Article Text

Abstract
Objectives Experience of flow control techniques during endovascular treatment of intracranial dural arteriovenous fistulas (DAVFs) using the Onyx liquid embolic system is reported, with an emphasis on high flow shunts.
Methods Data were evaluated in patients with DAVFs treated endovascularly with Onyx. Adjunctive techniques with coils, acrylics and balloon assistance were utilized to reduce the rate of flow with transarterial and transvenous approaches.
Results The following types of adjunctive techniques were used in 58 patients who underwent a total of 84 embolization sessions with Onyx: transvenous coiling with transvenous or transarterial Onyx embolization in 36 patients, transarterial coiling with transarterial Onyx embolization in eight patients, arterial or venous balloon assisted technique with transarterial or transvenous Onyx embolization in 11 patients, transarterial high concentration acrylics with transarterial Onyx embolization in one patient and staged transarterial or transvenous coiling and Onyx embolization in two patients. Complete obliteration of the fistulae was achieved in 41 patients (70.7%) and 27 patients (65.9%) with high flow fistulae after endovascular treatment alone. Periprocedural complications were encountered in 16 patients, and 13 complications were associated with the adjunctive techniques. There were four neurologic and two non-neurologic clinical sequelae. Distal Onyx migration occurred in four, microcatheter retention in three and cranial neuropathy in three patients. There was one instance each of cerebellar hemorrhage, thromboembolism, coil stretching and retention, and dissection. 56 survivors experienced complete resolution or significant improvement of their symptoms on follow-up.
Conclusions Flow control techniques are safe and effective adjunctive methods in primary endovascular Onyx embolization of high flow DAVFs.
Statistics from Altmetric.com
Introduction
Dural arteriovenous fistulas (DAVFs) are abnormal connections between arteries and veins which may involve the intracranial dura mater. Aggressive clinical symptoms and poor long term outcomes are associated with these pathological conditions when they involve cortical and deep venous drainage. Endovascular occlusion of the fistulous connections with embolic agents such as coils, acrylics and particles may definitively cure DAVFs.
Since the liquid embolic agent Onyx (ev3 Inc, Irvine, California, USA) was approved for presurgical embolization of cerebral arteriovenous malformations by the US Food and Drug Administration in 2005,1 Onyx based embolization has been a key off-label therapeutic option for DAVFs.2–5 High flow shunting occurs frequently in DAVFs. Embolization with Onyx alone for these high flow lesions may risk migration of Onyx distally into the venous system resulting in untoward venous outflow obstruction or pulmonary embolism. Endovascular flow control techniques can reduce the rapid flow within the fistulous connections as well as prevent inadvertent Onyx reflux. Our previous study showed that the balloon assisted technique (BAT) is a safe and effective adjunctive method for transarterial Onyx embolization of complex DAVFs.6 In this study, we describe our experience using the flow control techniques of coils, acrylics and balloon assistance for Onyx based embolization of DAVFs through both the transarterial and transvenous approaches.
Methods
Patient population
We retrospectively reviewed a database of patients with intracranial DAVFs treated with endovascular Onyx embolization at our institution between September 2005 and September 2010. We identified patients with DAVFs who underwent Onyx based embolization with adjunctive coil embolization, acrylic injection and BAT. We evaluated the location and type of fistula, arterial supply, presence of cortical vein involvement or varices, approach of Onyx embolization, adjunctive flow control technique, procedural complication, and angiographic and clinical outcome.
Types of lesions
Based on the presence of cortical or retrograde venous sinus drainage, DAVFs were classified by the Cognard grade system as the following2: type I, drainage into a sinus with normal antegrade flow; type II, drainage into a sinus with retrograde flow in the sinuses only (IIa), into cortical veins only (IIb) or into both (IIa+IIb); type III, direct drainage into a cortical vein without venous ectasia; type IV, direct drainage into a cortical vein with venous ectasia. Cavernous DAVFs were characterized by the following Barrow classification7: type B, type C and type D, indirect fistula between the cavernous sinus and meningeal branches of the internal carotid artery (ICA) only, meningeal branches of the external carotid artery (ECA) only, or meningeal branches of both the ICA and ECA, respectively.
Endovascular Onyx embolization technique
Two types of Onyx liquid embolic material, Onyx 34 and Onyx 18, were used. Onyx 34 has a higher viscosity than Onyx 18, resulting in greater and more rapid cohesion of the injected material and less fragmentation in the flow stream. Therefore, Onyx 34 was used for high flow fistulae to minimize the likelihood of distal Onyx migration into the outflow veins. Onyx 18 has lower viscosity and thus better penetration, so it was utilized when distal migration was felt to be less likely.
The following types of adjunctive flow control techniques for Onyx embolization were used: (1) transvenous coiling with transarterial Onyx embolization; (2) transvenous coiling with transvenous Onyx embolization; (3) transarterial coiling with transarterial Onyx embolization; (4) transarterial high concentration n-butyl cyanoacrylate (NBCA; Trufill, Cordis Neurovascular Inc., Miami Lakes, FL, USA) with transarterial Onyx embolization; (5) arterial BAT with transarterial Onyx embolization; (6) arterial BAT with transvenous Onyx embolization; (7) venous BAT with transarterial Onyx embolization; and (8) venous BAT with transvenous Onyx embolization.
When transarterial Onyx embolization was preferred, the larger feeding arteries from the ECA or ICA were catheterized distally. The tip of the Onyx compatible Marathon or Echelon-10 microcatheter (ev3 Inc) was navigated to a position as close to the fistula site as obtainable. Then the ‘reflux hold reinjection’ technique for Onyx embolization was performed. In high flow fistulae, we decreased the flow within the fistulous connections with detachable coils and high concentration NBCA through the arterial approach prior to the Onyx embolization.
We also occluded the non-dominant recipient venous outlet or varix with coils through the venous approach to prevent distal Onyx migration.
When transvenous Onyx embolization was undertaken, we reduced the flow within the fistulous connection with coil packing of the dural sinus through the venous approach prior to the Onyx embolization. This coil mesh minimized the risk of distal Onyx migration into the venous circulation.
Arterial or venous BAT was used with the Onyx compatible HyperForm or HyperGlide balloon catheters (ev3 Inc).6 In arterial BAT, the balloon catheter was positioned in the feeding artery proximal to the tip of another microcatheter used for transarterial Onyx embolization. The balloon was temporarily inflated in order to slow the flow to aid plug formation and control of Onyx penetration. Arterial BAT was also used to protect the normal cerebral vasculature during transvenous Onyx embolization. The Onyx compatible balloon was temporarily inflated in the ICA adjacent to the fistula to prevent Onyx from occluding the intracranial artery and distal embolism via extracranial–intracranial anastomoses.
In venous BAT, the balloon catheter was navigated transvenously and positioned in the recipient venous structure adjacent to the fistula during transarterial or transvenous Onyx embolization. Temporary balloon occlusion was used to prevent untoward distal Onyx migration into the functional venous sinus and adjacent key cortical veins and to force Onyx to reflux into the adjacent fistulous connections.
Follow-up
Patients with incompletely occluded fistulae were offered surgical disconnection treatment and/or stereotactic radiosurgery. Follow-up digital subtraction angiography at 3 months was performed, especially in patients with incompletely occluded fistulae. If fistulae cure was noted on follow-up angiograms, no further angiographic follow-up was performed. Clinical assessment was performed at the 1 month, 3 month or 6 month follow-up.
Results
Patient demographics
Fifty-eight patients were treated with Onyx embolization in combination with adjunctive flow control techniques. There were 33 women and 25 men, ranging from 12 weeks to 88 years of age. The main clinical presentations included ocular symptoms in 27 patients, cranial nerve palsy in 13, bruit and/or pulsatile tinnitus in 24, headache in 10, intracerebral hemorrhage in six, cognitive decline in two, vertigo in two, gait disturbance in one and intractable nausea in one patient. Five patients had previous endovascular treatment or unsuccessful surgical treatment at other institutions.
DAVFs involved the transverse sigmoid sinus (TSS) (n=20), the cavernous sinus (n=18), the tentorium (n=5), the clivus (n=5), the sphenoidal region (n=2), the superior sagittal sinus (SSS) (n=1), the torcular herophili (n=2), the falx cerebri (n=1), the hypoglossal canal (n=1) and the marginal sinus (n=1). Two patients had multiple DAVFs.
Forty non-cavernous DAVFs were classified as Cognard type I (n=5), type IIa (n=10), type IIb (n=3), type IIa+IIb (n=7), type III (n=5) or type IV (n=10). Eighteen cavernous DAVFs were classified as type B (n=4) or type D (n=14). DAVFs were supplied by multiple branches of the ECA and ICA or vertebral artery in 45 patients. High flow shunts were found in 41 patients. Thirty-one lesions had cortical venous involvement. Variceal development was found in 18 patients.
Endovascular treatment
Fifty-eight patients underwent a total of 84 embolization sessions with Onyx. Sixty-seven procedures were performed with flow control (table 1) while 17 procedures solely utilized Onyx. Primary occlusion was accomplished with Onyx 34 in 24 procedures, Onyx 18 in 34 procedures and a combination of Onyx 34 and Onyx 18 in 26 procedures. In 55 adult patients and three pediatric patients, the mean volume of contrast was 257 ml and 49 ml, and the average fluoroscopy time was 75 min and 84 min, respectively. Among 67 embolization sessions using flow control, 31 were transarterial and 36 transvenous.
Summary of different flow control techniques with Onyx embolization
Adjunctive transvenous coiling with transarterial Onyx embolization was performed in four patients with DAVFs involving the tentorium (n=2), clivus (n=1) and TSS (n=1). After the venous targets were occluded by coils, the fistulae were embolized with Onyx through the ascending pharyngeal artery, occipital artery and middle meningeal artery, respectively.
Adjunctive transvenous coiling with transvenous Onyx embolization was performed in 32 patients. Treated DAVFs involved the cavernous sinus (n=17), TSS (n=7), clivus (n=3), marginal sinus (n=1), hypoglossal canal (n=1) and sphenoidal region (n=1). In another two patients with multiple DAVFs, the dominant fistulae both involving the TSS were treated. In 17 cavernous DAVFs, the cavernous sinus and superior ophthalmic vein were catheterized and occluded by coils through the facial vein (n=8), inferior petrosal sinus (n=8) or direct percutaneous puncture (n=1).
Adjunctive transarterial coiling with transarterial Onyx embolization was performed in eight patients. Treated lesions involved the TSS (n=3), tentorium (n=2), cavernous sinus (n=1), falx cerebri (n=1) and sphenoidal region (n=1). Reduction of flow with coils was performed through the feeding arteries from the ECA or posterior meningeal artery of the vertebral artery. Onyx injections were performed through the feeding arteries, including the middle meningeal, occipital, accessory meningeal, internal maxillary, ascending pharyngeal and posterior meningeal arteries.
Two patients were treated by staged adjuctive coiling and Onyx embolization. In one patient with a TSS DAVF, the varix and TSS was transvenously occluded by coils, then the fistula was embolized with Onyx through the occipital artery. In the second session, the fistula was occluded with coils through the middle meningeal artery followed by transarterial Onyx embolization through the middle meningeal and occipital arteries. In another patient with a TSS DAVF, the high flow within the fistula was controlled by coils through the occipital artery followed by transarterial Onyx embolization through the occipital and middle meningeal arteries. In the second session, the sigmoid sinus was occluded by coils and Onyx was injected through the transvenous approach.
Adjuctive transarterial high concentration acrylics with transarterial Onyx embolization was used in one torcular DAVF patient over two embolization sessions. Acrylic based flow control was accomplished through the occipital, middle meningeal and accessory meningeal arteries followed by Onyx embolization through other feeding arteries of the ECA. In a third session, the varix was occluded by transvenous coiling followed by transvenous Onyx embolization.
Thirteen adjunctive BAT procedures were used in 11 patients, including arterial BAT with transarterial Onyx embolization in seven sessions, arterial BAT with transvenous Onyx embolization in one session, venous BAT with transarterial Onyx embolization in four sessions and venous BAT with transvenous Onyx embolization in one session. In venous BAT, the balloon was used to temporarily occlude the SSS or TSS in order to protect the adjacent key cortical veins during transarterial or transvenous Onyx embolization. There were two sessions of venous BAT in one patient with a SSS DAVF. One patient with a TSS DAVF underwent an additional arterial BAT session during transarterial Onyx embolization.
Adjunctive arterial BAT with transarterial Onyx embolization was used in seven DAVFs. There were five TSS, one tentorial and one torcular DAVF. Balloons were temporarily inflated in the occipital (n=6) and middle meningeal (n=1) arteries during the transarterial injection of Onyx. In one torcular DAVF, transarterial high concentration acrylic was injected into the posterior meningeal artery prior to the arterial BAT. In one patient with a clival DAVF, arterial BAT was used to protect the ICA during transvenous Onyx injection into the clival plexus (figure 1).
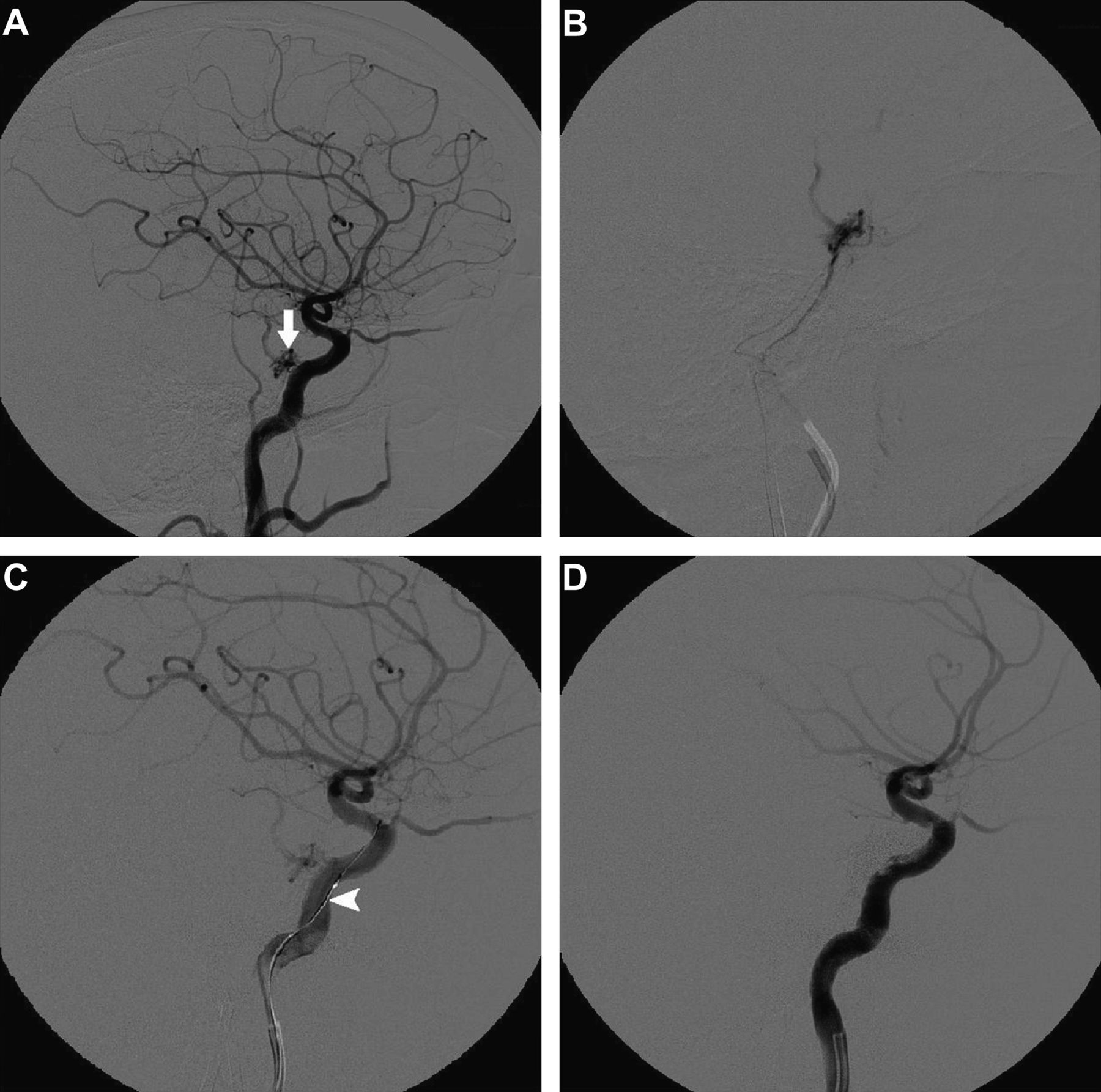
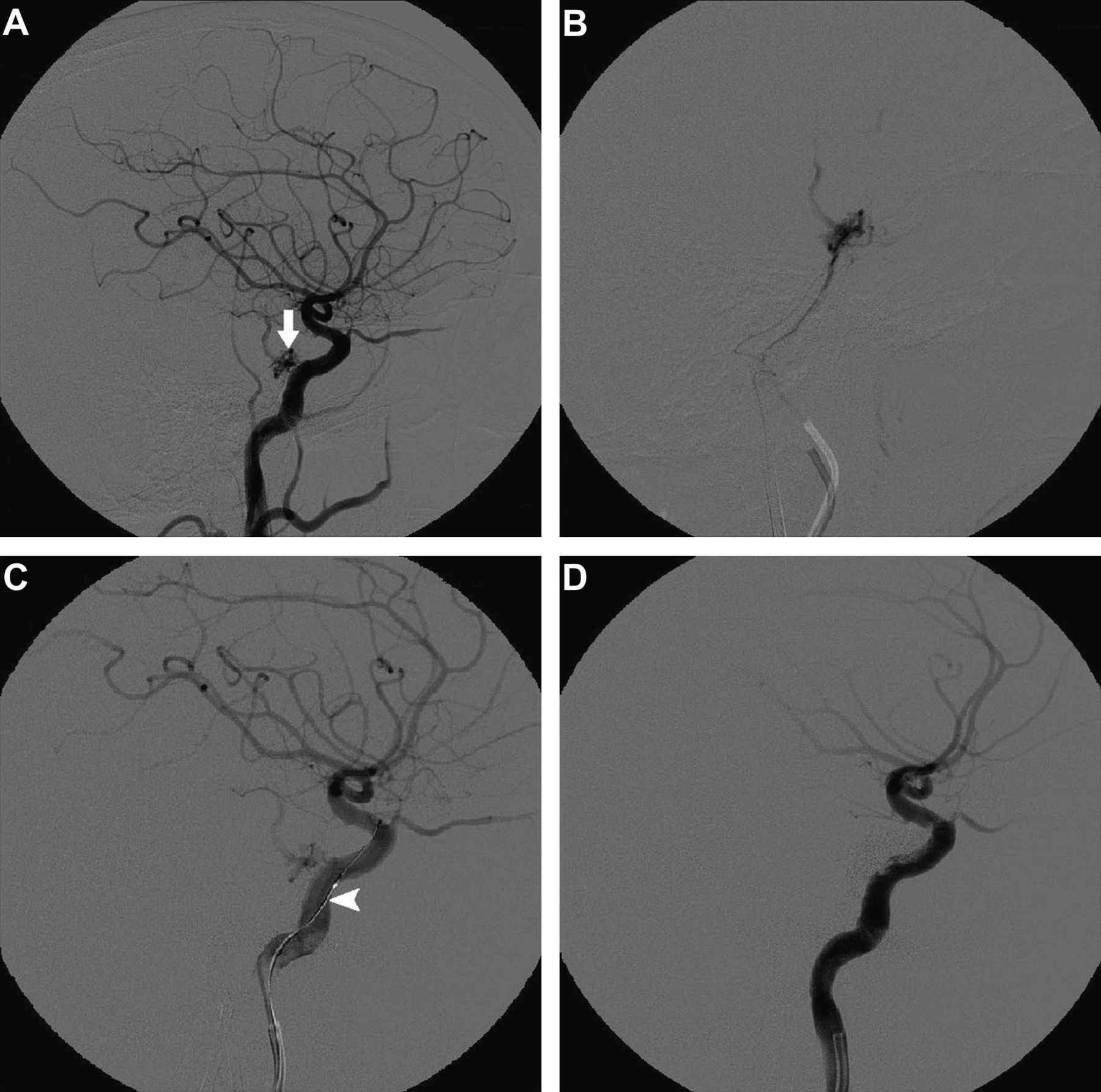{kind=link}
A 68-year-old woman presented with a clivus dural arteriovenous fistula which was treated by transvenous Onyx embolization with arterial balloon assisted technique. The fistula (arrow) is fed by the bilateral inferolateral trunk of the cavernous internal carotid artery (ICA) with clival venous plexus drainage and then the right uncal vein ((A) right common carotid artery angiogram; (B) superselective angiogram of the right clival plexus). The fistula was completely occluded by transvenous Onyx 34 and Onyx 18 injection into the clival plexus through the bilateral inferior petrosal sinus approach with balloon assistance in the ICA ((C) during embolization right ICA angiogram, arrowhead indicates the balloon; (D) post embolization right ICA angiogram).
Angiographic and clinical outcome
Cerebral angiograms obtained after embolization demonstrated complete occlusion of the fistulae in 35 patients, near complete (90–99%) occlusion in 18 patients and partial occlusion in five patients. The fistulae were cured with a primary transarterial approach in nine patients and a transvenous approach in 26 patients. Three patients with incomplete occlusion underwent subsequent treatment by surgical disconnection or stereotactic radiosurgery. One patient with a tentorial DAVF was cured after surgical clipping of the varix.
Angiographic follow-up examinations were performed in 31 patients at 1–32 months after treatment. Twenty-one fistulae with anatomical cure remained permanently occluded at angiographic follow-up. Among 10 fistulae with near complete occlusion, six fistulae had progressive anatomical cure between 2 and 32 months. The other four lesions remained nearly occluded without further embolization. Anatomic cure with endovascular treatment alone was achieved in 41 patients (70.7%).
In the subgroup of 41 patients with a high flow fistula, post embolization cerebral angiograms demonstrated complete occlusion in 22 patients (53.7%), near complete (90%–99%) occlusion in 14 patients (34.1%) and partial occlusion in five patients (5.2%). Twenty-one patients had angiographic follow-up examinations. Five fistulae with near complete occlusion had progressive anatomical cure. In total, 27 of 41 patients (65.9%) with high flow fistulae had anatomic cure with endovascular treatment alone.
Forty-eight patients had clinical cure, and eight patients experienced symptom improvement. Two patients presenting with intracerebral hemorrhage died after a family decision was made to withdraw care due to poor prognosis. The remaining four patients presenting with intracerebral hemorrhage did not have recurrent hemorrhage during the follow-up period. In this series, the mean angiographic and clinical follow-up times were 8.3±9.7 months and 4.1±6.6 months, respectively. All survivors experienced either complete resolution or significant improvement of their symptoms. In the subgroup of 41 patients with high flow fistulae, 34 patients had clinical cure, five patients had symptom improvement and two patients died.
Complications
Periprocedural complications were encountered in 16 patients. Table 2 shows the complications associated with treatment. Thirteen complications were associated with the adjunctive flow control techniques in 67 procedures whereas three complications were associated solely with the Onyx embolization in 17 procedures (patient Nos 14, 15 and 16 in table 2). Procedures with adjunctive flow control techniques had similar complication rates compared with those with Onyx embolization alone (19.4% (13 of 67 procedures) vs 17.6% (3 of 17 procedures), p=1).
Summary of 16 patients with complications after endovascular treatment
Distal Onyx migration occurred in four patients, two of which were asymptomatic. One patient experienced Onyx migration into the lung and presented with pulmonary embolism 1 month post embolization. Femoral artery thrombosis also occurred in this patient at 2 weeks which required surgical thrombectomy. In one patient, Onyx refluxed into the cavernous ICA during Onyx embolization through the ECA feeding artery. Although this did not result in flow obstruction, the patient died from his initial hemorrhage.
Three patients had new or worse cranial neuropathy. Microcatheter fracture in the ECA occurred in three patients associated with transarterial Onyx embolization. The fractured segment was successfully retrieved in one patient. Two other patients experienced microcatheter retention during transvenous Onyx variceal embolization. One patient had a cerebellar hematoma after complete occlusion of a TSS DAVF, which required surgical evacuation. This patient had residual imbalance at the 9 month follow-up. In one patient, a thromboembolic occlusion in a middle cerebral artery branch occurred after Onyx embolization. The occluded vessel was completely recanalized by intra-arterial thrombolysis. Both asymptomatic coil stretching and dissection occurred in one patient.
In the subgroup of 41 patients with high flow fistulae, procedural complications occurred in 14 patients. Eleven complications were associated with the adjunctive flow control techniques whereas three complications were associated with Onyx embolization alone.
Discussion
Endovascular embolization with Onyx is increasingly useful for cerebral arteriovenous malformations and DAVFs. However, in high flow lesions or large diameter vessels, Onyx, as with acrylics and particles, can pass through the shunt, resulting in distal embolism.2–5 ,8 In this study, we used a variety of adjunctive endovascular techniques for the Onyx based embolization. All techniques were performed in order to decrease the flow within the fistulous connections, thus minimizing the risk of distal Onyx migration into the venous circulation and to allow for more accurate Onyx deposition and penetration into the fistula. In addition, arterial and venous BAT can prevent Onyx from entering key vessels.
Results from this study suggest that patients with high flow DAVFs can achieve a high anatomic cure rate and favorable clinical outcomes after Onyx based embolization in combination with flow control techniques utilizing coils, acrylics or balloon assistance. The rates of anatomic cure with endovascular treatment alone observed in this study were 70.7% in all 58 patients with DAVFs and 68.3% in 41 patients with high flow fistulae. These results were comparable with other studies.2 ,5 ,7–9
Favorable clinical outcomes were achieved in 56 patients after endovascular Onyx treatment, and 48 patients had clinical cure during follow-up. More than 80% of our patients experienced clinical cure without permanent morbidity, similar to rates in other studies.2 ,5 ,8 Sixteen patients had complications after endovascular Onyx embolization. These complications were not unique to our study, and our symptomatic complication rate was similar to those in other studies.2 ,4 ,5 ,8 ,9 Distal Onyx migration occurred in four patients during Onyx embolization, resulting in the early termination of Onyx injection. Nonetheless, the flow controlling techniques utilized in this study allowed us to limit the Onyx migration to key cranial veins.
New or worse cranial nerve palsies occurred in three patients with adjunctive venous coiling followed by arterial Onyx embolization in two patients and venous Onyx embolization in another one patient. These complications may be related to cranial nerve ischemia from inadvertent vaso nervorum compromise by Onyx, or mass effect of embolic material.7 ,8
In this study, we have described various methods of flow control during endovascular Onyx embolization of intracranial DAVFs. Flow control is only used when direct Onyx injection (arterial or venous) is not likely to achieve good penetration of the fistula without untoward venous or arterial occlusion. However, the detailed criteria used to select a given flow control technique are complex. The angioarchitecture of the fistula is an important determinant of technique selection. Given the small number of patients treated with each individual flow control technique in our series, the relative merits of each individual technique for DAVF cannot be overemphasized.
Conclusion
Flow control techniques utilizing coils, acrylics or balloon assistance are safe and effective adjunctive methods in primary endovascular Onyx embolization of high flow DAVFs. These adjunctive methods do not increase the procedure related serious complications after endovascular treatment. With more experience, these techniques may result in more anatomic cures and improved safety during Onyx embolization of DAVFs.
References
Footnotes
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Z-SS is supported by the Program for New Century Excellent Talents in University of China (NCET2011), National Natural Science Foundation of China (81070949) and Fundamental Research Funds for Central Universities, Sun Yat-sen University (09ykpy38).
-
Competing interests GD is a paid consultant for ev3 Inc.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was provided by the local institutional review board at UCLA Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.