Article Text

Abstract
Background/objective Transarterial infusion of Onyx is now widely used in the treatment of arteriovenous malformations (AVMs) and dural arteriovenous fistulas (DAVFs). Transvenous Onyx embolization is rarely performed, and usually in cases of carotid cavernous fistulas. We describe a novel technique of transvenous Onyx embolization in the treatment of three high risk DAVFs and one vein of Galen (VOG) AVM.
Methods Cases were evaluated with specific attention to technical caveats, clinical indications, and complications. Patients were treated during 2011–2012 by two operators (FCA and CGM). Standard transfemoral venous approaches were employed in order to obtain access into the draining venous system in all cases.
Results Four female patients, aged 5 months to 68 years, were treated. Two patients, one presenting with headache and the other with a bruit, demonstrated high risk DAVFs involving the transverse–sigmoid sinuses. One patient, who was asymptomatic, manifested a high risk ethmoidal DAVF that was discovered incidentally during treatment of a basilar aneurysm. The final patient presented with symptoms of a pineal region mass and was found to have a VOG AVM. In all cases, a microcatheter was navigated through the draining venous pouch and into the ostium of an arterial feeder. A single Onyx infusion from this position filled multiple arterial feeders and resulted in cures in the first three patients and a significant reduction in AVM nidus in the fourth patient. No complications occurred.
Conclusions Transvenous Onyx infusion into a single arterial feeder can produce retrograde embolization of numerous other arterial feeders supplying high risk DAVFs and complex cerebral AVMs. This technique appears to be safe and potentially curative in select cases.
- Liquid Embolic Material
- Navigation
- Technique
- Vein
Statistics from Altmetric.com
Introduction
Transarterial and transvenous techniques have been employed for many years in the treatment of dural arteriovenous fistulas (DAVFs).1 ,2 Onyx is now routinely used for transarterial embolization of cerebral arteriovenous malformations (AVMs) and DAVFs.3 ,4 This liquid embolic agent has unique properties that enhance distal propagation into multiple feeding arteries. Often, a significant portion of the AVM or DAVF can be occluded through a single arterial injection. Rarely, Onyx has been injected transvenously for the treatment of AVMs and other complex fistulas. In a report of five cases, Kessler et al5 described their technique of transvenous Onyx embolization of AVMs. As in our report, they navigated a microcatheter through the draining vein as close as possible to the ostium of a feeding artery.5 Other authors have described the cavernous sinus infusion of Onyx for the treatment of indirect carotid cavernous fistula.6–8 These cases differ from ours, however, in that they involved occlusion of the venous drainage system, specifically the cavernous sinus. In this report, we describe our technique of transvenous to arterial Onyx infusion for the treatment of high risk DAVFs and a vein of Galen (VOG) AVM.
Methods
Patients
Transvenous to arterial infusion was performed in four patients. Each case was assessed for technical caveats, clinical indications for treatment, and complications. Embolization was performed by two operators (FCA and CGM), and angiographic follow-up was obtained in all patients.
Embolization techniques
Patient Nos 1 and 2
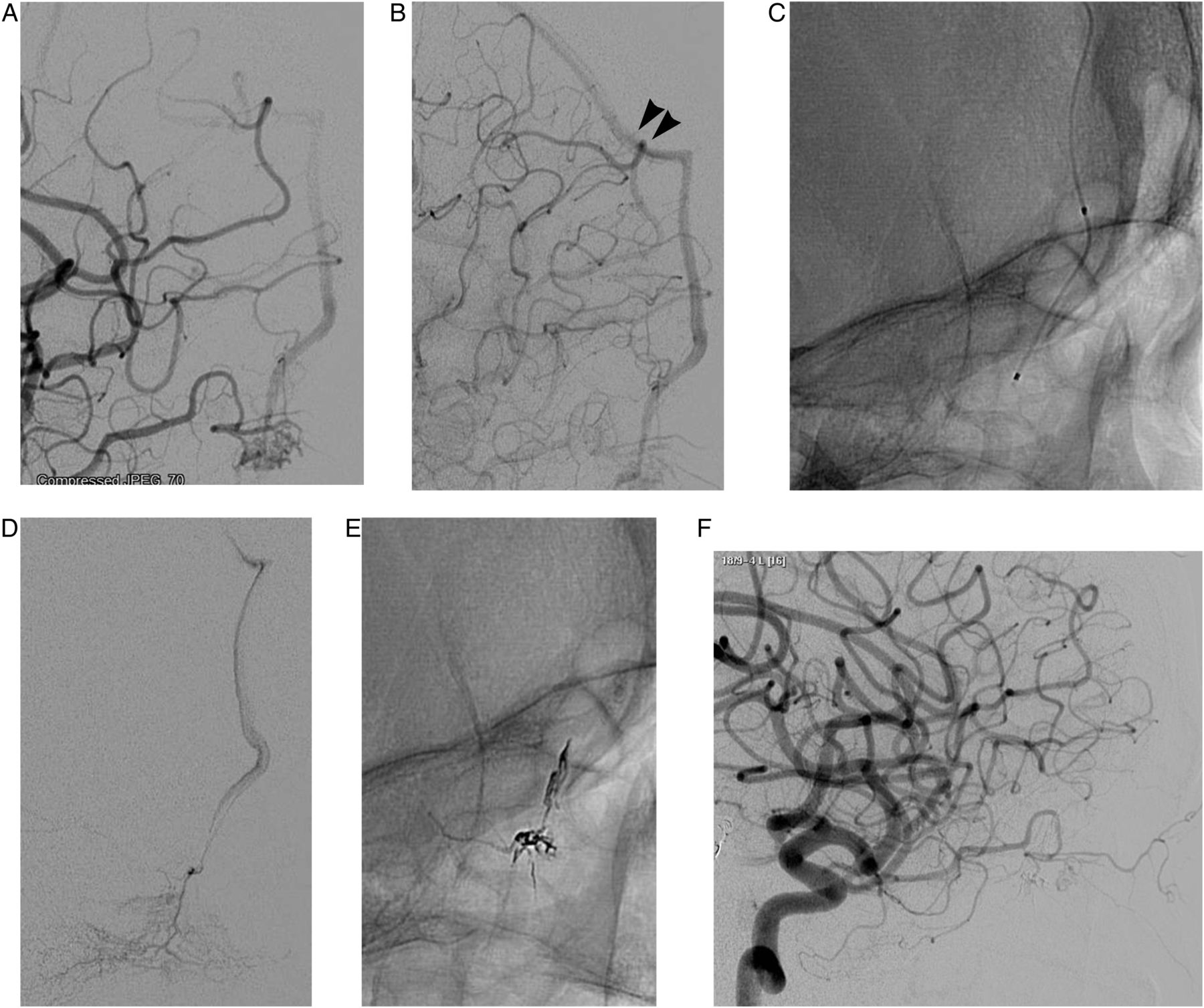
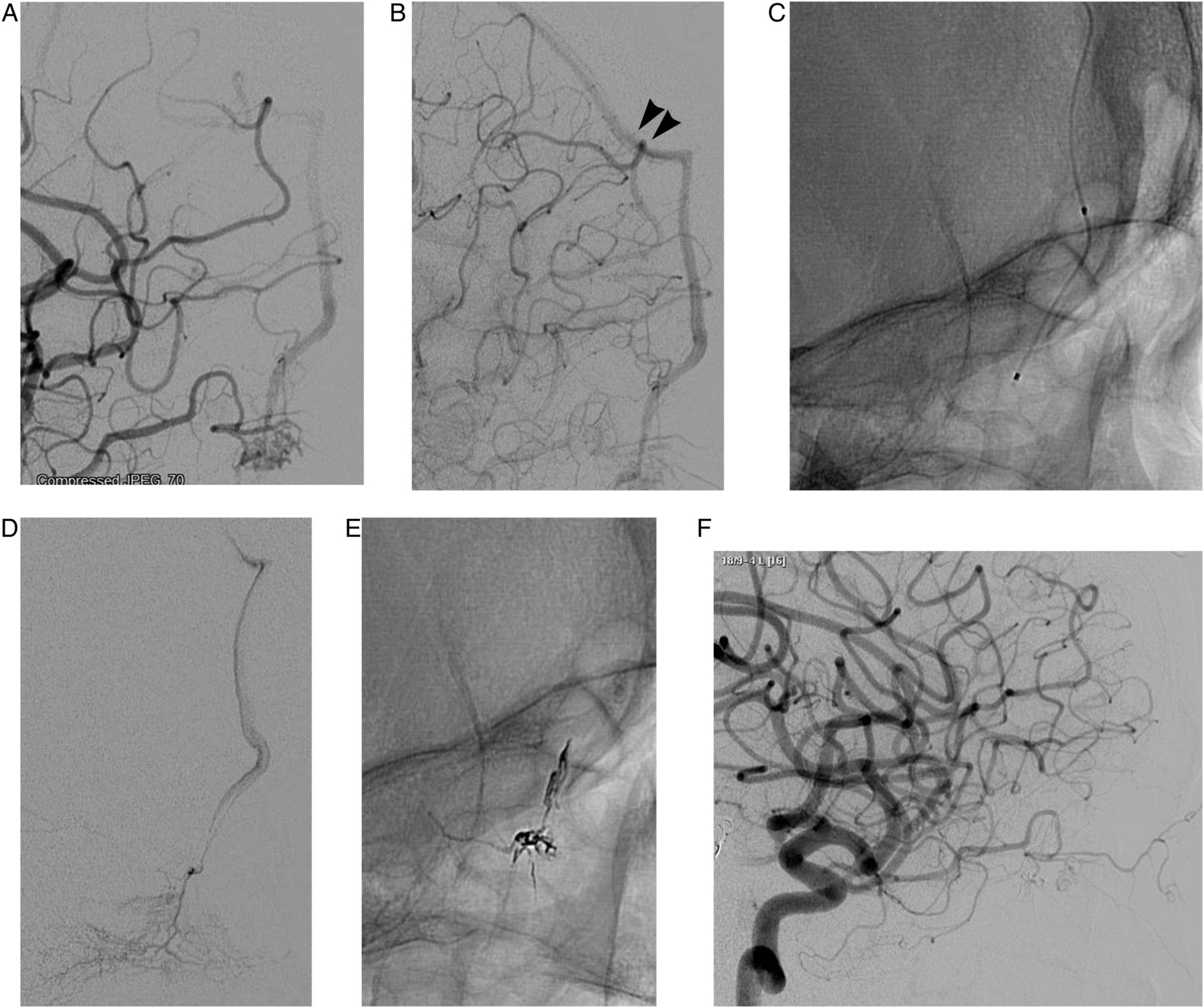
Standard transfemoral arterial and venous access was obtained in both patients with transverse–sigmoid fistulas. Superselective microcatheter angiography in both cases demonstrated a draining venous pouch parallel to the sigmoid sinus (figure 1A). Initially, transarterial Onyx 18 embolization was performed in both patients but quickly aborted due to excessive reflux and minimal penetration of the venous drainage system. A microcatheter was then navigated transvenously through the pouch and into the ostium of an arterial feeder (figure 1B). From this position, Onyx 18 was infused. Surprisingly, Onyx was noted to penetrate into multiple arterial feeders before refluxing into the venous pouch (figure 1C). In one case the entire pouch was casted and in the other, only a small amount of Onyx refluxed into the venous system. Control angiography immediately after transvenous to arterial treatment demonstrated a cure in both patients. Follow-up angiography at 9 months (patient No 1, figure 1D) and 6 months (patient No 2) confirmed a persistent cure.

(A) Patient No 1. Left common carotid artery (CCA) angiography demonstrates a left transverse–sigmoid high risk dural arteriovenous fistula (DAVF). The fistula first drains into a pouch (arrows) that runs parallel to the sigmoid sinus. (B) After navigating a microcatheter (arrow) into the distal aspect of the pouch, venography demonstrates not only the pouch but reflux into a collateral network of arterial feeders. (C) After embolization from a single arterial ostium, a native fluoroscopic image demonstrates extensive Onyx casting of multiple arterial branches. (D) Nine months later, left CCA angiography confirms cure of the DAVF. Used with permission from Barrow Neurological Institute.
Patient No 3
In the patient with an ethmoidal DAVF, transjugular venous access was obtained. This was done for two reasons. First, a standard microcatheter was not long enough to extend from a transfemoral guide catheter to the lesion, which was located on the floor of the frontal fossa and required navigation through the entire length of the sagittal sinus. Second, we were prepared to leave the catheter in place in the event that it became difficult to withdraw rather than risking avulsion of the cortical vein and intracranial hemorrhage. If this had occurred, we could have then cut the catheter as it emerged from the neck and tucked it under the skin. Conversely, leaving a retained venous catheter in the groin would have subjected the patient to thromboembolic complications as well as cardiac arrhythmias, given the catheter's course through the right atrium. Regardless, the microcatheter was easily withdrawn after embolization.
Transfemoral arterial access was obtained in this patient in order to perform control, right internal carotid artery angiography (figure 2A, B). After transjugular access was obtained, a 070 Neuron (Penumbra, Inc, Alameda, California, USA) catheter was navigated over a glidewire into the right transverse sinus. A microcatheter was then directed from the sagittal sinus into the draining frontal cortical vein (figure 2C). This allowed catheterization of the ostium of a feeding branch of the ethmoidal artery (figure 2D). Transvenous to arterial Onyx 18 infusion occluded several of the small feeding arteries and partially filled the distal aspect of the draining frontal vein (figure 2E). This treatment was immediately curative. Follow-up angiography at 6 months confirmed this cure (figure 2F).
(A) Patient No 3. Early phase left internal carotid artery (ICA) angiography demonstrates a high risk ethmoidal dural arteriovenous fistula fed from branches of the ophthalmic artery and draining into a frontal cortical vein. (B) Late phase left ICA angiography confirms that the frontal draining veins empty into the superior sagittal sinus (arrowheads). (C) A native fluoroscopic image demonstrates the microcatheter tip in the distal aspect of the draining vein. (D) Venography from this arterial ostium demonstrates reflux into a network of arterial feeders. (E) A native fluoroscopic image after Onyx embolization demonstrates filling of multiple arterial feeders as well as partial filling of the distal aspect of the frontal draining vein. (F) Six months later, left ICA angiography confirms cure of the lesion. Used with permission from Barrow Neurological Institute.
Patient No 4
Following standard transarterial embolization of a 5-month-old girl with a VOG AVM, a substantial portion of the nidus remained (figure 3A). Transvenous embolization was selected given her persistent symptoms. After transfemoral arterial access was gained in order to perform control angiography, access to the VOG venous pouch was achieved transfemorally (figure 3B, C). Numerous attempts were made using a microcatheter alone to engage the ostium of an arterial feeder. Because of the size and turbulent flow within the VOG, this was not possible. Instead, we navigated a distal access catheter (DAC) into the mid straight sinus (figure 3D). The DAC provided a stable platform through which we successfully catheterized an arterial ostium. Onyx 18 infusion through the microcatheter resulted in a significant reduction in the nidus through collateral embolization of multiple arterial feeders (figure 3E, F). Reflux into the venous pouch did not occur. Follow-up MRI 3 months later demonstrated progressive involution of the VOG and a reduction in ventricular size (figure 3G, H). The patient's symptoms stabilized and she returned at 1 year of age when angiography demonstrated enlargement of several arterial feeders. These were amenable to further transarterial embolization in preparation for stereotactic radiosurgery.

{kind=link}
{kind=link}
{kind=link}
(A) Patient No 4. Sagittal T2 MRI demonstrates a vein of Galen (VOG) arteriovenous malformation (AVM) causing obstructive hydrocephalus. (B, C) Early and late phase vertebral artery (VA) angiography demonstrates the AVM as well as eventual drainage into straight and transverse sinuses. (D) A native fluoroscopic image demonstrates the tip of the distal access catheter (arrowhead) in the straight sinus and the tip of the microcatheter (arrow) in the ostium of an arterial feeder. Note that the existing Onyx cast had been produced during a prior stage of transarterial embolization. (E) Following transvenous to arterial Onyx embolization, a substantially larger cast is produced by collateral filling of multiple arterial feeders. (F) Left VA angiography confirms a substantial reduction in nidus volume. (G, H) Axial MRIs before and 3 months post-treatment demonstrate progressive involution of the VOG and reduced ventricular size. Used with permission from Barrow Neurological Institute.
Results
Four female patients, ranging in age from 5 months to 68 years, were treated in the manner described above. Lesions included two high risk transverse–sigmoid DAVFs, a high risk ethmoidal DAVF, and a VOG AVM. Transvenous to arterial embolization resulted in cures in the first three patients and symptomatic improvement in the fourth patient with a VOG AVM. In all cases, collateral filling of multiple feeding arteries occurred through a single Onyx infusion. No complications occurred.
Discussion
Transvenous Onyx embolization has been reported in small cases series and case reports in a variety of pathologic scenarios. Most commonly, transvenous Onyx infusion has been applied in the treatment of indirect carotid cavernous fistulas.6–9 This technique typically involves the deposition of coils within the cavernous sinus followed by the slow infusion of Onyx to complete the occlusion of the venous drainage system.8 ,9 Obviously, this technique differs from the one we describe in which traversing the venous drainage pouch allowed catheterization of the ostium of an arterial feeder. The penetrating properties of Onyx enabled occlusion of multiple collateral arterial feeders without compromising venous drainage.
Transvenous occlusion of the cavernous sinus is generally well tolerated. The risk of pulmonary embolism is minimal given the relatively small caliber of the veins draining the cavernous sinus, specifically the petrosal sinuses and the ophthalmic veins. Complications have been reported, however, and include cranial neuropathies, bradycardia, asystole, and unintended migration of the agent into the carotid artery.3 ,6 ,8–11 Cranial neuropathies are thought to occur either from compression of the nerves from the embolic mass or chemical irritation from the dimethyl sulfoxide contained within the Onyx preparation.8–10 Similarly, compression or irritation of the trigeminal nerve can produce bradycardia and rarely even asystole through a vagal reflex arc.8–10 ,12 Despite these potential complications, Onyx embolization in this setting offers the advantages of shorter treatment times and greater penetration into the interstices of the cavernous sinus, thereby increasing the likelihood of cure.6
Using a technique similar to ours, Kessler et al5 reported the transvenous to arterial treatment of grade 3 or 4 AVMs in five patients. The authors advised employing a transjugular approach.5 Their rationale for this approach, which we support and employed in the management of our patient with an ethmoidal DAVF, was that this allowed the safe retention of the microcatheter within the jugular vein in cases with substantial reflux.5 The fragile nature of the veins draining an AVM would likely predispose to hemorrhage if an adhesed microcatheter was forcibly extracted. In addition, if a transfemoral approach were used, the retained catheter would traverse the right atrium and expose the patient to the risks of cardiac arrhythmias and thromboembolic complications. The concern over catheter retention and vessel rupture would be diminished with use of a detachable tip microcatheter. Unfortunately, while these catheters are available and widely used in Europe, they are not yet approved for use in the USA.
The effect of catheter adhesion is less of a concern in cases of DAVFs involving the major dural sinuses. In this setting, the dural leaves are substantially thicker than cerebral veins, thus making it far less likely to cause a rupture during catheter extraction. We employed the transjugular approach in the patient with the ethmoidal DAVF because we traversed a cortical vein, which is presumably more delicate than a dural sinus, in order to catheterize the ostium of a feeding artery.
Kessler et al5 argued that the transvenous to arterial approach was optimal in cases with favorable venous architecture or when the transarterial approach was not feasible. Using this approach, they cured four of five patients and substantially reduced the nidus in the last patient.5 Nonetheless, the potential morbidity of this procedure cannot be underestimated. If curative embolization is not accomplished and venous drainage of the AVM is compromised, the risk of subsequent hemorrhage is high. In DAVFs, however, occlusion of the venous drainage is less often detrimental and frequently curative.
Similarly, Dowd et al13 described a technique in which they transvenously catheterized a pericallosal arterial feeder in a 2-year-old patient whom they had previously treated in the perinatal period for a choroidal VOG malformation. The authors did not employ liquid embolysates, choosing instead to coil an enlarged feeding artery.13 While the technique is similar to ours, specifically, navigating through an enlarged VOG, the pathologic entity is not. In their case, the authors addressed a single fistulous feeder to a choroidal malformation. In our case, the use of Onyx allowed collateral embolization of numerous arterial feeders to a true VOG AVM.13
Lin et al14 reported an interesting case in which they cured a purely intraorbital arteriovenous fistula through a transvenous approach. In this case, the authors navigated a microcatheter into a branch of the superior ophthalmic vein and were able to push Onyx in a retrograde fashion to the site of the arteriovenous fistula.14 This technique allowed successful penetration of the fistulous site and resulted in a cure. This report differs from ours as the authors did not attempt, or need to attempt, catheterization of the ostia of feeding arteries.14 The flow properties of Onyx enabled them to cure the fistula from a distal catheter position. In our cases, this technique would have resulted in occlusion of the venous drainage system.14
Finally, Dalyai et al15 reported transvenous Onyx embolization of a cirsoid scalp AVM. In this case, the authors inflated a balloon in the external jugular vein as a means of preventing pulmonary embolism and improving retrograde flow of Onyx into the draining venous pouch.15 Again, this technique differs from ours in that the venous drainage system, rather than the feeding arteries, was occluded.
Our series highlights the efficacy of Onyx on a number of fronts. Importantly, this technique adds to the very limited endovascular treatment options for the management of ethmoidal DAVFs. These lesions are typically supplied by ethmoidal branches of the ophthalmic artery. Superselective catheterization of these small and tortuous branches is often impossible. Even when catheterization is feasible, distal access to a site close to the fistulous communication is exceedingly difficult to achieve. Add to this that embolization through these feeding vessels increases the risk of unintended embolization of, or reflux into, the central retinal artery. Our technique is ideal when there is a sizeable and non-tortuous draining cortical vein. Navigation through the sinuses is straightforward, and a transjugular approach decreases the morbidity of catheter retention and negates concerns over adequate catheter length.
Transarterial Onyx infusion has recently been described as an effective means of treating complex DAVFs.16 Nonetheless, microcatheterization of a position proximal to the fistulous site is not always possible nor does Onyx always penetrate distally enough to be curative.16 The transvenous to arterial technique offers an effective alternative in select cases. Both DAVFs treated and cured in our series were characterized by a recipient venous pouch parallel to the affected transverse and sigmoid sinuses. Navigating from the sinus into the pouch provided a stable position for catheterization of an arterial ostium. Such cases, in which a parallel pouch or a large draining vein allow transvenous navigation into an arterial ostium, are optimal for the transvenous to arterial infusion technique. Presumably, in DAVFs that drain directly into the transverse and sigmoid sinuses and do not have a parallel pouch, stable transvenous to arterial catheterization would be more difficult to achieve and would raise the probability of refluxing Onyx into the normal sinus.
In the case of the VOG AVM, however, we were forced to catheterize an arterial ostium directly opening into an enlarged VOG. An attempt to navigate a microcatheter primarily to this site was not feasible given its lack of stability and navigability within the high flow VOG. By employing a DAC within the straight sinus, a stable platform was constructed that allowed successful microcatherization through the VOG pouch. This technique may also be useful in DAVFs that drain directly into a normal sinus. Successful embolization into multiple arterial feeders in this case likely reduced the hydrodynamic pressure within the VOG and produced an improvement in the patient's hydrocephalus.
Despite the advantages of the transvenous to arterial technique, a number of potential complications must be considered. Reflux into normal cortical veins or dural sinuses can compromise normal cerebral venous drainage and produce stroke or hemorrhage. Theoretically, aggressive transvenous embolization can produce symptomatic pulmonary embolization. Finally, propagation of Onyx into arterial feeders to the cranial nerves or cerebrum can occur with potentially devastating neurological sequelae.
Once again, the transvenous to arterial technique offered an effective treatment option in our patient with a symptomatic VOG AVM. In her case, prior transarterial embolization had been performed but was no longer feasible given the diminutive size and tortuosity of the remaining arterial feeders. The transvenous approach resulted in a further decrease in the size of her nidus and stabilized her symptoms. Presumably, this retrograde means of infusing Onyx could also be applied in patients with choroidal VOG malformations.
Conclusion
This report describes the transvenous to arterial embolization of Onyx for the treatment of DAVFs and a VOG AVM. This technique extends the armamentarium that interventionalists can use for the management of these high risk complex lesions. In particular, transvenous to arterial embolization may make the endovascular treatment of select ethmoidal DAVFs feasible. A variety of catheter techniques are described that facilitate microcatheterization of an arterial ostium. Such catheterization was sufficient to provide collateral embolization of numerous arterial feeders. This technique resulted in cures in three patients and a substantial reduction in AVM nidus in the fourth.
References
Footnotes
-
Contributors All authors contributed to this manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.