences in outcomes in patients treated with extracranial stenting at time of procedure compared with patients treated with angioplasty alone.
Methods
Literature search
This systematic review is reported according to the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analysis). A comprehensive literature search of Ovid MEDLINE, Ovid EMBASE, and the Webs of Science from January 2007 through September 2017 was performed to identify studies evaluating patients presenting with acute tandem occlusions of the extracranial ICA and intracranial ICA, and/or proximal MCA treated with endovascular thrombectomy. Initial search terms were: tandem occlusion, internal carotid artery occlusion, mechanical thrombectomy, stroke, and large-vessel occlusion. We also searched references from included studies to identify additional eligible studies.
Identified studies from the literature search were then further evaluated for inclusion in the meta-analysis. For the purposes of this meta-analysis, we included studies with a minimum of 10 consecutive patients evaluating those with AIS with ≥70% stenosis or occlusion of the extracranial ICA and concomitant occlusion of the intracranial ICA and/or proximal MCA with at least 70% of the cases treated with second-generation MT devices (eg. Solitaire, Trevo, Revive, Preset, Penumbra). Case reports, review articles, studies with <10 patients, studies including patients with incomplete occlusion of the intracranial large vessel and/or <70% stenosis of the extracranial ICA in their definition of TO, and studies with ≥30% of cases using first-generation devices (ex: MERCI) or intra-arterial thrombolysis alone were excluded from this analysis. After selection of the articles, the data was extracted by one author.
Baseline data and outcome variables
We evaluated the following outcome measures: the overall outcomes of patients with tandem occlusions treated with second-generation mechanical thrombectomy devices; differences in outcomes of patients with extracranial treatment first compared with intracranial treatment first approaches; and differences in outcomes in patients treated with extracranial stenting at time of procedure compared with patients treated with angioplasty alone.
We collected the following demographic information from each study: number of patients, age, gender, presenting National Institute of Health Stroke Scale (NIHSS), percentage of patients treated with IV thrombolysis, comorbidities (smoking, dyslipidemia, hypertension, diabetes mellitus), onset to arrival, onset to puncture, location of intracranial occlusion, number of patients undergoing angioplasty alone, number of patients undergoing stenting alone, number of patients treated extracranially first, number of patients treated intracranially first, MT device(s), use of anticoagulation, and antiplatelet strategy. Available data including rates of modified Rankin Scale (mRS)≤0–2 at 90 days, mortality at 90 days, procedure-related complications, technical success rates of carotid revascularization, rates of thrombolysis in cerebral infarction (TICI) IIb/III and TICI III only, rates of any intracerebral hemorrhage (ICH) and symptomatic ICH, NIHSS at 90 days, and procedure times were separately extracted for all patients (overall outcomes), extracranial treatment first patients, intracranial treatment first patients, stented patients, and angioplasty-only patients.
Statistical analysis
From each study, we extracted a number of events at the end of follow-up and sample size. We used a random-effects model for combining cumulative incidence rates (ie: event rates) in order to account for heterogeneity between studies. The I2 index was used to express the proportion of inconsistency that is not attributable to chance. Analysis was conducted using Stata 14 software (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP).
Study quality and risk of bias assessment
As included studies were case series and uncontrolled, individual quality was evaluated using the National Institute of Health Quality Assessment Tool for before-after (pre-post) studies with no control group.6 This checklist evaluates uncontrolled studies for an overall quality rating, and has been used in a previous meta-analysis of MT efficacy and safety in TO patients.4
Results
Literature search
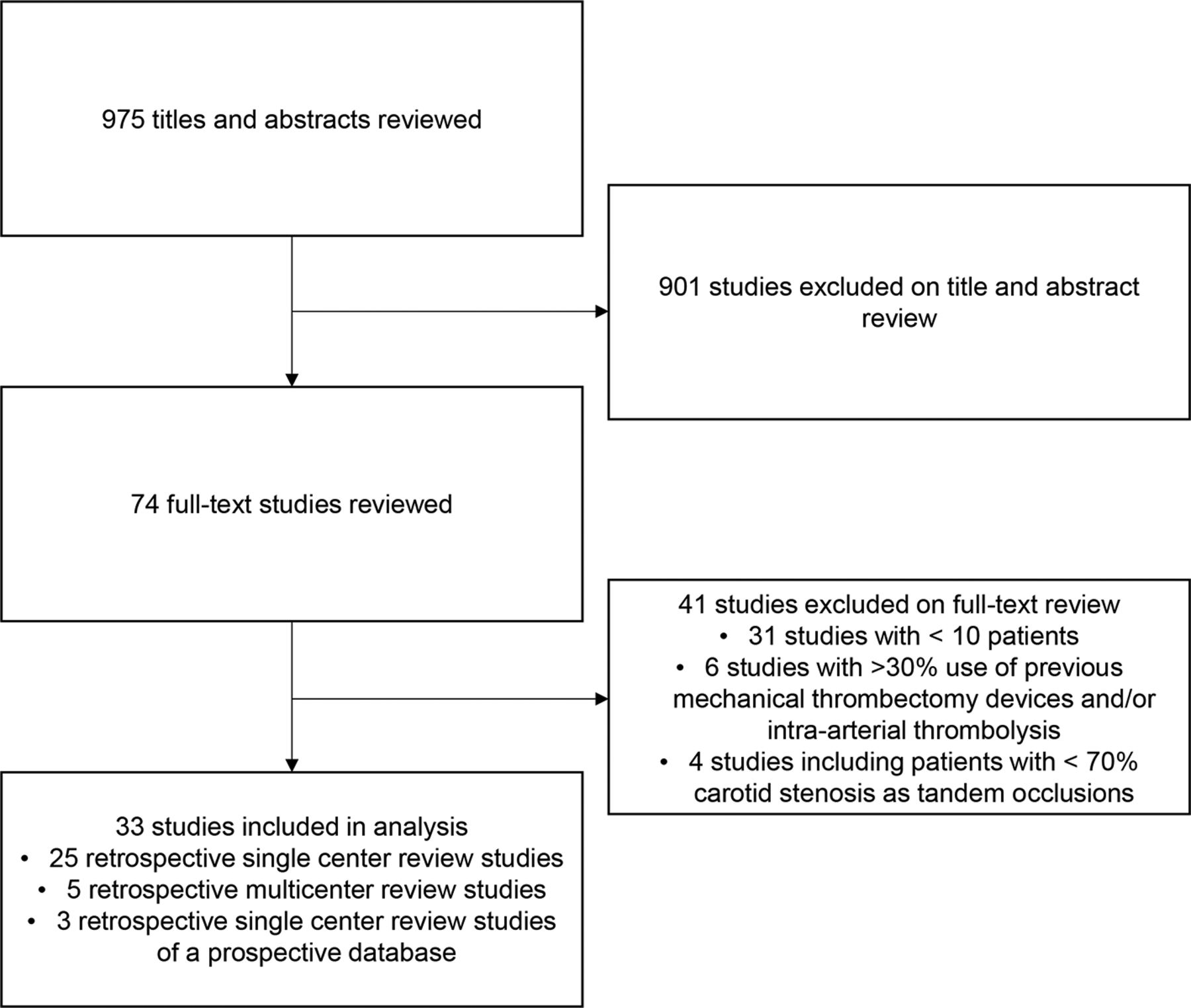
Initial literature search identified 975 unique articles or abstracts. On review of the abstracts and titles, 901 were excluded based on review of the title and abstract. Seventy-four articles were retrieved for full text evaluation, of which 33 met the inclusion criteria.5 7–38 Of the articles excluded from full text review, 31 articles included less than 10 patients, six articles utilized previous generation clot retrieval devices in more than 30% of cases, and four articles included patients with less than 70% stenosis of the extracranial ICA. Most included studies used a predominantly second-generation stent retriever technique (27/33), while the remainder used a combination of second-generation stent retrievers and/or an aspiration method as their predominant technique (6/33). Of the included 33 studies, 25 were retrospective single center reviews, five were retrospective multicenter reviews, and three were retrospective single center reviews of a prospective database. All studies included in the analysis had at least one or more outcome measure available for one or more of the patient groups analyzed. The literature search flow diagram is provided in figure 1.

PRISMA flow diagram showing screening and selection of studies for systematic review.
In total, 1102 treated patients with tandem occlusions were included in this assessment. Of these, outcome data was provided for 158 patients undergoing extracranial treatment first, and 158 patients undergoing intracranial treatment first. Outcome data was provided for 509 patients undergoing extracranial treatment with stent placement at the time of procedure, and 76 patients treated with angioplasty only. Patient characteristics of the included studies and baseline demographic data are provided in table 1.
Overall outcomes in tandem occlusions treated with MT
A total of 30 studies reported 90-day mRS in patients with tandem occlusions treated with MT for a total of 1070 patients, with a 47% (95% CI 42% to 51%) overall rate of mRS ≤0–2 at 90 days (figure 2). I2 value was 48%, indicating no substantial heterogeneity in reported outcomes. The 90-day mortality rate was 15% (CI 0.11 to 0.19), symptomatic ICH rate was 8% (95% CI 6% to 11%), TICI IIb/III rate was 78% (CI 73% to 82%), and TICI III rate was 36% (95% CI 26% to 48%). Mean procedure time was 79 min (95% CI 70 to 88 min). I2 value was 93% for procedure times, indicating substantial heterogeneity among procedure times. Insufficient data was available to compare NIHSS at 90 days. Meta-analysis outcome data is provided in table 2.
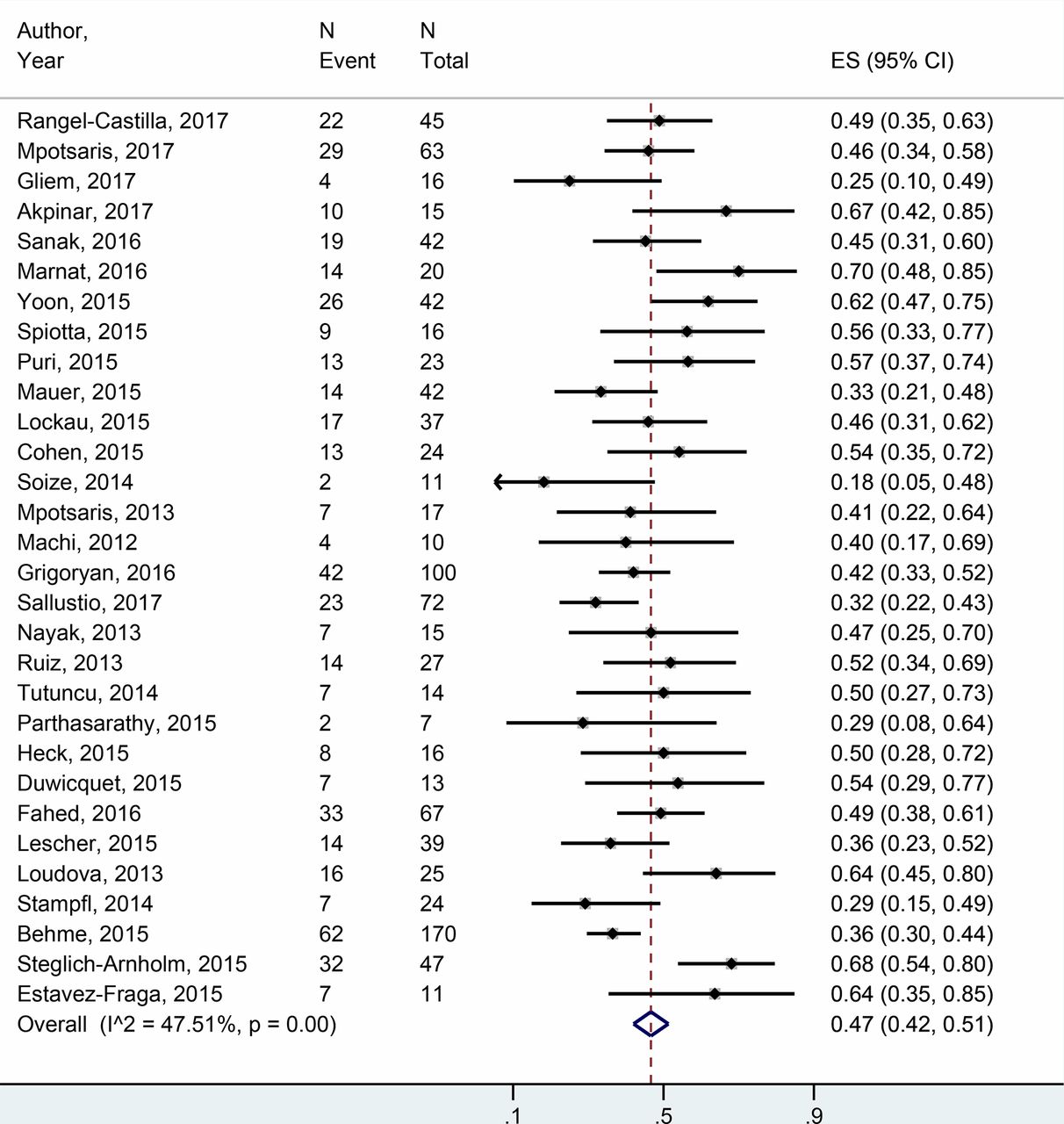
Forest plot for meta-analysis assessing rate of 90-day mRS≤0–2 in all tandem occlusion patients treated with mechanical thrombectomy.
Meta-analysis outcome data for overall tandem occlusions treated with mechanical thrombectomy, intracranial first versus extracranial first approaches, and stenting versus angioplasty-only approaches
Extracranial versus intracranial treatment first approaches
A total of eight studies provided data on 90-day mRS in extracranial first MT treatments of TO patients, with a rate of 53% (95% CI 44% to 61%), while seven studies provided data on 90-day mRS in intracranial first treatment with a rate of 49% (95% CI 39% to 50%) (P=0.58) (figure 3). I2 value was 18%, indicating no significant heterogeneity. The 90-day mortality was 8% in extracranial first and 15% in intracranial first patients, P=0.28. I2 value was 28%, indicating no significant heterogeneity. No differences were seen between groups for procedure-related complications, symptomatic ICH, TICI IIb/III, TICI III, technically successful carotid revascularization rates, or procedure times. The TICI IIb/III recanalization rate is presented in figure 4. Insufficient data was available to compare NIHSS at 90 days.
Meta-analysis outcome data for overall tandem occlusions treated with mechanical thrombectomy, intracranial first versus extracranial first approaches, and stenting versus angioplasty-only approaches

Forest plot for meta-analysis assessing rate of 90-day mRS≤0–2 in patients treated with extracranial first and intracranial first approaches for tandem occlusion patients treated with mechanical thrombectomy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for meta-analysis assessing rate of TICI IIb/III recanalization in patients treated with extracranial first and intracranial first approaches for tandem occlusion patients treated with mechanical thrombectomy.
Stenting versus angioplasty-only treatment of extracranial ICA occlusion
A total of 13 studies provided data on 90-day mRS in MT with extracranial stenting treatments of TO patients, with a rate of 49% (95% CI 42% to 56%), while three studies provided data on 90-day mRS in angioplasty-only extracranial treatment with a rate of 49% (95% CI 33% to 65%) (P=0.39). I2 value was 49%, indicating no substantial heterogeneity among studies. The 90-day mortality was 10% (95% CI 6% to 15%) in 14 extracranial stenting studies and 13% (95% CI 0% to 25%) in two studies providing data for angioplasty-only outcomes (P=0.38). I2 value was 34%, indicating no substantial heterogeneity. No differences in adjusted meta-analysis were seen between groups for procedure-related complications, symptomatic ICH, TICI IIb/III, or procedure times. Insufficient data was available to compare NIHSS at 90 days, TICI III rates, or the technical success rates of carotid revascularization.
Study quality and risk of bias assessment
All studies were retrospective reviews, three of which retrieved data from a prospective database. Studies demonstrated important heterogeneity in terms of inclusion criteria (eg. what types of endovascular therapies were included), supplemental management (eg. antiplatelet regime), outcome data, and data assessment. Almost all studies were non-comparative. Using the prespecified tool, studies were of variable rating quality, though predominantly rated fair or poor for potential risk of bias.
Discussion
Overall outcomes in tandem occlusions treated with MT
This systematic review and meta-analysis of >1000 patients treated with second-generation MT techniques has demonstrated that nearly half of all treated patients have good neurological outcomes (GNO) (mRS ≤0–2 at 90 days). This rate of GNO is comparable to findings of efficacy in a smaller review performed recently.4 Furthermore, the rate of GNO is similar to outcomes following MT in the entire population of patients treated with second-generation MT techniques, where a rate of 46% mRS ≤0–2 at 90 days was identified in the HERMES meta-analysis data,3 although this comparison is made with caution due to the predominantly retrospective nature of included studies in our analysis. While previously identified as an independent predictor of poor outcome in patients treated with thrombolysis alone,2 our findings suggest that TOs do better with MT showing a similar improvement as has been seen in MT for large-vessel occlusion alone. This superiority for MT in TO has also been identified in MR CLEAN, ESCAPE, and REVASCAT trials,39–41 though these studies were not included in our meta-analysis due to the unavailability of sufficient subgroup data.4
Improved outcome in TO patients is likely related to more complete recanalization, and reduced time to recanalization than was traditionally seen with thrombolysis only. This is evidenced by a TICI IIb/III rate of 78% (95% CI 73% to 82%) in our meta-analysis, compared with only a 9% recanalization rate in the thrombolysis era.1 While it is theorized that tandem occlusions increase the time to reperfusion, our meta-analysis also demonstrates a reasonable 79 min (95% CI 70 to 88 min) procedure time. There was significant heterogeneity among studies with respect to procedure time, though the perceived increase in overall time to revascularization in TOs is likely less than initially believed.
The safety profile in our meta-analysis also appears comparable to the general MT group seen in the HERMES data, with a similar mortality rate of 15%. Although limited by differences in included studies, our meta-analysis demonstrates only a slightly higher rate of symptomatic ICH at 8% (95% CI 6% to 11%), than is seen in the general MT group demonstrated by HERMES data (4.4%). A slightly higher rate of symptomatic ICH is likely accounted for by the need for a more aggressive antiplatelet regimen in stented patients, which was performed in the majority of patients in our meta-analysis. Early aspirin administration in acute stroke treated with thrombolysis has been shown to result in higher rates of symptomatic ICH in a large, multicenter, randomized controlled trial.42 Although specific antiplatelet regimens were highly variable and incompletely reported among studies included in our analysis, most studies demonstrated a regimen involving ASA and/or clopidogrel. For example, in the largest included study, Behme et al reviewed a total of 170 patients from four centers with a total of 15 patients (9%) with symptomatic ICH.27 In their study, all patients received extracranial stenting, with each center demonstrating a different antiplatelet regimen. Center A bridged with IV eptifibatide before loading with 300 mg clopidogrel and 500 mg ASA after stent placement followed by 8 weeks of dual antiplatelet therapy; Center B loaded patients with 500 mg ASA IV prior to stent placement followed by a 375 mg clopidogrel via NG tube loading dose and subsequently 4 months of oral antiplatelet therapy; Center C bridged patients with IV tirofiban prior to oral loading of 500 mg ASA and 300 mg clopidogrel and subsequently 4 months of oral antiplatelet therapy; and Center D treated patients with 500 mg IV ASA in conjunction with IV heparin or tirofiban bridging followed by possible 600 mg clopidogrel loading and subsequently 3 months of dual antiplatelet therapy. All patients in their study remained on lifelong monotherapy with ASA.
Extracranial versus intracranial treatment first approaches
Our meta-analysis demonstrates no statistical differences between revascularization rates, rates of GNO at 3 months, mortality rates at 3 months, nor rates of symptomatic ICH between patients treated with an extracranial first approach, and patients treated with an intracranial first approach. Further, no statistical differences are demonstrated for procedure-related complication rates, technical successful rates of carotid revascularization, nor procedure times between these groups.
To date, no consensus exists regarding an extracranial first versus intracranial first approach. Several authors have advocated for an extracranial first approach,5 18 19 21 24 25 32 35 while others favor an intracranial first approach.13 17 22 26 Some authors have reported an operator- and patient-dependent model.14 Despite the controversy, few studies have directly compared an extracranial first versus intracranial first approach. Lockau et al evaluated extracranial first versus intracranial first approaches in a small study of 25 patients, noting significantly shorter angiography time in intracranial first patients (43±31 min vs 111±43 min, P<0.001).22 They also noted a trend toward improved 90-day outcomes in the intracranial first group (13/25=52% vs 4/12=33%, P=0.319), though neither of the findings persist in larger pooled analysis. Our meta-analysis does demonstrate a slight trend toward an improved safety profile with an extracranial first approach including a 90-day mortality rate (8% [95% CI 3% to 15%] vs 15% [95% CI 3% to 32%]) and procedure-related complications (8% (1–20%)%] vs 20% (9–39%)%]), though these differences were not significant and did not translate into differences in 90-day GNO. A slight shift toward reduced procedure-related complications with an extracranial first approach may relate to improved collateralization and reduced trans-stenosis catheter manipulation during the intracranial thrombectomy. Rates of symptomatic ICH are similar between groups (8% [95% CI 3% to 15%] vs 7% [95% CI 2% to 15%]). At present, no single approach can be advocated for on a consistent basis.
Stenting versus angioplasty-only treatment of extracranial ICA occlusion
Our meta-analysis demonstrates no statistical differences between revascularization rates, rates of GNO at 3 months, mortality rates at 3 months, nor rates of symptomatic ICH between patients treated with extracranial stenting, and patients treated with angioplasty only. Further, no statistical differences are demonstrated for procedure-related complication rates, technical successful rates of carotid revascularization, nor procedure times between these groups.
Extracranial stenting versus angioplasty only at time of mechanical thrombectomy also represents a controversial issue. Akpinar et al postulate that delayed stenting may aid in preventing unnecessary stenting in patients with poor outcomes, in addition to preventing new or worsening intracranial hemorrhages due to early use of antiplatelet agents. In their study of 15 patients, they identified good outcomes in 67% (10/15), and a symptomatic ICH in only one patient when treating with angioplasty only during initial endovascular treatment.11 Lower rates of hemorrhages without stenting, however, were not corroborated by Lescher et al, where 13% (4/30) of patients without stenting developed symptomatic ICH, but no patients with stenting (0/9) developed symptomatic ICH.26 Most studies published to date evaluating MT in TO have entirely or partly treated extracranial occlusion with stenting during initial treatment. Few studies provide specific data on angioplasty only approaches. Further, differences between thrombolysis and antiplatelet managements between these groups is not well evaluated. In light of this, while no statistical differences are demonstrated between stenting and angioplasty-only groups in our meta-analysis, interpretation remains limited due to a small sample size in the angioplasty-only group.
Limitations and future direction
This systematic review and meta-analysis has a number of limitations due to the inclusion of predominantly uncontrolled studies. Most of the included studies were retrospective non-comparative series and are thus subject to some degree of selection bias in addition to demonstrating variability in available outcome data. Second, most studies included patients treated with more than one MT device and technique. Many studies also included some patients treated with first-generation MT devices and even some patients treated only with intracranial intra-arterial thrombolysis (IAT). Due to variability and lack of subgroup data analysis within studies, specific evaluation of second-generation MT devices could not be differentiated or compared with patients treated with first-generation MT or IAT alone. Third, as uncontrolled studies, inconsistent rates of reported outcome variables decreased the power of analysis in some categories. Variables which were insufficiently powered were not analyzed, and were identified in the results section. Fourth, due to their retrospective nature, several potentially important confounders such as antiplatelet regimen were variable and inconsistent. This subjects these series to the potential for both confounders and measurement bias. Finally, we did not differentiate patients with extracranial ICA occlusions from atherosclerosis or dissection etiologies, however, a recent study has shown that there are no differences in outcomes between these groups.43
Given the aforementioned limitations, this systematic review and meta-analysis highlights the need for more regimented studies specifically assessing outcomes in both extracranial versus intracranial first approaches with second-generation MT devices for tandem occlusions in AIS, and extracranial stenting vs angioplasty-only approaches. Ideally, both should be assessed with a prospective multicenter randomized controlled trial, though this approach may be difficult due to the time and cost required to acquire the number of patients for adequate effect size. Therefore, more retrospective and prospective series evaluating technical differences in approach will improve future pooled analysis. Specifically, more data on an angioplasty-only initial approach would be helpful, including comparing specific procedural-related complications to extracranial stenting and evaluating rates of re-occlusion in the angioplasty-only population. Future systematic reviews and meta-analysis could also evaluate other technical differences in approach for tandem occlusions which were not evaluated in our meta-analysis.
Conclusions
This is the largest known systematic review and meta-analysis to date evaluating tandem occlusions in acute ischemic stroke, and the first known to evaluate technical differences in approach. Nearly half of all patients with tandem occlusions treated with mechanical thrombectomy have good neurological outcomes. In addition to being efficacious, mechanical thrombectomy in tandem occlusions also demonstrates a good safety profile, and should be considered the standard of care in eligible patients. No statistical differences in outcomes are identified between extracranial first and intracranial first approaches. While no statistical differences are seen in extracranial stenting and angioplasty-only approaches, interpretation remains limited due to a small angioplasty-only sample size to date. More rigorous prospective studies are needed. At present, however, the approach to mechanical thrombectomy in tandem occlusions should be tailored on an individual operator- and patient-specific basis.
References
Footnotes
Contributors MPW and WB conceptualized and designed the project. MPW reviewed the articles and collected the data. MHM analyzed the data. All authors contributed to data interpretation, write-up, editing, and revisions of the final manuscript. All authors have contributed to production of the final version of this manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data from this project can be acquired by contacting the corresponding author at mitch.wilson@ualberta.ca