Article Text

Abstract
Introduction The effectiveness of a scoring system based on the circle of Willis for evaluations of collateral circulation was studied in patients with intracranial atherosclerotic stenosis.
Methods Eighty-three patients who underwent medical or endovascular treatment for symptomatic and severe intracranial atherosclerotic stenosis were enrolled in the study. Clinical profiles, status of the circle of Willis (poor and good integrity group), and clinical outcomes were analyzed. Primary endpoints were: (1) symptomatic ischemic or hemorrhagic stroke within 30 days; and (2) recurrent transient ischemic attack or ischemic stroke beyond 30 days.
Results The estimated rates of the primary endpoint at 1 and 2 years after treatment were 8.5% and 11.4% in the medical group and 7.0% and 9.7% in the endovascular group, respectively. A primary endpoint event after medical treatment was only identified in patients with poor integrity of the circle of Willis (p=0.059). In patients with poor integrity of the circle of Willis, previous antiplatelet medication before initial presentation (p=0.026) and hypertension (p=0.006) were more prevalent. During the follow-up period, complete arterial occlusion was identified in 9 patients. The circle of Willis score of the patients with complete arterial occlusion was 1.33±1.52 in the fatal stroke group (n=3) and 3.20±1.64 in the asymptomatic group (n=6, p=0.099).
Conclusions If patients have poor integrity of the circle of Willis, the risk of recurrent stroke may be increased. Such patients appear to be good candidates for endovascular treatment.
- Angioplasty
- Atherosclerosis
- Stroke
- Stenosis
Statistics from Altmetric.com
Introduction
Intracranial atherosclerotic stenosis is one of the most common causes of stoke.1 A recent randomized prospective study (Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis, SAMMPRIS) demonstrated the superiority of medical treatment over invasive endovascular treatment.2 ,3 Considering the high periprocedural risk of endovascular treatments and the unexpectedly good outcomes of medical treatments, appropriate patient selection is very important for the endovascular treatment of intracranial atherosclerotic stenosis. If we can find a patient with a high risk of stroke even after medical treatment, this patient can be a good candidate for endovascular treatment.
The investigators in the Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) study reported that collateral circulation could be a prognostic factor for intracranial atherosclerotic stenosis.4 ,5 However, the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) grading system, which is widely used, has many limitations regarding its use as a prognostic factor for intracranial atherosclerotic stenosis because it was fundamentally designed for an intra-arterial cerebral thrombolysis trial in relation to acute ischemic stroke.4–7 Most patients with intracranial atherosclerotic stenosis (not occlusion) tend to be classified as ‘none’ or poor collaterals (grade 0, 1 or 2) according to a report by Liebeskind et al.4 ,5 Furthermore, the ASITN/SIR grading system cannot predict the potential for the future development of collaterals, instead only reflecting the current collateral status.
We therefore designed a new scoring system called the ‘circle of Willis score’. To evaluate the clinical effectiveness of the new scoring system, we designed a retrospective study involving patients with intracranial atherosclerotic stenosis at our institution.
Methods
Patients with severe and symptomatic intracranial atherosclerotic stenosis (70–99%) were enrolled in this study. A detailed scheme of the study is shown in figure 1. Stenosis was measured by the WASID criteria.8 According to these criteria, 83 patients were finally enrolled in the study. Forty-two patients initially underwent medical treatment and 41 underwent endovascular treatment. For two patients in the medical group, the medical treatment failed and they later underwent endovascular treatment. Finally, 42 patients were included in the medical group and 43 patients were included in the endovascular group.

Detailed scheme of the study. BA, basilar artery; ICA, internal carotid artery; MCA, middle cerebral artery; PTA, percutaneous transluminal angioplasty; PTAS, percutaneous transluminal angioplasty with stenting; VA, vertebral artery; WASID, Warfarin-Aspirin Symptomatic Intracranial Disease.
At our institution, medical treatment is the first treatment option for intracranial atherosclerotic stenosis and it is performed by an independent neurologist or by a neurosurgeon according to current guidelines.9 An endovascular treatment is selectively recommended only when the patient has recurrent ischemic symptoms in spite of the medical treatment or when the patient was initially considered as having a high risk of recurrent stroke by the attending physician after considering the complete clinical situation.
Such a treatment strategy is reflected in the clinical profile (table 1), in which patients who were already prescribed antiplatelet medication before their initial presentation were more common in the endovascular group despite the marginal level of statistical significance (p=0.081). There were no statistically significant differences between the medical and endovascular groups apart from the duration of follow-up. The endovascular group had a smaller proportion of patients with middle cerebral artery lesions (16.3% vs 42.9%, p=0.061).
Clinical profiles of the enrolled patients
In the endovascular group, percutaneous transluminal angioplasty (PTA) was performed in 16 patients and percutaneous transluminal angioplasty with stenting (PTAS) was performed in 27 patients. Coronary balloons and stents were used in 38 patients, and the Gateway balloon/Wingspan stent system was used in four patients. In one patient an Enterprise stent was used after angioplasty with a Gateway balloon. Most endovascular procedures were performed under local anesthesia, meaning conscious sedation with intramuscular injection of 50 mg phenobarbital.
To evaluate the collateral circulation as a prognostic factor, we designed a new scoring system. Our scoring system, called the circle of Willis score, is based on the hypothesis that the integrity of the circle of Willis determines the potential for the future development of the collateral circulation caused by the progression of intracranial atherosclerotic stenosis. Details of the circle of Willis score are shown in table 2. It consists of scores for the anterior communicating artery (ACoA) and for the posterior communicating artery (PCoA). Each ACoA and PCoA score is evaluated by a certificated neurointerventionist based on complete four-vessel angiography. The ASITN/SIR grade is also evaluated for a comparison with the circle of Willis score. The maximum circle of Willis score is 6, indicating the existence of a large ACoA and PCoA—that is, complete integrity of the circle of Willis. The circle of Willis scores were dichotomized into poor (0–2) and good (3–6) integrity groups for statistical analysis.
Scoring system for the evaluation of the integrity of the circle of Willis
Primary endpoints were: (1) symptomatic ischemic or hemorrhagic stroke within 30 days after cerebral angiography (medical group) or endovascular treatment; and (2) recurrent transient ischemic attack (TIA) or ischemic stroke beyond 30 days. Secondary endpoints were any death and ischemic stroke in any non-qualifying artery territory. Because a minor stroke may remain undetected during the follow-up period due to the limitations of a retrospective study, recurrent TIA beyond 30 days was included as a primary endpoint.
After treatment the patients underwent clinical follow-up by independent attending physicians. Follow-up radiological images were reviewed by an independent neuroradiologist. Stenosis ≥50% and progression of stenosis ≥20% compared with the immediate post-procedural angiography was considered as re-stenosis. Statistical analyses were performed using independent t tests, the Fisher exact test, and a Kaplan–Meier analysis with a log rank test.
Results
Overall clinical outcomes are shown in table 3. There were no statistically significant differences between the two groups. The results of the Kaplan–Meier analysis are shown in figure 2. In the medical group the estimated rates of the primary endpoints were 8.5% (95% CI 2.8% to 24.1%) and 11.4% (95% CI 4.5% to 27.7%) 1 year and 2 years after enrollment, respectively and, in the endovascular group, the estimated rates of the primary endpoint were 7.0% (95% CI 2.3% to 20.1%) and 9.7% (95% CI 3.7% to 23.9%) 1 year and 2 years after treatment, respectively.
Clinical outcomes of the enrolled patients

Kaplan–Meier analysis of the primary endpoint in the medical and endovascular groups (log rank test, p=0.975). TIA, transient ischemic accident.
Most of the endovascular procedures (86%) were performed under local anesthesia. Only six procedures (14%) were performed under general anesthesia owing to poor patient cooperation (n=2) or combined coil embolization procedures for unruptured cerebral aneurysms (n=4). Five patients showed neurological symptoms during the procedure under local anesthesia, including transient lateral gaze limitation, severe headache, and brief seizures. Endovascular procedures were prematurely terminated in two of the five patients, and they later underwent successful endovascular treatment under general anesthesia.
Table 4 shows the results of a comparison between the circle of Willis scores and the ASITN/SIR grades. According to the ASITN/SIR grade, most patients were classified into the ‘none’ or ‘poor’ collateral group as reported by Liebeskind et al.5 However, patients were evenly distributed in the circle of Willis scoring system. In an analysis of the circle of Willis scores of all enrolled patients (n=82), apart from one patient with incomplete angiography data, 35 patients were included in the ‘good integrity’ group while 47 patients were in the ‘poor integrity’ group. There were no statistically significant differences between the good and poor integrity groups in terms of age (p=0.088), male-to-female ratio (p=0.812), initial presentation (p=1.000), initial degree of stenosis (p=0.853), follow-up duration (p=0.345), presence of diabetes mellitus (p=0.117), presence of dyslipidemia (p=1.000), or smoking (p=1.000). However, in the poor integrity group, previous antiplatelet medication before initial presentation (66.0% vs 40.0%, p=0.026) and hypertension (89.4% vs 62.9%, p=0.006) were more prevalent compared with the good integrity group. Internal carotid artery stenosis was more prevalent (48.9%) in the poor integrity group and M1 stenosis was more prevalent (48.6%) in the good integrity group (p=0.013). There were no statistically significant results in the analysis according to the ASITN/SIR grade.
Comparison of the circle of Willis score and ASITN/SIR grade
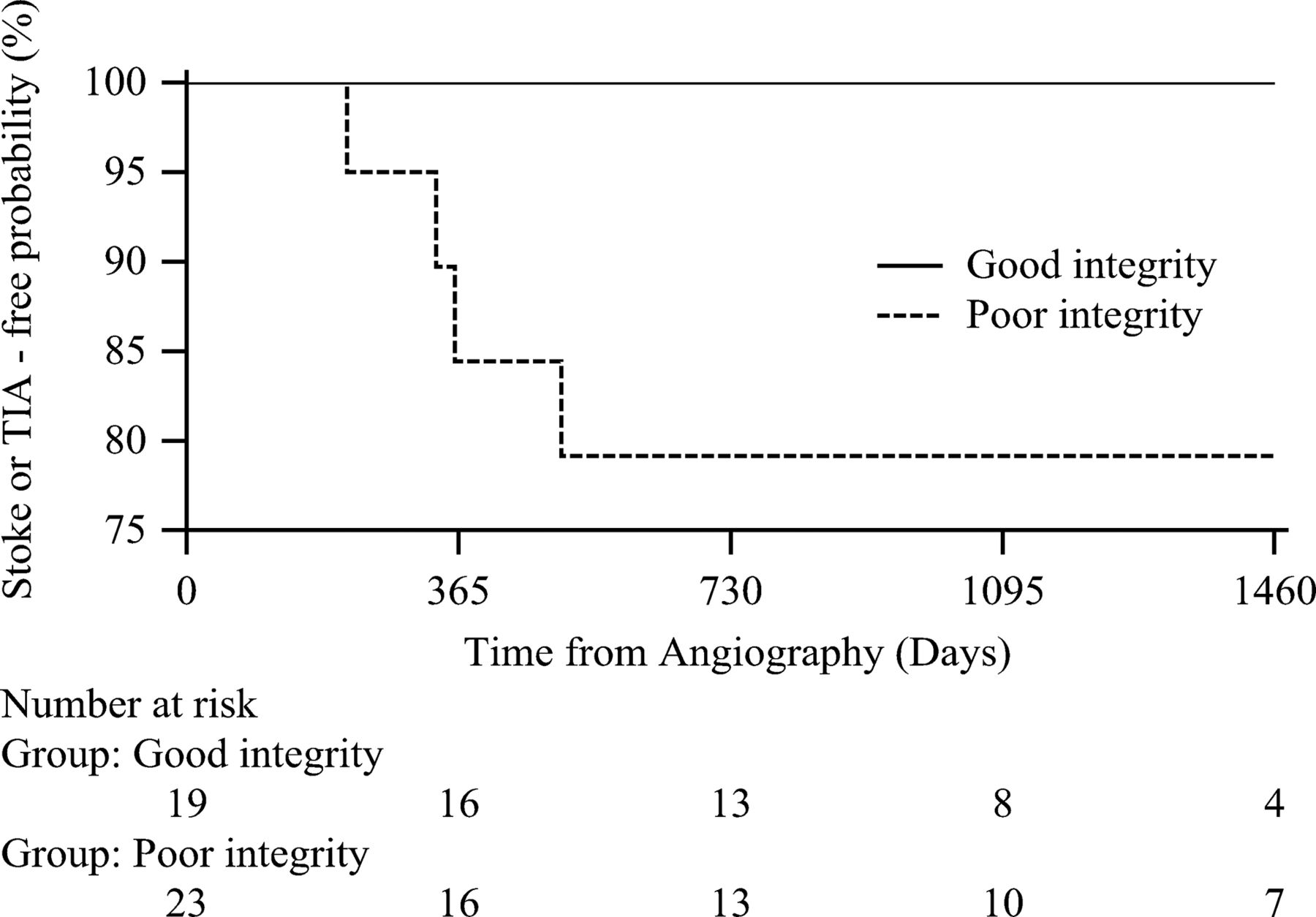
The results of a Kaplan–Meier analysis according to the circle of Willis score of the medical group are shown in figure 3. A primary endpoint event in the medical group was only identified in the poor integrity group (figure 3, p=0.059) and in patients with hypertension (p=0.184). No differences were found in the Kaplan–Meier analysis according to the circle of Willis score of the endovascular group (p=0.136).
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier analysis of the medical group according to the circle of Willis score (log rank test, p=0.059). TIA, transient ischemic accident.
Follow-up angiographic imaging (CT angiography, MR angiography or conventional cerebral angiography) was available for 21 patients (50.0%) at a mean interval of 22.5 months after medical treatment and in 31 patients (72.1%) at a mean interval of 25.5 months after endovascular treatment. Among these patients, progressive stenosis or re-stenosis was identified in two patients (9.5%) in the medical group and in four patients (12.9%) in the endovascular group (p=1.000). Additional PTA or PTAS were performed in three patients in the endovascular group to resolve re-stenosis. Complete arterial occlusions were identified in five patients (23.8%) in the medical group and in four patients (12.9%) in the endovascular group (p=0.457). These arterial changes were symptomatic in only three patients (2 fatal strokes in the medical group and 1 fatal stroke in the endovascular group) and the other patients had no neurological symptoms. The circle of Willis score of the patients with complete arterial occlusions which developed during the follow-up period was 1.33±1.52 in the fatal stroke group (n=3) and 3.20±1.64 in the asymptomatic group (n=6, p=0.099).
Discussion
This study showed outcomes for the medical group comparable to those of SAMMPRIS. Since 2000, a number of new medications have been developed and their effectiveness with regard to stroke prevention has been reported in randomized trials.10–12 The improvement in outcomes with medical treatment was also evidenced in the Carotid Occlusion Surgery Study (COSS), where the stroke rate 2 years after enrollment in the medical arm was lower than the initial expectation (22.7% vs 40%).13 In SAMMPRIS, a similar phenomenon was observed.2 ,3 For now, the current advancement in medical treatments for ischemic stroke appears to surpass those of endovascular or surgical treatments.
Despite the good outcomes in the medical group, there were still instances of medical treatment failures. A fatal stroke caused by the failure of medical treatment resulted from arterial occlusion via the progression of pre-existing stenosis. Such a patient can be a good candidate for endovascular treatment. If so, how can the risk of fatal stroke be evaluated? One remarkable finding of this study is that progressive occlusion or re-stenosis rates were considerable in both groups. A total of 16 patients in each group showed progression of stenosis or occlusion; however, most of them (75%) were asymptomatic on account of collateral flows from other intracranial arteries.
The future development of collateral circulation followed by the progression of intracranial atherosclerotic stenosis appears to play a critical role in determining patient outcomes. The current methods used to evaluate collateral circulation, such as the ASITN/SIR grade, reflect the tissue perfusion status at that time. These types of methods can be useful in cases of acute complete arterial occlusion; however, intracranial atherosclerotic stenosis is a different problem. The temporal features of the collaterals need to be evaluated. If intracranial atherosclerotic stenosis progresses continuously, there are two ways to compensate for the reduced blood flow. One involves direct collateral flows through the circle of Willis (antegrade collaterals) and the other involves leptomeningeal collaterals (retrograde collaterals). Leptomeningeal collaterals to offset the large arterial territory may require flow augmentation, which can be achieved by systemic hypertension or with additional flows through the circle of Willis from other arterial territories. In other words, the circle of Willis can be a route for antegrade collaterals and a route for blood flow augmentation as supplied by retrograde collaterals, which is why we designed the circle of Willis scoring system.
Interestingly, we found that the incidence of systemic hypertension was significantly higher (p=0.020) in the poor integrity group. This finding suggests that systemic hypertension is not only a risk factor for atherosclerosis but it can also be a physiologic response to decreased cerebral perfusion. Aggressive antihypertensive medication for such patients may therefore lead to hemodynamic instability and can result in poor clinical outcomes. However, in a post hoc analysis of the WASID trial, Turan et al14 reported that higher blood pressures are associated with an increased risk of ischemic stroke in patients with intracranial stenosis, which is completely contrary to the common clinical practice of maintaining high blood pressure in patients with intracranial stenosis. Turan et al14 suggested that higher blood pressure levels may be related to the progression of atherosclerosis.
According to the circle of Willis score, we can explain the conflicting result of the report by Turan et al as follows. Hypertension may have two roles in intracranial atherosclerotic stenosis: one is an atherosclerotic risk factor and the other is a physiologic response to maintain cerebral perfusion. If a patient has good circle of Willis integrity, hypertension may be an atherosclerotic risk factor rather than a physiologic response. In such a situation, hypertension needs to be controlled. However, if a patient has poor circle of Willis integrity, hypertension may be a physiologic response to augment blood flow through leptomeningeal collaterals, and maintaining a high blood pressure can be a reasonable treatment.
In this study, previous antiplatelet medication before initial presentation with ischemic symptoms was significantly prevalent in the poor integrity group (p=0.026). Thus, failures of antiplatelet medication were more prevalent in the poor integrity group. Furthermore, recurrent stroke in the medical group was only identified in patients with poor circle of Willis integrity. Amin-Hanjani et al15 reported that a low distal flow on quantitative MRI is related to a high risk of stroke in symptomatic vertebrobasilar disease. This finding suggests the importance of maintaining adequate cerebral perfusion, which can be achieved by the circle of Willis. The circle of Willis score appears to be a prognostic factor of the failure of medical treatment in these cases.
As a result of this study, we can predict that, if patients have a low circle of Willis score (0–2) and systemic hypertension, endovascular treatment can be a better option than medical treatment considering the risk of fatal stroke caused by arterial occlusion. However, even after endovascular treatment, the rate of re-stenosis or occlusion was not significantly decreased compared with the medical group (25.8% vs 33.3%). A high rate of re-stenosis after PTAS with the Wingspan stent had already been reported by other researchers.16 This may be a limitation of the current endovascular technique.
In this study, endovascular treatment resulted in clinical outcomes similar to those in the medical group. This is an impressive result considering that more serious (ie, medically intractable) patients were enrolled in the endovascular group. This outcome can be attributed to a low periprocedural stroke rate (7.0% in the current series vs 14.7% in SAMMPRIS). There are important differences in the procedural protocols of anesthesia. In our institution, local anesthesia (ie, conscious sedation) is a standard protocol with few exceptions. The effectiveness and safety of PTA or PTAS under local anesthesia have been reported, and the use of general anesthesia in SAMMPRIS has been criticized.17–19 Awake stenting enables an interventionist to detect neurological changes during the procedure. In this retrospective analysis, neurological deterioration could be detected during the procedure in five patients (13.5%), with transient symptoms in three and ischemic or hemorrhagic stroke in two. Severe vessel damage can be prevented by the early detection of neurological deterioration. Therefore, minimization of target vessel damage and maximization of the resolution of stenosis need to be balanced.
Although this study suggests that patients with poor integrity of the circle of Willis can be good candidates for endovascular treatment, it also has many limitations. The first is its retrospective nature. The second is that collaterals from the external carotid artery could not be evaluated in this study owing to the absence of external carotid artery angiography. The third is the small size of the population in only a single center. For that reason, we failed to show definite statistical significance and further statistical analysis is impossible.
In spite of these limitations, the circle of Willis score is a novel concept for the evaluation of collateral circulation. Additional well-designed studies are required to evaluate the clinical effectiveness of the circle of Willis score for intracranial atherosclerotic stenosis.
Conclusion
The circle of Willis is considered to play a critical role in preventing future stroke events in patients with intracranial atherosclerotic stenosis. If patients have a low circle of Willis score (0–2), endovascular treatment can be a good option compared with medical treatment considering the risk of fatal stroke caused by arterial occlusion.
References
Footnotes
Contributors KMK: Study design, data collection, statistical analysis and manuscript preparation as the first author. H-SK: Study design, result interpretation and manuscript preparation. WJL: Review of radiological images. YDC, JEK: Editing of the manuscript. MHH: Manuscript review and advice.
Competing interests None.
Ethics approval Ethics approval was obtained from the IRB of the corresponding author’s institution.
Provenance and peer review Not commissioned; externally peer reviewed.