Article Text

Abstract
Background Large vessel occlusive disease portends a poor prognosis unless recanalization is rapidly achieved. Endovascular treatment is typically performed via a transfemoral approach, but catheterization of the occluded vessel can be problematic in cases of extensive vessel tortuosity.
Methods A retrospective review of a prospectively maintained database identified 7 patients who underwent acute endovascular reperfusion therapy via transcervical approach.
Results We identified 7 patients. Admission NIHSS ranged from 8–27 and recanalization occurred between 7–49 min of carotid access. Prior to carotid access, 20–90 min were spent attempting target vessel catheterization via the transfemoral approach. All occlusions were in the left MCA. In 87.5% of patient, TICI2b/3 recanalization was achieved. Neck hematoma formation occurred in one case requiring elective intubation. At 2 months followup, all patients had survived with mRS 0–4 except for one patient who had a large infarct despite recanalization.
Conclusions Transcervical access for acute ischemic stroke leads to rapid and high quality recanalization. Future studies will focus on improved hemostasis and early identification of patients who would benefit the most from direct carotid access for acute stroke.
- Stroke
- Technique
- Thrombectomy
- Angiography
Statistics from Altmetric.com
Increasing lines of evidence have established a strong relationship between good functional outcomes after an ischemic stroke and fast reperfusion times. In a recent analysis of over 50 000 patients treated with IV thrombolysis, accelerating treatment by 15 min was associated with 18 more patients having improved ambulation at discharge, 13 more patients being discharged to a more independent environment and 4 fewer patients dying prior to discharge (per 1000 patients).1 A sub-study of the recently reported IMS-III study showed that every 30 min until reperfusion led to a 10% decrease in the probability of good outcome. While IV thrombolysis remains the first line therapy in acute ischemic stroke, not all patients are eligible for chemical thrombolysis and of those who are eligible, recanalization only occurs in 10–40% of cases.2
Mechanical thrombectomy is an important alternative strategy to restore flow, particularly in large vessel occlusive disease. The benefit of intra-arterial approaches, however, is negated by long delays in achieving reperfusion.2 ,3 Numerous barriers can lead to delayed revascularization including the logistics of patient transfer and the use of time-consuming advanced imaging. The standard endovascular approach to acute stroke intervention is the common femoral approach. The preference for this approach is related to the compressibility of the right common femoral artery, the potential for less dire consequences in case of femoral artery injury compared to carotid artery injury and to the fact that via this approach all brachiocephalic vessels can be catheterized and thus multiple potential sites of occlusion (eg anterior vs posterior circulation) can be accessed. Age and traditional cerebrovascular risk factors promote the elongation and tortuosity of the femoral, iliac, aortic, brachiocephalic and cervical arteries. Additional challenges in catheter navigation include thoracic aortic aneurysms and severe thoracic aortic atherosclerosis. Therefore once groin access is achieved, procedural times may be significantly prolonged in cases of difficult anatomy.4 In this study, we present 7 cases in which the target vessel could not be quickly catheterized via the transfemoral approach necessitating alternative access via a trans-cervical approach.
Methods
Patients were selected for endovascular therapy based on clinical syndrome (NIHSS>8) with suspected large vessel occlusion and radiographic evidence of well-preserved parenchyma (CT ASPECT score of 7 or greater and MRI ASPECTS of 6 or greater). All procedures were performed with minimal conscious sedation (utilizing dexmedetomidine, fentanyl and versed as needed) to permit serial neurological assessment. After transfemoral access was achieved, the target vessel could not be accessed with a base catheter. In one case, the transfemoral approach was not attempted as primary access modality due to the extreme vessel tortuosity observed on CTA.
In all cases, numerous wires could not be passaged distally in the common carotid to permit exchange of the diagnostic catheter for a shuttle sheath. After at least 20 min of procedural time, the transfemoral approach was abandoned and a transcervical approach was pursued.
In the supine position, the neck was extended. A rolled sheet was placed underneath the shoulders to help facilitate positioning. The neck was sterilized with a chlorohexidine sponge and then prepped and draped in normal sterile fashion. After subcutaneous administration of 1% lidocaine, the left common carotid artery was identified by palpation or visualized with ultrasonography (US) as necessary to achieve access using a micropuncture needle. The use of sonography was dependent on operator preference. If sonography was used, the most superficial aspect of the CCA proximal to the bifurcation was targeted. In the case of palpation, the most proximal aspect of the CCA distal to the clavicle was targeted. This was typically 2–3 finger breadths above the clavicle so as to allow the micropuncture needle to enter the skin at a 45° angle without being obstructed by the clavicle. Once brisk arterial blood was visualized in the micropuncture needle, a cope wire was advanced followed by a 4Fr introducer with the Seldinger technique. The microwire was replaced with an angled 0.038 glidewire (Terumo) to permit dilation with a 5Fr dilator followed by placement of a 5 or 6 Fr sheath. A skin incision was necessary to both facilitate catheter advancement and permit the redundant cervicle epidermis from being pulled into the arteriotomy. It should be noted that advancing the sheath through the cervical carotid is much more difficult than penetrating the femoral artery and often requires significant forward pressure. The Pinnacle sheath (Terumo) was subsequently connected to a pressurized heparinized saline infusion. The introducer sheath was advanced as distal as possible until it was either hubbed at the skin or tortuosity limited easy advancement over the wire. The use of sheath size was operator dependent. The 5F sheath was utilized to minimize the size of the arteriotomy but this limited the size of distal access catheter that could subsequently employed for manual aspiration. In cases where a 5F sheath was placed, the largest DAC that could be passed was a 044 DAC and manual aspiration could not be adequately performed. Thrombectomy was achieved with a Trevo device. The larger 6F sheath was utilized by some operators and this facilitated the entry of a larger 072 Navien catheter with successful manual aspiration thrombectomy. Manual aspiration was performed with a distal access catheter as previously described.5 Imaging of the head with MRI (1.5 T) or CT scan was then processed with automated software to calculate infarct volume size as previously described.6
Results
Patient features are summarized in table 1. In all cases, recanalization (TICI 2A-3) was achieved and in 87.5% patients recanalization TICI 2B-3 was achieved with procedural times ranging from 7–43 min.
Patient characteristics with procedural and clinical data
Case #1
An octogenerian presented with wake up symptoms of language difficulty and right sided weakness. Initial clinical examination fluctuated between an NIHSS of 3 to 5 with admission MRI head revealing no evidence of infarct. The patient was managed conservatively but subsequently developed worsening and persistent symptoms with an NIHSS of 10. MRA head revealed a left M1 occlusion and the patient was taken for angiography. Catheter based angiogram confirmed a left M1 occlusion. A 5Fr Simmons catheter was used to access the proximal left common carotid but could not be tracked further distal. Multiple catheters and wires were unsuccessful in achieving distal access. After 30 min of attempted catheterization, direct carotid access was attempted and successfully achieved. Successful recanalization with MAT (058 Navien catheter) was achieved 19 min after carotid access.
Access site closure was attempted with deployment of a Mynx closure device. This was unsuccessful and resulted in a neck hematoma. An angiogram revealed contrast extravasation at the cervical puncture site. At this point, manual pressure was applied for a total of 30 min and the patient was electively intubated for airway protection. A follow up CTA of the neck revealed no pseudoaneurysm and the hematoma was managed conservatively. The patient was successfully extubated and discharged to a rehabilitation facility. A post procedural MRI head revealed an infarct volume of 24 cc (figure 1C). At 3 months, the patient was ambulating independently with improved language.
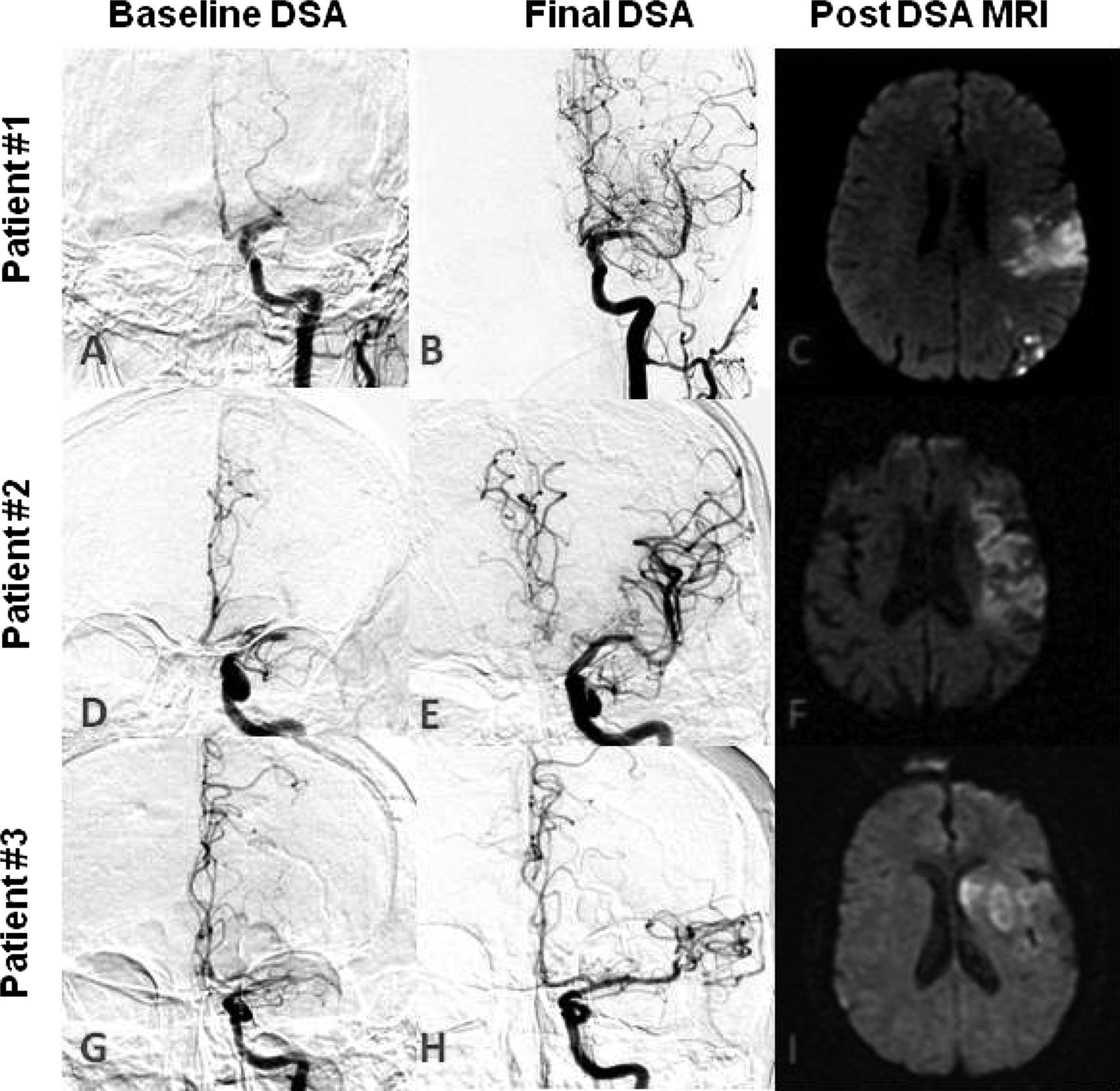
AP projection of the intracranial vasculature on digital subtraction angiography at baseline (Case #1, panel A; Case #2, panel D; Case #3, panel G) and after thrombectomy (Case #1, panel B; Case #2, panel E; Case #3, panel H). Diffuse restricted weighted imaging MRI reveals the final infarct distribution and volume (Case #1, panel C; Case #2, panel F; Case #3, panel I).
Case #2
An octogenerian presented with sudden onset of right sided weakness and language difficulty. Examination revealed an NIHSS of 27. CTA of the head revealed a left M1 occlusion with pre-procedural MRI head revealing a small left frontal infarct. The patient presented outside the IV tPA window and endovascular therapy was pursued. A diagnostic angiogram was performed with a 5 Fr Simmons catheter but the target vessel could not be catheterized after 20 min of procedural time. Carotid puncture was achieved after 13 min of attempting cervical access and recanalization with MAT (072 Navien catheter) was achieved 7 min after carotid access.
Access site closure was again attempted with deployment of a Mynx closure device followed by manual compression. The patient was quite agitated and did not tolerate manual compression. We maintained a 5 Fr catheter in the left common carotid to perform serial angiographic runs to confirm resolution of contrast extravasation. After 30 min of manual compression, contrast extravasation had subsided. A follow up carotid ultrasound the following day revealed no carotid pseudoaneurysm. A post procedural MRI head revealed an infarct volume of 24 cc (figure 1F). At 3 months, the patient was ambulating with assistance and had improved language function.
Case #3
An elderly patient with a history of hypertension and diabetes presented with wake up symptoms of language difficulties and right sided weakness (NIHSS 9). CT head revealed good preservation of the parenchyma (ASPECT score of 9) and CTA head revealed a left M1 occlusion. Extensive attempts to catheterize the left common carotid were unsuccessful with multiple catheters via the transfemoral approach. After 70 min of procedural time, the decision was made to pursue supra-aortic access. TICI 2b recanalization was achieved with two passes of manual aspiration (058 Navien catheter) 45 min after carotid access was established. Successful hemostasis was achieved with manual compression of the carotid access site for 30 min. A post procedural MRI head revealed a 21 cc infarct (figure 1I). At 3 months, the patient was non-ambulatory but had improved language function.
Case #4
An elderly patient presented with an NIHSS of 22. CTA of the head and neck revealed a left terminal internal carotid artery occlusion. Patient was not eligible for intravenous thrombolysis. After 90 min of attempted transfemoral carotid access through a bovine type III aortic arch (see figure 2A), direct carotid access was pursued. A 5F sheath was placed, through which a 4.3 DAC was advanced for attempted manual aspiration. The clot burden was however too large and could not be aspirated. After 3 passes with the Trevo device, recanalization was achieved (TICI 2a). No local complications was observed at the puncture site, however the patient finally developed a large infarct and died during the hospital stay.
{kind=link}
{kind=link}
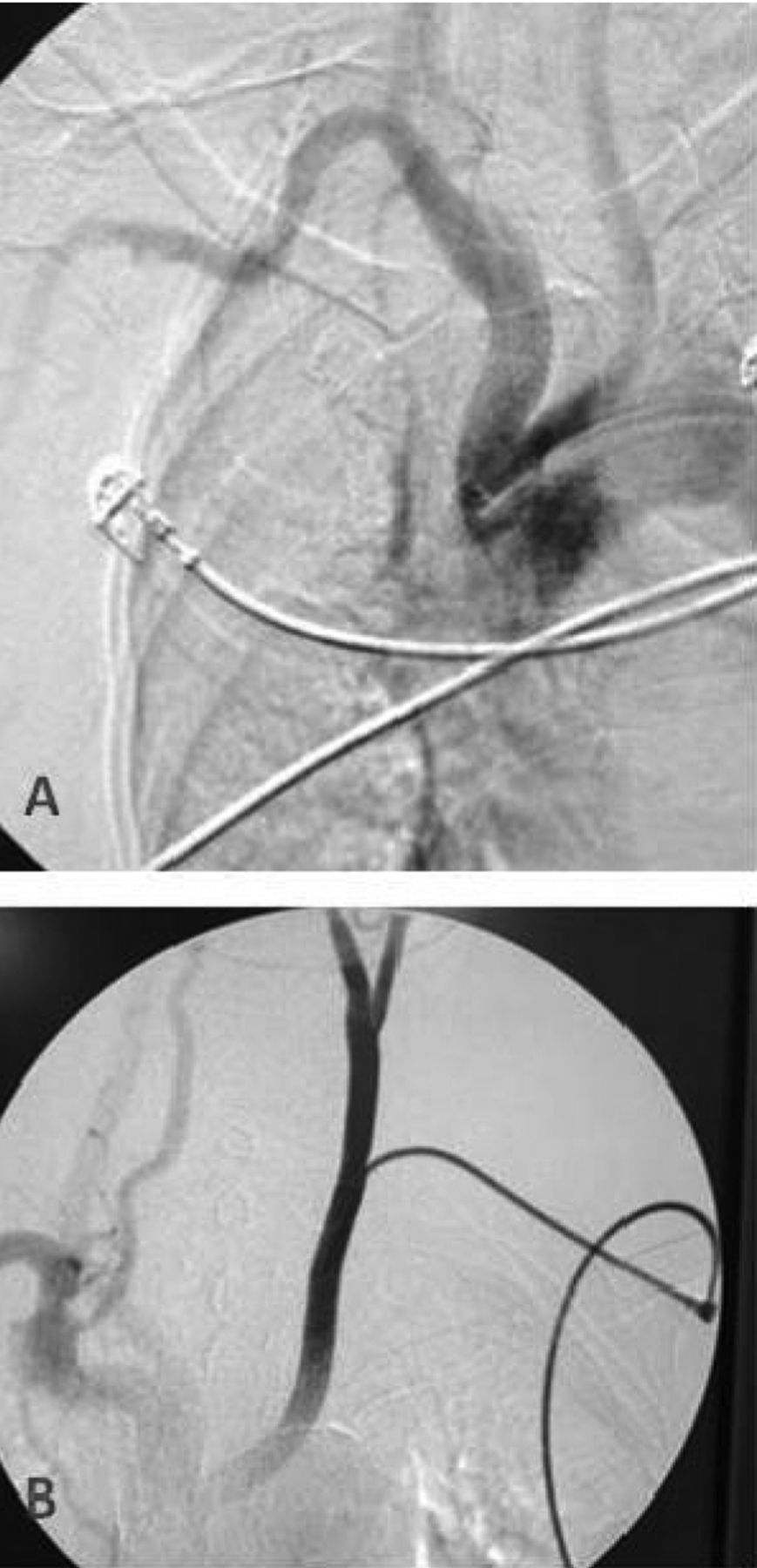
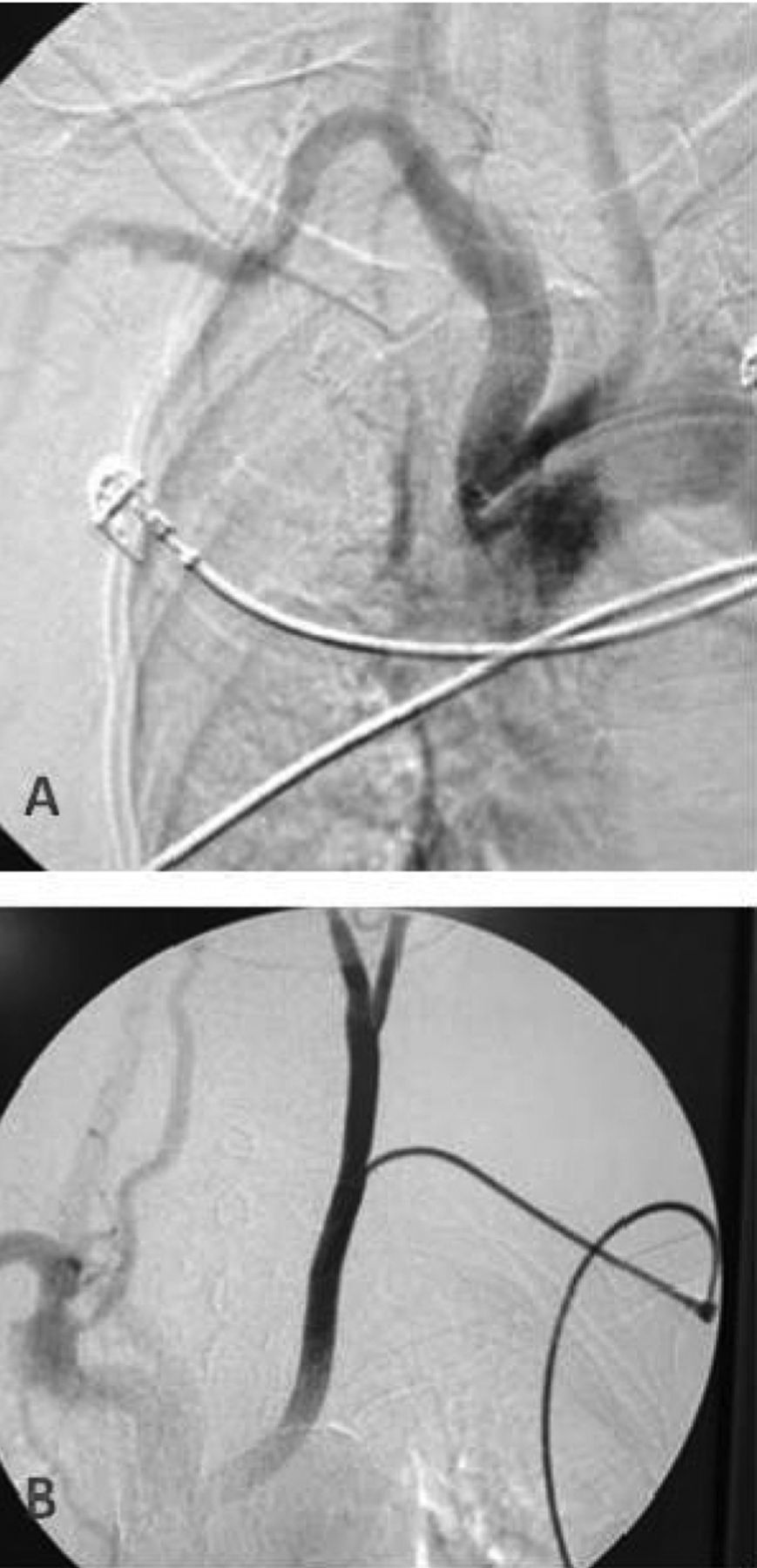
AP projection of the aortic arch on digital subtraction angiography. A: A bovine type 3 aortic arch limited target vessel catheterization in Case #4. B: Insufficient angulation lead to inadvertent placement of the sheath in the caudal direction in Case #5.
Case #5
An elderly patient received intravenous thrombolysis at an outside facility for a left hemispheric syndrome. On arrival to our center, the patient had a persistent clinical syndrome (NIHSS 17) and a CTA head and neck confirmed a proximal left M1 occlusion. After 60 min of attempted carotid catheterization via trans-femoral access, carotid access was pursued. Due to insufficient angulation during puncture, the 5F sheath was inadvertently placed in the caudal direction (see figure 2B). The initial cerebral angiogram showed almost complete recanalization (TICI 2B) and no further treatment was felt to be necessary. The sheath was immediately pulled out and manual compression was applied for 10 min. No local complications were observed and patient had complete clinical recovery (mRS 3 months: 0)
Case #6
An octogenerian with a history of hypertension and coronary artery disease presented with wake-up symptoms of right sided weakness and language difficulty at an outside facility and transferred for further evaluation. On arrival, the patient had an NIHSS of 20 with a CTA head and neck revealing a left M1 occlusion. Because of an extremely tortuous aortic arch observed on the initial CTA, a transcervical approach was directly undertaken. The target occlusion was accessed 10 min after puncture and recanalization (TICI 2b) was achieved after 3 passes of the Trevo device. Total procedure time was 40 min. The 5F sheath was removed and manual compression applied for 20 min. Carotid ultrasound confirmed absence of hematoma or common carotid damage at puncture site. No other complications were observed. At 3 months the patients had a mRS of 2.
Case #7
An octogenerian with a history of atrial fibrillation presented with sudden onset of right sided weakness and language difficulty (NIHSS 21). IV thrombolysis could not be administered due to dabigatran usage. A CT head revealed a hyperdense left MCA with minimal ischemic changes (ASPECT 8). Despite 90 min of attempted catheterization, the target lesion could not be accessed leading to a transcervical approach. After 8 min of carotid access, the left MCA artery was recanalized with a single pass with manual aspiration thrombectomy resulting in TICI2b flow. Carotid access hemostasis was achieved with manual compression for 20 min without neck hematoma formation. At 3 months, the patient had improved language but did require assistance for grooming and ambulation.
Discussion
Persistent large vessel occlusive disease is associated with high rates of mortality and morbidity. Difficult catheter access can lead to lower rates of recanalization and ultimately poor clinical outcomes. Transcervical access has been a successful alternate strategy for carotid stenting7 and aneurysm coiling.8 In this study, direct percutaneous puncture and catheterization of the common carotid artery was instrumental in achieving rapid and successful revascularization in the case of acute stroke intervention.
In a recent analysis of 130 patients undergoing endovascular procedures for acute stroke, 5.1% of the patients could not be successfully catheterized via transfemoral access.4 These patients had low rates of recanalization (14.3% vs 80.5%) and less good outcomes (0% and 36%). Recanalization in patients with good catheter access occurred with a median time of 20 min from groin puncture, whereas patients with high vessel tortuosity had greater than 30 min delay in catheter delivery to the target vessel.
While the transfemoral access remains the preferred approach in most cases, understanding the predictors of difficult access is critical in triaging the patients who may benefit the most from an alternative approach. In our series, an additional 20–90 min of procedural time was spent attempting to achieve catheterization via the transfemoral approach. Identifying these patients as poor candidates for the transfemoral approach at an earlier timepoint may have prompted a transcervical approach as the initial strategy and faster onset to treatment time. Predictors of difficult catheter during acute stroke include hypertension, hyperlipidemia, advanced age (>75 years of age) and left anterior circulation stroke.4 The seven patients in our study all had left MCA occlusions and most patients were older than 75. In a recent review of 1067 consecutive carotid stenting procedures, 90% were achieved via a femoral approach. An additional 9% were treated with a transbrachial approach. The remaining 10 cases (0.9%) could not be catheterized with either approach but were successful with a transcervical approach.7 The lesion was in the left carotid in 70% of the cases, again highlighting the challenge of catheterizing the left side.
The transfemoral approach has been associated with increasingly fast rates of groin access to recanalization, particularly with the advent of stentrievers. A recent comparison of various endovascular modalities revealed groin to recanalization time of 36±18 min for stentrievers compared to 92±67 min for intra-arterial thrombolysis and 114±57 min for the Merci device.9 In our cases series, once transcervical access was achieved, recanalization was similarly observed at ultrafast rates (25±14 min). In the case of patients 2 and 7, it took only 7–8 min to achieve recanalization. The proximal access saved time by not only bypassing the tortuous arch but also establishing better support and ease of access to the lesion. For the cases of manual aspiration, we suspect the proximal support also aided in a stronger aspiration effect.
While transcervical access may facilitate faster and higher rates of recanalization in a subset of patients, many challenges remain. We had difficulty achieving hemostasis in one patient with resultant neck hematoma. This led to elective intubation for airway protection although surgical hematoma evacuation was not necessary. Previous series have reported a 4–7% rate of neck hematoma after sheath removal.10 Several factors likely influenced the formation of a neck hematoma in our series. First, we commenced all our interventions with minimal conscious sedation to permit continuous clinical assessment during the procedure. However, manual compression was not well tolerated in two of the wake patients and this lead to difficulty in achieving continuous compression. In subsequent cases, additional sedation was administered during closure to minimize patient movement. Secondly, access was achieved with a percutaneous approach. An open surgical exposure, however, may be superior in achieving hemostasis as it mitigates the need for manual compression or a closure device.11 Open surgical exposure, however, may not be readily feasible in the acute stroke setting. Finally, we utilized the Mynx closure device without good success for carotid artery closure.
At present, the use of closure devices for this technique is limited. To our knowledge, there is no device approved for cervical carotid closure. Soon to be published data regarding the use of Starclose for percutaneous transcervical carotid stenting has been successfully utilized in over 100 cases without major complications or significant neck hematomas (Jacques Moret, personal correspondence). The ideal closure device would be exclusively extravascular and avoid the need for leaving behind an intravascular foreign body with subsequent risk of distal embolization. The use of alternative transfemoral closure devices such as Angioseal (St. Jude's Medical, Inc.)12 and Starclose (Abbott) may lead to superior results. The use of Perclose (Abbott) or Exoseal (Cordis) for this purpose has not been described. Manual compression alone has also been used with good success, even in cases of patients on dual antiplatelet therapy.13
In general, it would be reasonable to expect that anticoagulation use may lead to high risk of hematoma formation but in 2 cases, the concomitant use of intravenous thrombolysis (case #5) or oral anticoagulants (ie, dabigatran) (case #7) did not result in neck hematoma formation while achieving hemostasis with 10–20 min of manual compression. The use of intra-arterial thrombolysis also appears to be safe with adequate hemostasis during closure.
Despite the associated complications, we observed good quality of recanalization with low final infarct volumes and high rates of survival that exceed those expected for this age group. One can speculate that a primary access approach in these patients without the significant delay posed by the transfemoral approach attempts may have led to even better outcomes.
Conclusion
Successful endovascular therapy for acute stroke relies on a systems approach to reducing times at each step.14 Difficult catheter access of the target vessel can limit successful and timely recanalization in a subset of patients. In this preliminary series, the transcervical approach proved to be a feasible and efficacious strategy to achieve fast recanalization once the carotid artery was accessed. Future studies will focus on early triage of patients most likely to require alternative access to further limit procedural times as well as improving methods of achieving hemostasis.
References
Footnotes
-
Contributors Author contributions to the study and manuscript preparation include the following: Conception and design: all authors. Acquisition of data: all authors. Analysis and interpretation of data: all authors. Drafting the article: all authors. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: all authors. Administrative/technical/material support: all authors. Study supervision: all authors.
-
Competing interests TJ has received consulting and speaker fees from Co-Axia, ev3, Concentric Medical, and Micrus.
-
Ethics approval University of Pittsburgh, IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.