Article Text

Abstract
Background Dural arteriovenous fistulae (dAVF) of the anterior fossa have a malignant course since they exclusively drain into cortical frontal veins and warrant aggressive treatment. Classically, these lesions have been treated with microsurgical clipping of the fistulous connection. We describe a transvenous approach for Onyx embolization of these lesions that relies on distal venous access using a flexible new-generation guide catheter.
Methods A retrospective review was performed of all patients with an anterior fossa dAVF treated at the Medical University of South Carolina since 2010. Charts, procedural records, angiographic images and follow-up were reviewed. Three patients were identified.
Results Transfemoral venous access and distal transvenous sinus access was obtained in a retrograde fashion to at least the level of the right transverse sinus. Once a distal guide catheter position was obtained within the venous sinus system, a microcatheter was advanced into the predominant draining anterior frontal cortical vein in preparation for embolization. Onyx 34 embolization was then initiated from this position with the objective of achieving penetration across the vascular shunt.
Conclusions Our experience demonstrates that transvenous Onyx embolization offers an effective and safe alternative to the classic neurosurgical treatment of anterior fossa dAVF.
- Catheter
- Fistula
Statistics from Altmetric.com
Introduction
Among the dural arteriovenous fistulae (dAVF) of the brain, those located in the anterior cranial fossa are most rarely encountered.1–3 These dAVF are fed from the ophthalmic artery via anterior ethmoidal branches, frequently with bilateral supply. Drainage is generally via arterialized frontal cortical veins to the anterior third of the superior sagittal sinus.2 dAVF of the anterior cranial fossa occur more frequently in men than in women and usually in elderly subjects.4 ,5 Since retrograde cortical venous drainage is the most common drainage pattern of dAVF of the anterior fossa, they have a malignant course and most frequently present with hemorrhage, with reported rates of 60–90%.3 ,4 ,6 Thus, even the incidental identification of these lesions warrants aggressive treatment.
Classically, these lesions have been very effectively treated with microsurgical clipping of the fistulous connection with a bicoronal craniotomy and subfrontal approach.3 However, the surgical approach is not without risk. Bifrontal craniotomy can lead to surgical site infection, retraction injury and, at times, frontal sinus breach requiring exoneration and repair. In many instances, patient preference for a less invasive technique may also be a factor in the development of endovascular approaches to traditional surgical lesions. Advances in technique and devices over the past decade have resulted in viable endovascular alternatives to the surgical treatment of a number of vascular pathologies including dAVF.7–9 The introduction of novel, supportive, yet flexible intracranial 6 F guide catheters such as the Neuron family of catheters (Penumbra, Alameda, California, USA) that provide distal access10 ,11 and the availability of the ethylene vinyl alcohol copolymer Onyx (eV3 Neurovascular, Irvine, California, USA) represent two such advances.12–15 We describe a transvenous approach for Onyx embolization of these lesions that relies on distal venous access using a flexible new-generation guide catheter.
Methods
A retrospective review was performed of all patients treated for an anterior fossa dAVF at the Medical University of South Carolina since 2010. Medical records and angiographic images and follow-up were reviewed. Three patients were identified (table 1). None of the patients treated presented with hemorrhage. All presented with headache and, in addition, one patient had right-sided visual acuity loss and left upper extremity symptoms. All patients underwent successful transvenous embolization with immediate angiographic complete occlusion. Follow-up angiography was performed at 2–14 months and showed no recurrent fistula.
Patient table
Results
All procedures were performed under general anesthesia. Using an 18 G Cook needle (Cook Medical, Bloomington, Indiana, USA), a 6 F Pinnacle sheath was placed into the right common femoral vein. While the microcatheter access to the lesion is transvenous, retrograde venography through either the guide or microcatheter is insufficient to delineate the anatomy of the vascular shunt. The placement of a second diagnostic catheter within the internal carotid artery that primarily supplies the dAVF is beneficial to demonstrate the anatomy and provide roadmap guidance. Thus, a 5 F Pinnacle sheath was placed into the right common femoral artery for transarterial access. Patients were anticoagulated with 5000 U intravenous heparin and intermittent boluses were administered to maintain an activated clotting time 2–2.5 times the patient's baseline level.
Distal transvenous access was obtained retrograde across the internal jugular vein (figure 1), whereby the guide catheter can be positioned as far distally as the superior sagittal sinus. This can be performed with a variety of guide and intermediate catheter combinations; some examples are shown in table 1. For example, a triaxial catheter system consisting of a 6 F Shuttle sheath (Cook Medical) with a telescoping 6 F 070 Neuron guide catheter (Penumbra) and a 5 F Select catheter Berenstein tip (Penumbra) was advanced over a 0.038 inch guidewire (Microvention, Tustin, California, USA) to the level of the right transverse sinus. Using a triaxial system with intermediate catheters, the tight ‘Z’ turn of the sigmoid sinus–jugular bulb junction can be navigated. Achieving distal venous access is critical to provide sufficient support and length to deliver the microcatheter. Once a distal guide catheter position was obtained within the venous sinus system, a Marathon microcatheter (ev3 Neurovascular) was advanced over a microwire. In all cases the microcatheter was advanced as far distally within the venous draining system as was possible. Ideally, a microcatheter position immediately adjacent to the fistula is obtained. However, despite deep venous guide access, proximal tortuosity and catheter length constraints can limit the distal venous access achievable.
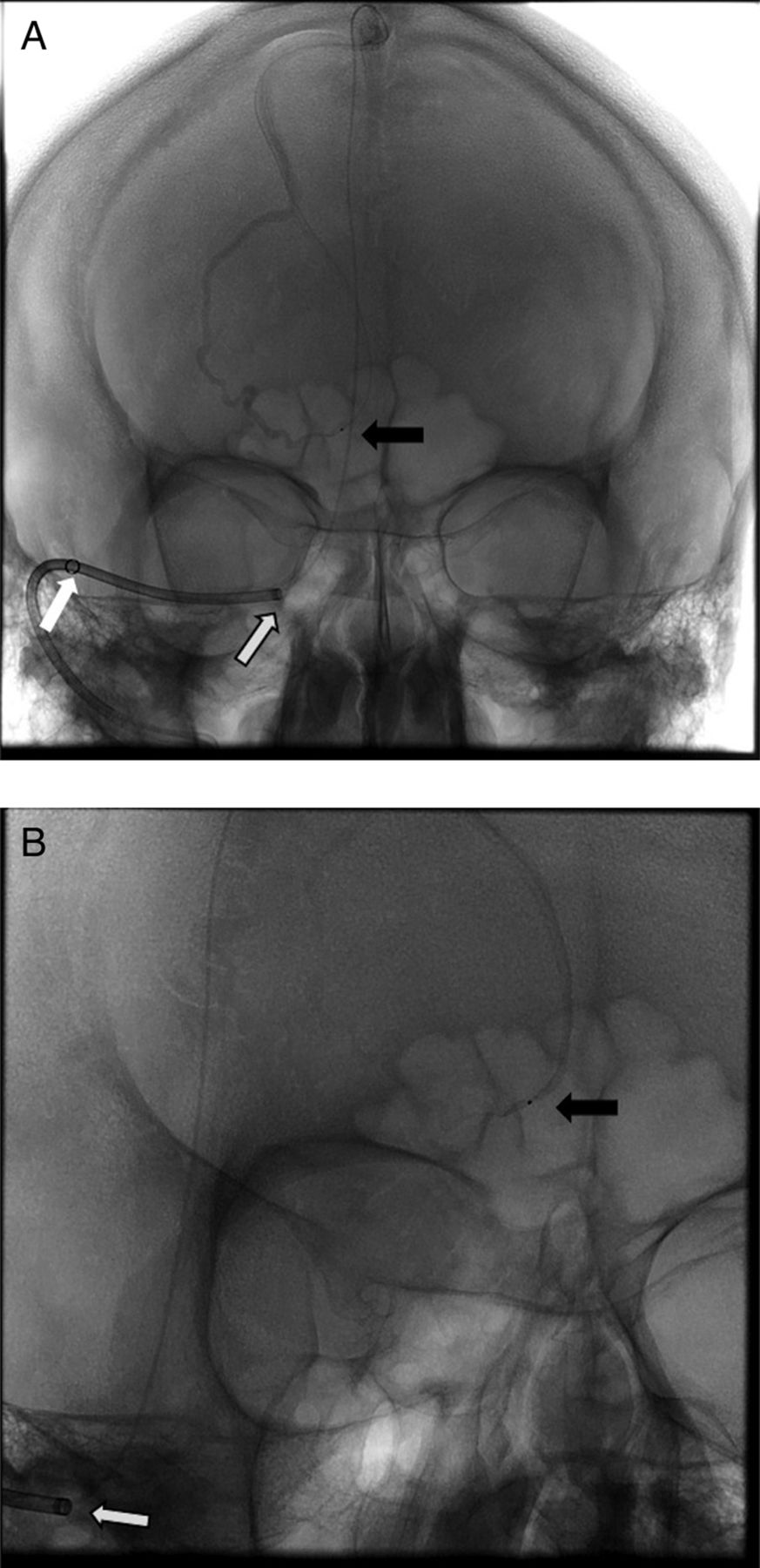
Unsubtracted anteroposterior (A) and transorbital (B) views of the head showing transvenous access across the jugular bulb-sigmoid sinus with a coaxial system consisting of a 6 F Neuron 070 guide (white arrow) with a telescoping Penumbra 041 reperfusion catheter (white arrow, black outline) placed along the distal transverse sinus. A Marathon microcatheter was then navigated over a 0.010 inch microwire into the anterior superior sagittal sinus (black arrow).
Internal carotid angiography was performed with a 5 F diagnostic catheter to delineate the fistulous connection point. Under roadmap guidance with an arterial injection of contrast, the microcatheter was positioned within the predominant draining right anterior frontal cortical vein in preparation for embolization. Onyx 34 embolization was then initiated from this position with the objective of achieving penetration across the vascular shunt (figures 2⇓–4).

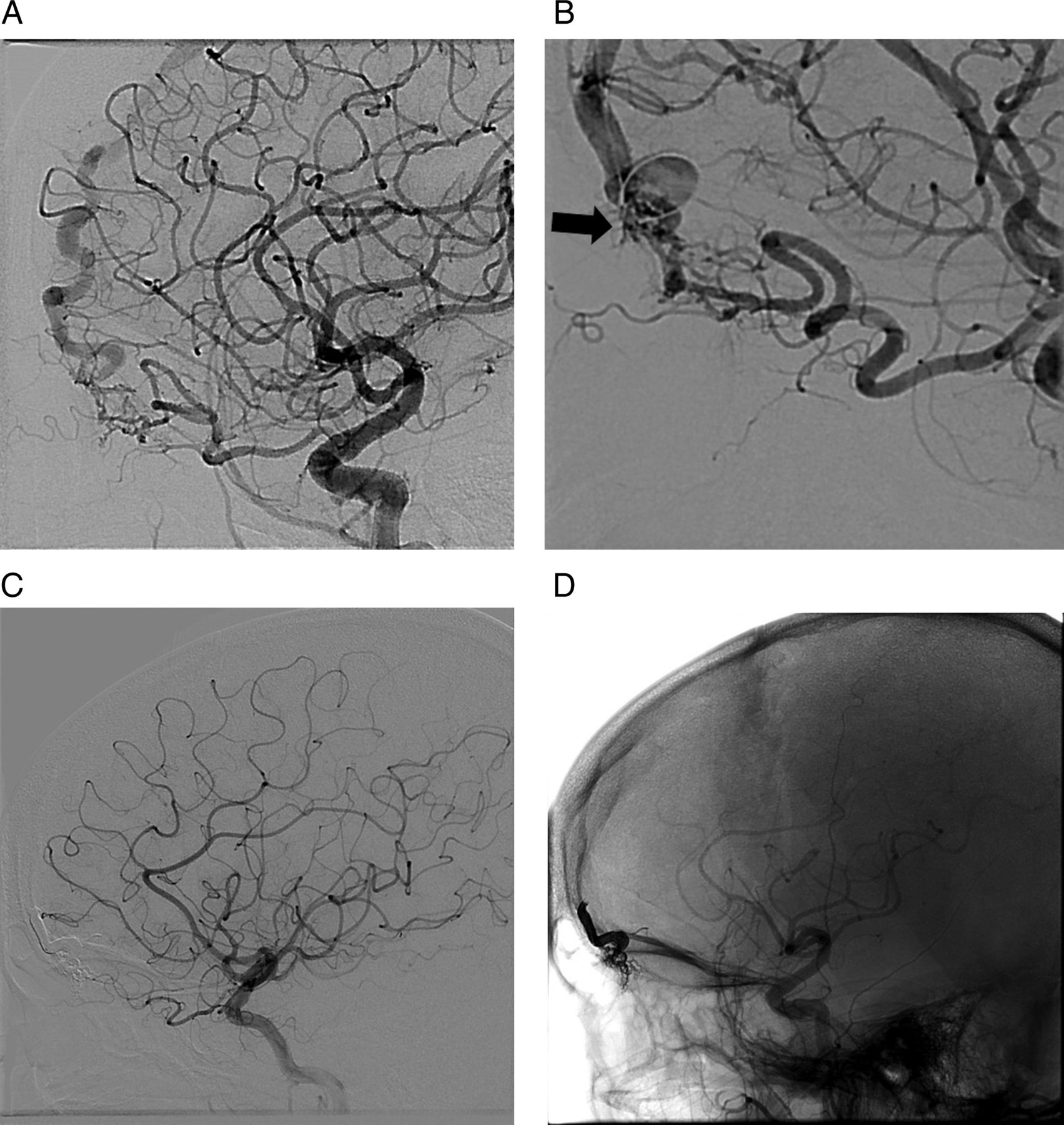
Patient 1. (A) Pretreatment lateral view of a right internal carotid (RICA) angiogram showing an anterior fossa dural arteriovenous fistula (dAVF) supplied by the ophthalmic artery with venous drainage across a dilated frontal cortical vein. (B) Superselective angiography in a magnified lateral projection with a microcatheter injection within the anterior ethmoidal artery showing the vascular shunt across the anterior fossa skull base. (C) Transarterial embolization proved to be challenging, with inadequate penetration into the shunt and residual filling of the dAVF on the post-transarterial embolization RICA angiogram. Transvenous access was obtained and a superselective venogram with a Marathon microcatheter (black arrow) injection within the recipient frontal cortical vein in (D) unsubtracted and (E) subtracted views. Note the lack of contrast opacification across the shunt in this selective venogram, highlighting the importance of having simultaneous transarterial access for contrast administration. (F) Following transvenous Onyx embolization, the Onyx cast penetrates the anterior fossa floor in this unsubtracted lateral view. (G) Following transvenous Onyx embolization, the dAVF is completely occluded.

Patient 2. (A) Pretreatment magnified lateral view of a right internal carotid artery (RICA) angiogram showing another example of a stereotypical anterior fossa dural arteriovenous fistula (dAVF) supplied by the ophthalmic artery with venous drainage across a dilated frontal cortical vein. (B) RICA angiogram shows a Marathon microcatheter positioned within the distal recipient cortical vein (black arrow). (C) Post-treatment RICA angiogram following transvenous Onyx embolization shows complete occlusion of the dAVF. (D) Unsubtracted view showing penetration of the Onyx cast across the skull base.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient 3. (A) Pretreatment magnified lateral view of a right internal carotid artery (RICA) angiogram showing another example of a stereotypical anterior fossa dural arteriovenous fistula (dAVF). (B) RICA angiogram shows a Marathon microcatheter positioned within the distal recipient cortical vein (black arrow). (C) Post-treatment RICA angiogram following transvenous Onyx embolization shows complete occlusion of the dAVF. (D) Unsubtracted view showing penetration of the Onyx cast across the skull base.
Discussion
Dural AVFs supplied by the anterior ethmoidal arteries occurring at the anterior cranial fossa most commonly present with hemorrhage.3 ,4 ,6 ,16–18 These malformations warrant definitive treatment since they follow a malignant course due to a high risk of hemorrhage, even in those found incidentally. Historically, surgical clip disruption with bipolar electrocautery and/or clip application at the fistulous connection point via a subfrontal or interhemispheric approach has been the mainstay of treatment.4 ,19 ,20 More recently, endovascular approaches have been attempted.21–24 However, anterior fossa dAVF present a unique challenge to transarterial21 ,24 superselective embolization since an approach involving the ophthalmic artery is perilous and associated with a risk of retinal infarction. In addition, adequate penetration of Onyx across the small branches of the anterior ethmoidal artery as it courses through the cribriform plate may be difficult to achieve prior to refluxing and compromising the central retinal artery. Deeper penetration typically involves increasing amounts of embolisate material reflux, thus resulting in a narrowing of the safe ‘landing zone’ within the parent artery.
Successful transvenous approaches to dAVF in other locations have been described using available embolic materials prior to the introduction of Onyx.23 ,25 In the Onyx era, some authors have advocated transvenous access for balloon inflation across the predominant draining sinus with concomitant transarterial Onyx embolization.26 ,27 Transvenous coil embolization of anterior fossa dAVF has been described22 ,28 but required direct percutaneous jugular venous access due to the distal location of the fistulous connection along the basal frontal lobe. Conventional guide catheters are too rigid to navigate deeply into the venous sinus anatomy from a transfemoral approach. Alternatively, direct venous sinus access can be obtained with a burr hole craniotomy,2 ,27 ,29 ,30 but this adds surgical morbidity and carries a significant risk of bleeding complications, especially in the setting of anticoagulation. For these reasons, the mainstay treatment of anterior fossa dAVF has remained surgical disconnection and few centers offer endovascular obliteration.
We have described a novel transvenous approach for treating anterior fossa dAVF that relies on two principles for successful completion. First, distal venous access using flexible new-generation guide catheters (Penumbra) must be obtained. These flexible catheters, either in coaxial or triaxial fashion, can be used to effectively negotiate the ‘Z’ turn at the sigmoid sinus–jugular bulb transition and be positioned within the transverse sinus or even the superior sagittal sinus. Navigation of the guide catheter deep into the venous sinus system is essential to allow adequate microcatheter length for sufficiently distal access into the arterialized frontal cortical vein, as well as providing sufficient support for navigation. In addition, distal access is critical to provide the necessary microcatheter support to navigate into the target cortical vein in the frontal lobe. Importantly, simultaneous transarterial access into the internal carotid artery that predominantly supplies the dAVF is necessary to adequately visualize the vascular shunt prior to and during treatment. Venography in the retrograde direction is insufficient to overcome the flow across the fistula and will not opacify the lesion across the skull base. Transarterial contrast injection is necessary to provide a working roadmap image.
Secondly, Onyx penetration across the fistula can be achieved without the degree of concern of possible pedicle reflux that might occur during a transarterial injection of Onyx into the ophthalmic artery tree. Onyx reflux within the recipient cortical vein, although undesirable, is not associated with a risk of cortical infarct since the cortical vein is arterialized and therefore already non-functioning. To achieve distal penetration of Onyx across the fistulous point, it must be pushed against the predominant flow of the fistula. To be successful, time must be invested to create a proximal ‘plug’, allowing the Onyx around the catheter tip (including a small amount which has refluxed) to become dense. Once this plug has been created, further administration of Onyx will be preferentially against the arterialized venous flow and towards the fistula. In none of the three cases described was Onyx delivery to the fistulous point particularly challenging.
We have found this procedure to be highly efficacious and without complications. In all instances deep penetration of the fistulous shunt was achieved with Onyx, achieving disruption of the fistula. This technique provides another useful tool in the armamentarium of the neurointerventionalist.
Conclusion
Our experience shows that transvenous Onyx embolization offers an effective and safe alternative to the classic neurosurgical treatment of anterior fossa dAVF.
References
Footnotes
-
Contributors All authors made a material contribution to this article, the revision of the article and gave their final approval for submission of the article to the journal.
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from the Medical University of South Carolina Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.