Article Text

Abstract
Background Flow diversion represents a major paradigm shift in the treatment of unruptured intracranial aneurysms. The potential impact of this technique on coil utilization and adjunctive techniques such as balloon-assisted and stent-assisted coiling is unknown. In this study, the effect of introduction of flow diversion devices on the utilization of coil and adjunctive techniques was assessed.
Methods A retrospective review was conducted of consecutive patients with unruptured aneurysms treated at our institution comparing two groups: Group 1 (patients treated in the 2-year interval preceding the introduction of the Pipeline Embolization Device (PED) and Group 2 (patients treated during the 2-year interval following introduction in our practice of the PED).
Results Mean aneurysm diameter was 8.7±6.3 mm in Group 1 and 8.5±6.1 mm in Group 2 (p=0.79). PED therapy was employed in 38 (21.7%) of 175 aneurysms in Group 2. The proportion of stent-assisted procedures was significantly less in Group 2 than in Group 1 (6.9% vs 14.7%, p=0.04), as was the proportion of patients undergoing parent artery sacrifice (0.6% vs 3.9%, p=0.046). The mean and median number of coils used per aneurysm were 5.4±3.6 and 5 (range 1–18) for Group 1 and 3.2±3.2 and 3 (range 0–19) for Group 2 (p≤0.0001).
Conclusions Flow diversion represents a disruptive technology. More than one-fifth of unruptured aneurysms at our institution were treated with PED after introduction of this technology, resulting in marked decreases in coil and stent utilization.
- Aneurysm
Statistics from Altmetric.com
Introduction
Flow diversion represents a potentially ‘disruptive’ technology in that it may portend a new paradigm shift in the treatment of intracranial aneurysms. Flow diverters induce changes in intra-aneurysmal and parent artery flow dynamics that eventually trigger intra-aneurysmal thrombosis and aneurysm occlusion.1 At this stage it is unknown how much effect this new technique will have on coil utilization or utilization of other ‘adjuncts’ such as balloon or stent assistance. In our practice, the Pipeline Embolization Device (PED; eV3, Irvine, California, USA) has been available since June 2009 and, in this study, we report the impact of the PED on coil, balloon and stent utilization.
Methods
After IRB approval, we conducted a retrospective review of 256 consecutive patients treated with endovascular embolization for unruptured intracranial aneurysms at our institution between June 2007 and June 2011. Information regarding patient demographics, location and size of the treated aneurysm, number and type of coils used and use of stent assistance or balloon assistance was collected. Paraclinoid aneurysms were classified according to the classification of Bouthillier and coworkers.2 The aneurysms were divided into two groups: Group 1 included aneurysms treated during the 2-year period (15 June 2007 to 14 June 2009) preceding the introduction of the PED in our practice and Group 2 included those treated in the 2-year period following the introduction of the PED (from 15 June 2009, the date of the first placement of the PED in our institution, to 14 June 2011). Patients were evaluated and treated in a standardized fashion by three operators (GL, DFK and HJC) who share the same philosophy of indications for treatment and treatment techniques. The goal of coil embolization was to fill the aneurysm with as many coils as possible as long as it was deemed safe. The procedure was terminated when no additional coils could be safely placed within the aneurysm. For patients undergoing coil embolization, antiplatelet therapy was usually administered each time treatment was considered. Patients undergoing planned stent-assisted coil embolization and PED treatment were loaded with dual antiplatelet therapy (aspirin 325 mg/daily and clopidogrel 75 mg/daily for 5 days). In such cases, post-procedural antiplatelet therapy was continued for at least 3 months, after which clopidogrel was usually discontinued and patients maintained on daily aspirin alone.
In order to provide an index for the impact of PED on overall coil usage, we compared the mean and the median number of coils used per aneurysm in Groups 1 and 2. Continuous data are presented as mean±SD. The χ2 test was used for comparison of proportions and the two-sided t test for comparison of means. Results were considered significant for p values ≤0.05. All statistical analyses were performed with JMP software V.9.0.1 (SAS Institute).
Results
Two hundred and fifty-six patients with 277 unruptured aneurysms were treated with endovascular therapy between June 2007 and June 2011. Ninety-eight patients (mean age 55.9±12.2 years, 75.5% women, 102 aneurysms) were treated between 15 June 2007 and 14 June 2009 (Group 1, Pre-PED) and 158 patients (mean age 55.3±12.9 years, 82.9% women, 175 aneurysms) were treated between 15 June 2009 and 14 June 2011 (Group B, Post-PED). The mean diameter of the treated aneurysms was 8.7±6.3 mm in Group 1 and 8.5±6.1 mm in Group 2 (p=0.79). The location of the treated aneurysms is indicated in table 1. There was no significant difference in location between the two groups.
Location distribution of unruptured aneurysms
PED therapy was employed in 38 (21.7%) of 175 aneurysms in Group 2. Balloon assistance was used in 27 (26.5%) of 102 aneurysms in Group 1 and 32 (18.3%) of 175 aneurysms in Group 2 (p=0.12). Stent-assisted coiling was performed in 15 (14.7%) and 12 (6.9%) of the procedures in Groups 1 and 2, respectively (p=0.04). Parent artery occlusion was used in four cases (3.9%) in Group 1 and one case (0.6%) in Group 2 (p=0.046).
In Group 1 the mean and median number of coils used per aneurysm were 5.4±3.6 and 5 (range 1–18), respectively. In Group 2 the mean and median number of coils used per aneurysm were 3.2±3.2 and 3 (range 0–19), respectively (p≤0.0001, table 2). Two size and location matched aneurysms treated in Groups 1 and 2 are shown in figures 1 and 2.
Features of aneurysms and treatments

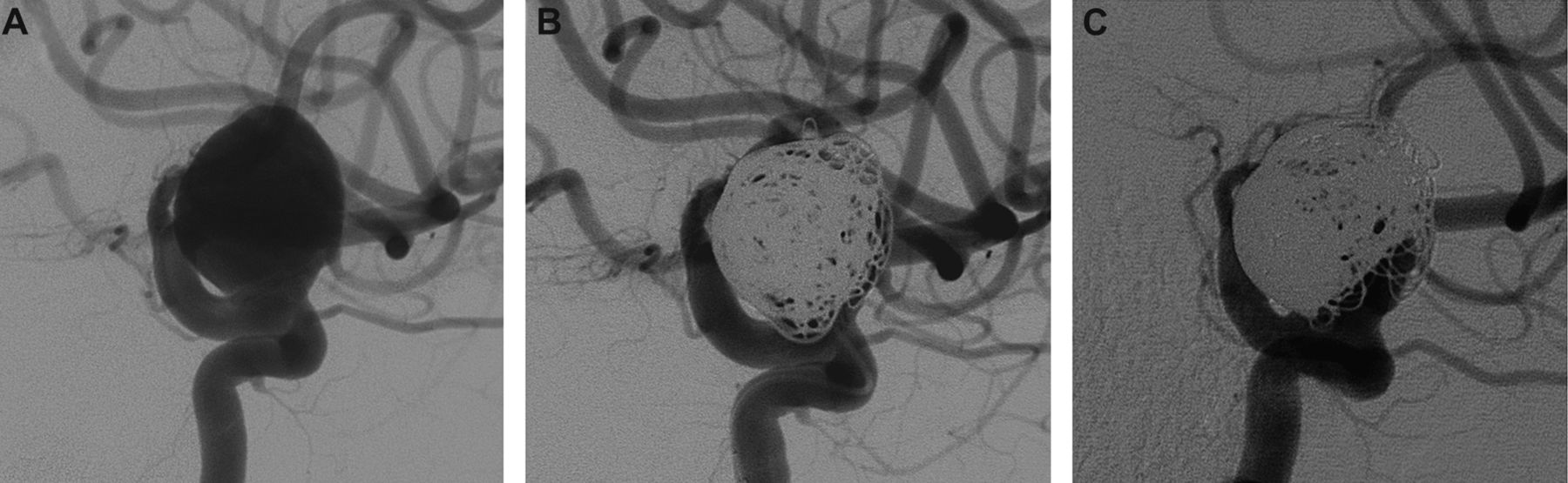
A 52-year-old patient was diagnosed with an incidental very large left carotid–ophthalmic aneurysm in early 2009 (A, anterior-posterior digital subtraction angiogram). The aneurysm was treated with platinum coils with a good initial result (B); however, a follow-up angiogram 6 months later showed aneurysm recurrence (C).

{kind=link}
{kind=link}
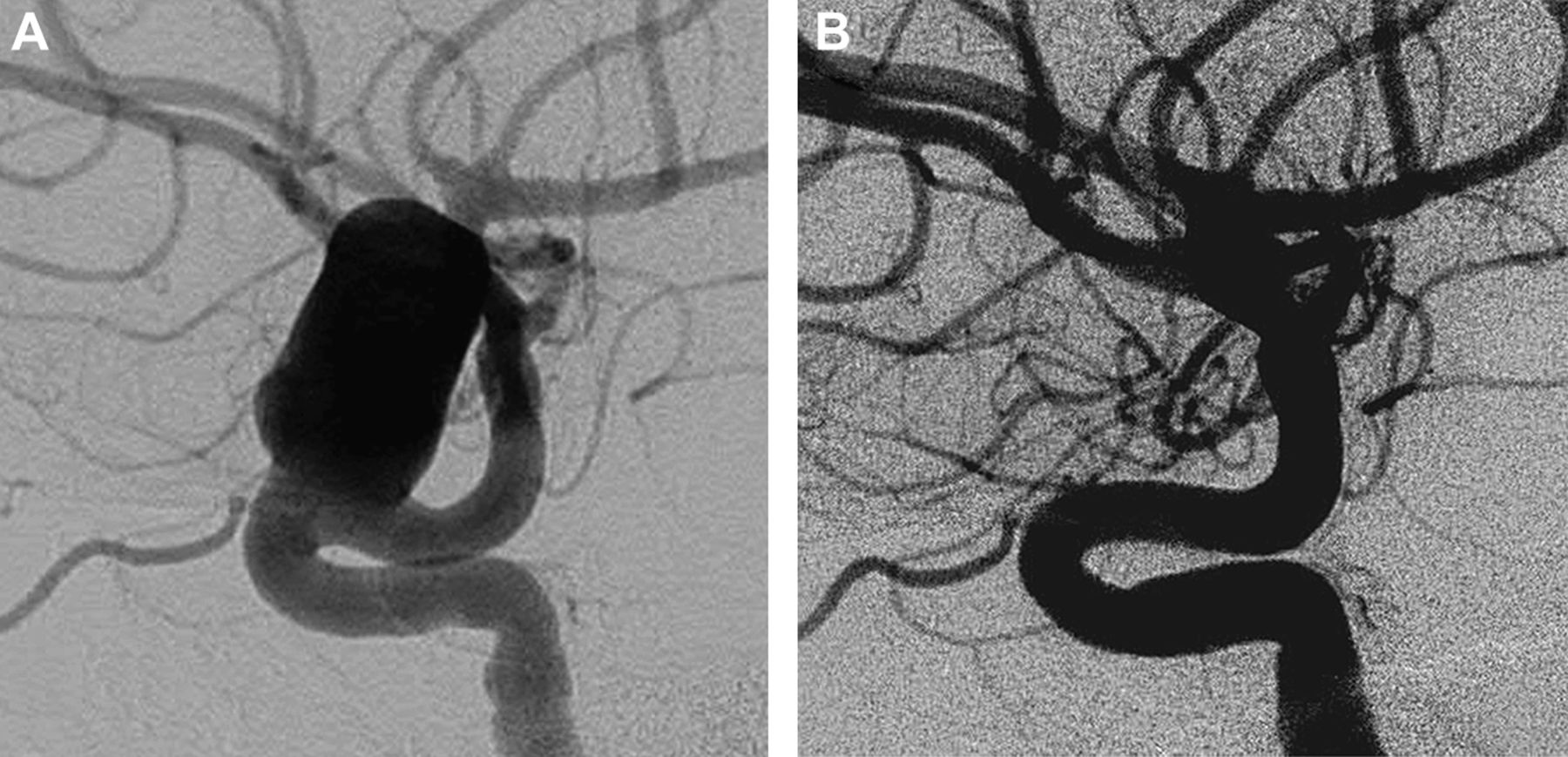
A 58-year-old woman presented with non-specific visual complaints and was found to have a very large carotid–ophthalmic aneurysm (A) which was treated with three telescoping flow diverters. Angiographic follow-up 6 months later showed complete occlusion of the aneurysm (B).
Discussion
In this study we have shown that the introduction of flow diversion technology had a profound impact on our practice patterns. More than one-fifth of patients treated since we gained access to the PED were treated with flow diversion rather than coil embolization. Further, even though aneurysms were of similar mean diameter before and after PED utilization, our coil usage fell by more than 40% on a per aneurysm basis while stent usage dropped by half. Thus, based on our institution's experience, the PED indeed represents a ‘disruptive’ technology.
To our knowledge, no previous study has evaluated the impact of flow diversion on practice patterns. Available case series of PED therapy provide ample evidence of the safety and efficacy of the device.1 ,3–5 However, these previous case series do not provide insight into the impact of flow diversion on clinical practice. Combining the promising data from previous case series with utilization data from our current study, it is likely that flow diversion will lead to a substantial impact on coil and stent usage.
Our study has several important limitations. First, the concomitant use of coils in conjunction with flow diversion technology, as proposed by several investigators, may affect how much flow diversion will diminish overall coil utilization. Since we rarely use coils with flow diversion, we are unable to address this potential effect. Second, this was a retrospective case series with potential bias in case selection. Third, we limited our use of the PED to paraclinoid aneurysms, as required by regulatory requirements during the duration of the study. It is likely that off-label use of the PED will be widespread, which will serve to further diminish coil and stent utilization.
In conclusion, flow diversion represents a major paradigm shift in the endovascular treatment of unruptured intracranial aneurysms and may ‘change’ the endovascular landscape. In our practice, introduction of the PED for the treatment of complex proximal ICA aneurysms has resulted in a significant decrease in the number of coils used in the treatment of unruptured aneurysms as well as a significant decrease in the number of stent-assisted coiling procedures. While strictly limiting the utilization of the device mostly to ‘on-label’ use, flow diversion already represents about 22% of the endovascular procedures performed for unruptured intracranial aneurysms.
Footnotes
-
Competing interests None.
-
Ethics approval The ethics approval was provided by Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.