Article Text

Abstract
Background and aim High resolution MR imaging (HRMRI) has been used to study intracranial atherosclerotic plaques. How HRMRI guided our decision making process in endovascular intervention of basilar artery (BA) atherosclerotic disease is reported.
Methods 3 patients with symptomatic BA atherosclerotic disease underwent BA wall HRMRI under a 3 T MR scanner. Endovascular intervention was then performed utilizing HRMRI findings to guide therapy and to aid in planning the intervention.
Results HRMRI clearly identified the eccentric atherosclerotic plaque at the opposite side of the adjacent right anterior inferior cerebellar artery in one patient and left posterior cerebral artery in one patient, and eccentric atherosclerotic plaque protruding BA lumen at the opposite side of the adjacent right anterior inferior cerebellar artery in the remaining patient. The BA stenosis was stented without compromise of the adjacent branch arteries in the three patients.
Conclusion HRMRI may be used to delineate the eccentric atherosclerotic plaque and the ostia of the major side branches of BA. The HRMRI findings seem helpful in guiding BA stenting with reduced complication risk.
Statistics from Altmetric.com
MR angiography, CT angiography or digital subtraction angiography are effective diagnostic tools for evaluating the mechanisms of transient ischemic attack (TIA) or ischemic stroke. However, vascular imaging from these studies often shows luminal narrowing rather than vascular wall pathology. One of the major advances in neuroimaging over the past decade has been direct visualization of the arterial wall by high resolution MR images (HRMRI).1–3 HRMRI has been used to characterize atherosclerotic plaques,1–5 dissection4 5 and vasculitis.5 It has also been used to detect small branch occlusive disease at or near the origin of small perforators and guide antithrombotic therapy,6–8 and to study remodeling of intracranial artherosclerosis.9 The aim of our current study was to investigate HRMRI guided endovascular intervention of basilar artery (BA) disease.
Methods
Subjects
Three patients with symptomatic BA disease were referred to our hospital for endovascular therapy. Patient demographics, atherosclerotic risk factors, clinical data, images and follow-up information were prospectively collected. Before stenting, they underwent BA wall HRMRI for visualization of BA plaque and the anatomical relationship between the BA plaque and the ostia of the adjacent branch arteries.
HRMRI protocols
The HRMRI protocol was approved by our institutional ethics committee. Written informed consent was obtained from all patients before each HRMRI examination. Using a 3 T MR scanner (Signa, TwinSpeed; GE Healthcare, Milwaukee, Wisconsin, USA) with an eight channel phased array head coil, we obtained the BA wall images. The following multicontrast sequences were used: (1) three-dimensional time of flight images, using repetition time/echo time (TR/TE)=21 ms/3.2 ms, field of view (FOV)=16 cm×16 cm, thickness=1 mm, matrix=256×256 and number of excitations (NEX)=1; (2) proton density weighted images (PDWI) and T2 weighted images (T2WI) of 12–14 slices; (3) and T1 weighted images (T1WI) of four slices precontrast and postcontrast, which included images at the slice of maximal lumen narrowing site. Parameters for PDWI and T2WI were as follows: fast spin echo (FSE), TR=3000 ms, TE=12.5 ms for PDWI and TE=62.3 ms for T2WI, FOV=16 cm×16 cm, thickness=2 mm, matrix=256×320, NEX=2 and echo train length (ETL)=10. T1WI were obtained by double inversion recovery FSE with the following parameters: TR/inversion time (TI)/TE=800 ms/650 ms/8.6 ms, FOV=16 cm×16 cm, thickness=2 mm, matrix=256×320 matrix, NEX=4 and ETL=12. Postcontrast T1WIs were acquired 5 min after gadolinium injection (0.1 mmol/kg gadopentetate dimeglumine, Magnevist; Bayer Schering Pharma, Berlin, Germany). The cross sectional voxel size was 0.6 mm×0.6 mm on time of flight and 0.6 mm×0.5 mm on T1WI, T2WI and PDWI. Fat suppression was used to reduce signal from surrounding fatty tissues. A zip 512 matrix was used to enhance spatial resolution.
Results
HRMRI images of the three patients provided essential information to guide the endovascular intervention.
Case No 1
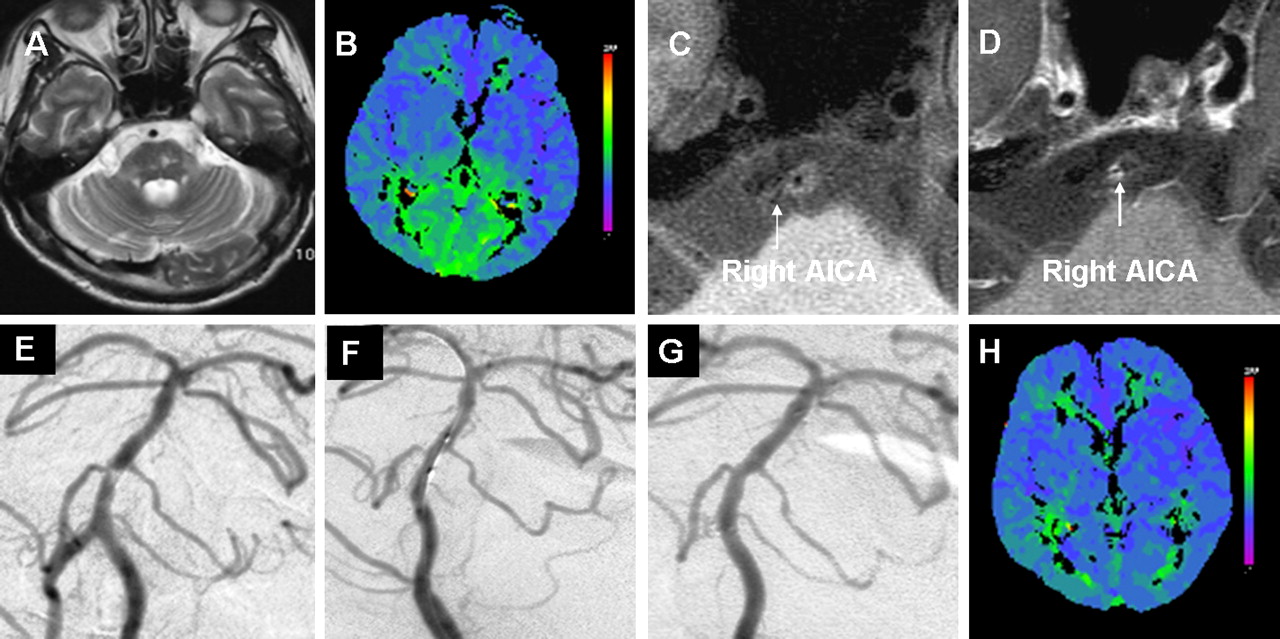
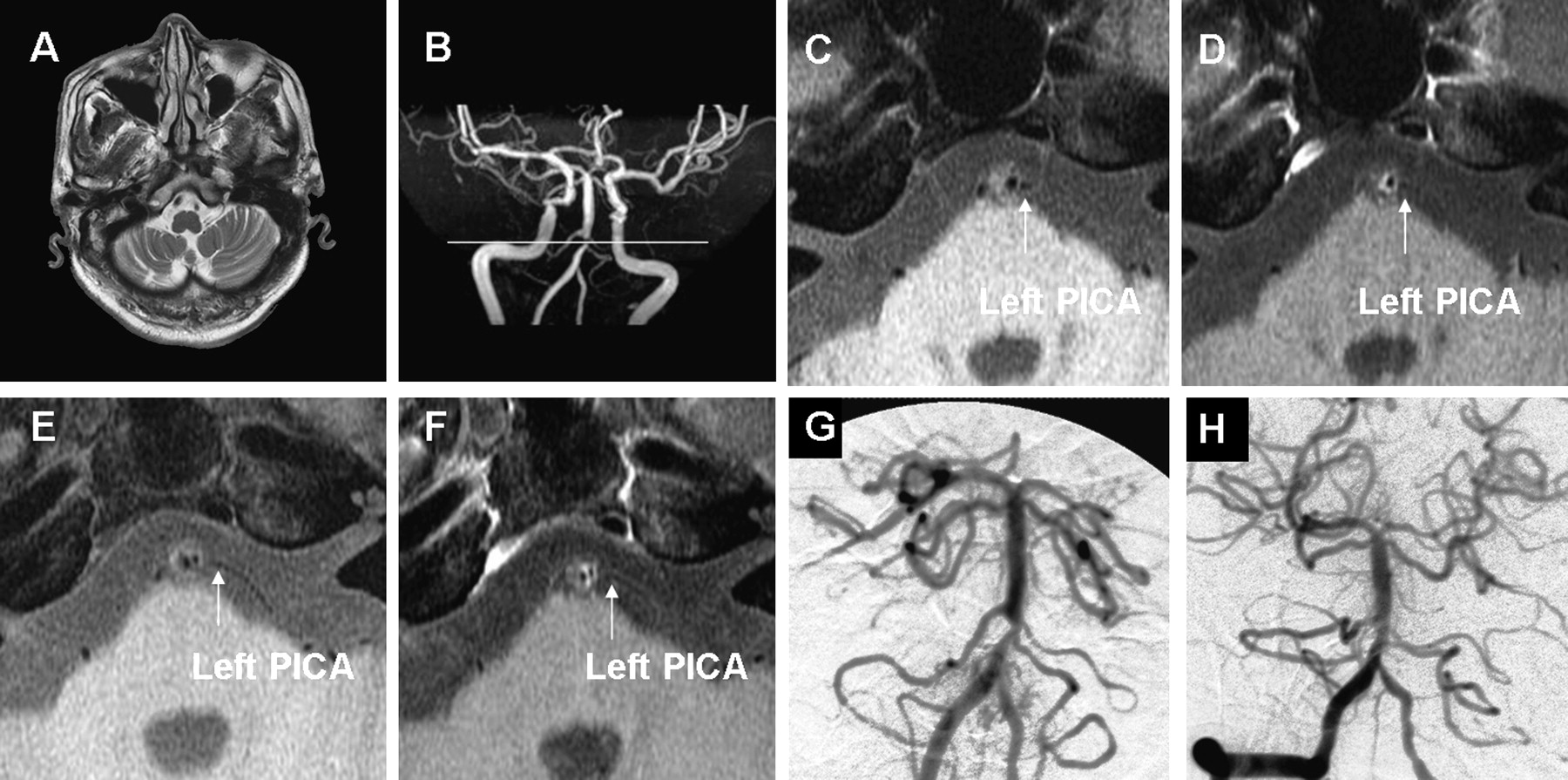
A 54-year-old man with a history of diabetes mellitus, hypertension, hyperlipidemia and hyperhomocysteinemia presented with recurrent transient attacks of dizziness for 2 months. Brain T2WI showed multiple small infarctions in the pons and cerebellum (figure 1A). CT perfusion demonstrated prolonged time to peak in the bilateral occipital lobes (figure 1B), suggesting flow limiting stenotic vertebrobasilar disease. HRMRI T1WI (figure 1C) and postcontrast T1WI (figure 1D) clearly revealed, at the slice of the narrowest site, an eccentric atherosclerotic plaque along the left arterial wall of the BA and identification of the right anterior inferior cerebellar artery (AICA). This finding suggested that the likelihood of the right AICA occlusion secondary to the stenting should be very low as it was located at the opposite wall of the BA plaque. Compared with that on T1WI (figure 1C), the slight enhancement by visual identification at the right AICA ostium was found on postcontrast T1WI (figure 1D). This suggested that neovasculature or inflammation may involve the right AICA ostium. Diagnostic angiogram showed a severe focal stenosis near the origin of the right AICA and proximal to the left AICA (figure 1E). Based on the HRMRI findings, the BA stenosis was treated with a 2.5 mm×9 mm Gateway balloon (Boston Scientific, Fremont, California, USA) (figure 1F) followed by placement of a 3 mm×15 mm Wingspan stent (Boston Scientific, Natick, Massachusetts, USA) without compromising either of the AICAs (figure 1G). Repeat CT perfusion showed normalization of the posterior circulation perfusion deficit (figure 1H). The patient was doing well without TIA or stroke on clopidogrel (for 1 year), aspirin, statin, oral hypoglycemic agent, and antihypertensive and antihomocysteine agents during the 34 month follow-up.

Brain T2 weighted image showed multiple small infarctions in the pons and cerebellum (A). CT perfusion demonstrated a prolonged time to peak in the posterior circulation (B), suggesting flow limiting stenotic vertebrobasilar disease. At the narrowest slice of the basilar artery (BA), an eccentric atherosclerotic plaque along the left BA wall was found on T1 weighted image (T1WI) (C), and the right anterior inferior cerebellar artery (AICA) ostium (arrow) with slight enhancement was visualized on postcontrast T1WI (D). Diagnostic angiogram showed the severe focal BA stenosis at the level of the origin of the right AICA and proximal to the left AICA (E). The BA stenosis underwent balloon angioplasty (F) and stenting without compromising either of the AICAs (G). Repeat CT perfusion showed normalization of the posterior circulation perfusion deficit (H).
Case No 2
A 59-year-old man with a history of hypertension, hyperlipidemia and hyperhomocysteinemia presented with recurrent transient attacks of dizziness for 8 months. Brain T2WI showed infarction in the cerebellum (figure 2A). CT perfusion demonstrated prolonged time to peak in the bilateral occipital lobes (images not shown), suggesting flow limiting stenotic vertebrobasilar disease. HRMRI T1WI (figure 2C) and postcontrast T1WI (figure 2D) clearly revealed, at the slice of the narrowest site, an eccentric atherosclerotic plaque along the right arterial wall of the BA. The left posterior inferior cerebellar artery (PICA) was visualized at the opposite of the atherosclerotic lesion on T1WI (figure 2C) and postcontrast T1WI (figure 2D). In proximal splice, the left PICA wound its way across the CSF on T1WI (figure 2E) and postcontrast T1WI (figure 2F). This suggested that the likelihood of the left PICA occlusion secondary to the stenting should be very low as it was located at the opposite wall of the BA plaque. Compared with that on T1WI (figure 2C,E), the slight enhancement by visual identification at the surface of the BA plaque and the left PICA ostium was found on postcontrast T1WI (figure 2D,F). This finding suggested that neovasculature or inflammation may involve the BA plaque and the left PICA ostium. Diagnostic angiogram showed a severe focal stenosis near the origin of the left PICA and proximal to the bilateral AICAs (figure 2G). Based on the HRMRI findings, the BA stenosis was treated by placement of a 2.5 mm×13 mm Apollo stent (MicroPort Medical, Shanghai, China) which was deployed by slow balloon inflation at 6 atm, without compromising the left PICA and the bilateral AICAs (figure 2H). Repeat CT perfusion showed normalization of the posterior circulation perfusion deficit (images not shown). The patient was doing well without TIA or stroke on clopidogrel, aspirin, statin, and antihypertensive and antihomocysteine agents during the 8 month follow-up.
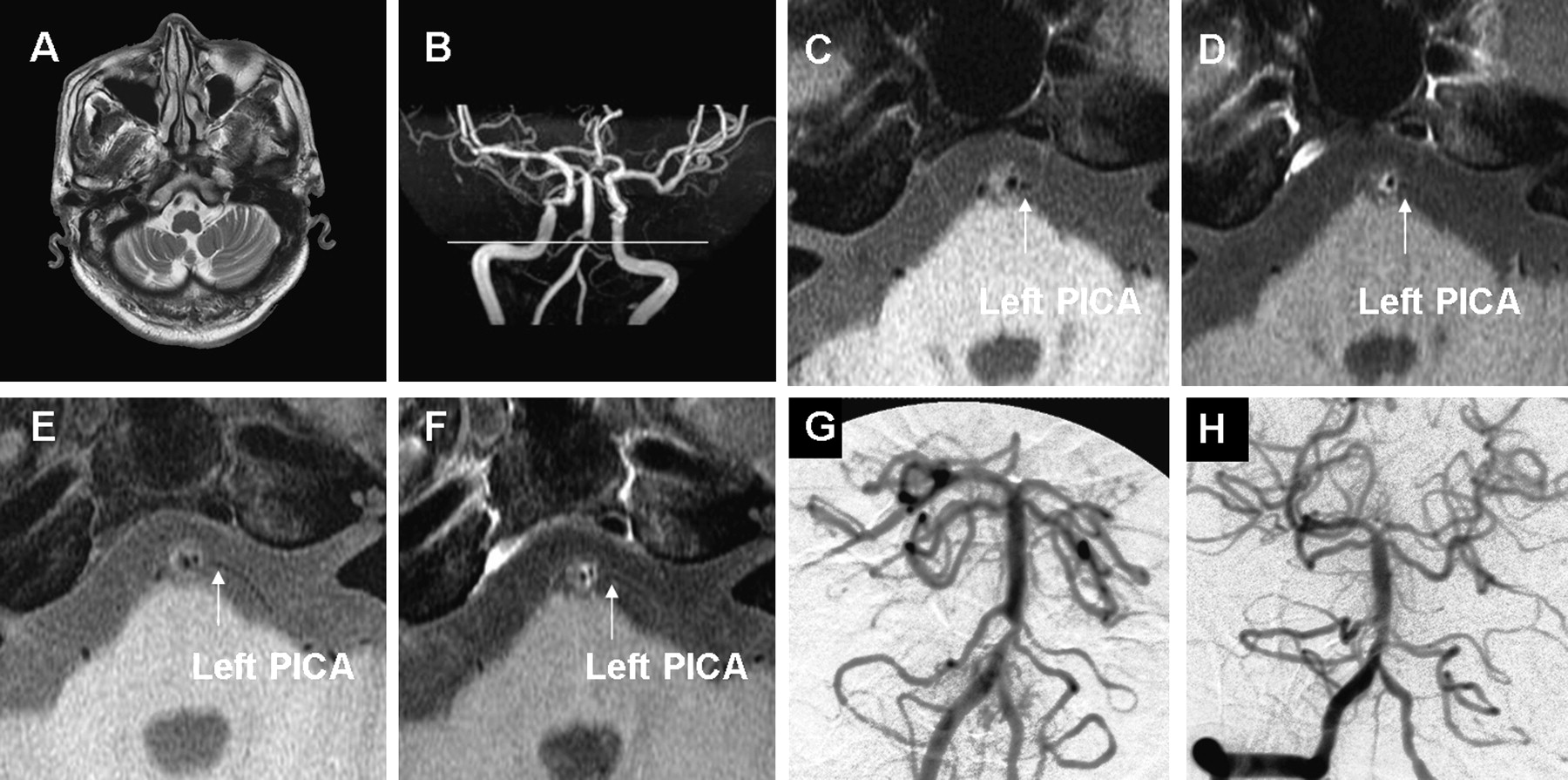
Brain T2 weighted image (T2WI) showed infarction in the cerebellum (A). MR angiography (MRA) showed high resolution MRI scan cover the narrowest site of basilar artery (BA) (B). At the narrowest slice of the BA, an eccentric atherosclerotic plaque along the right arterial wall of the BA was found on T1 weighted images (T1WI) (C) and postcontrast T1WI (D), and the left posterior inferior cerebellar artery (PICA) (arrow) was visualized at the opposite of the atherosclerotic lesion on T1WI (C) and postcontrast T1WI (D). In proximal splice, the left PICA wound its way across the CSF on T1WI (E) and postcontrast T1WI (F). The slight enhancement at the surface of the BA plaque and the left PICA ostium was found on postcontrast T1WI (D, F) The BA stenosis (G) was stented without compromising the left PICA and bilateral anterior inferior cerebellar arteries (H).
Case No 3
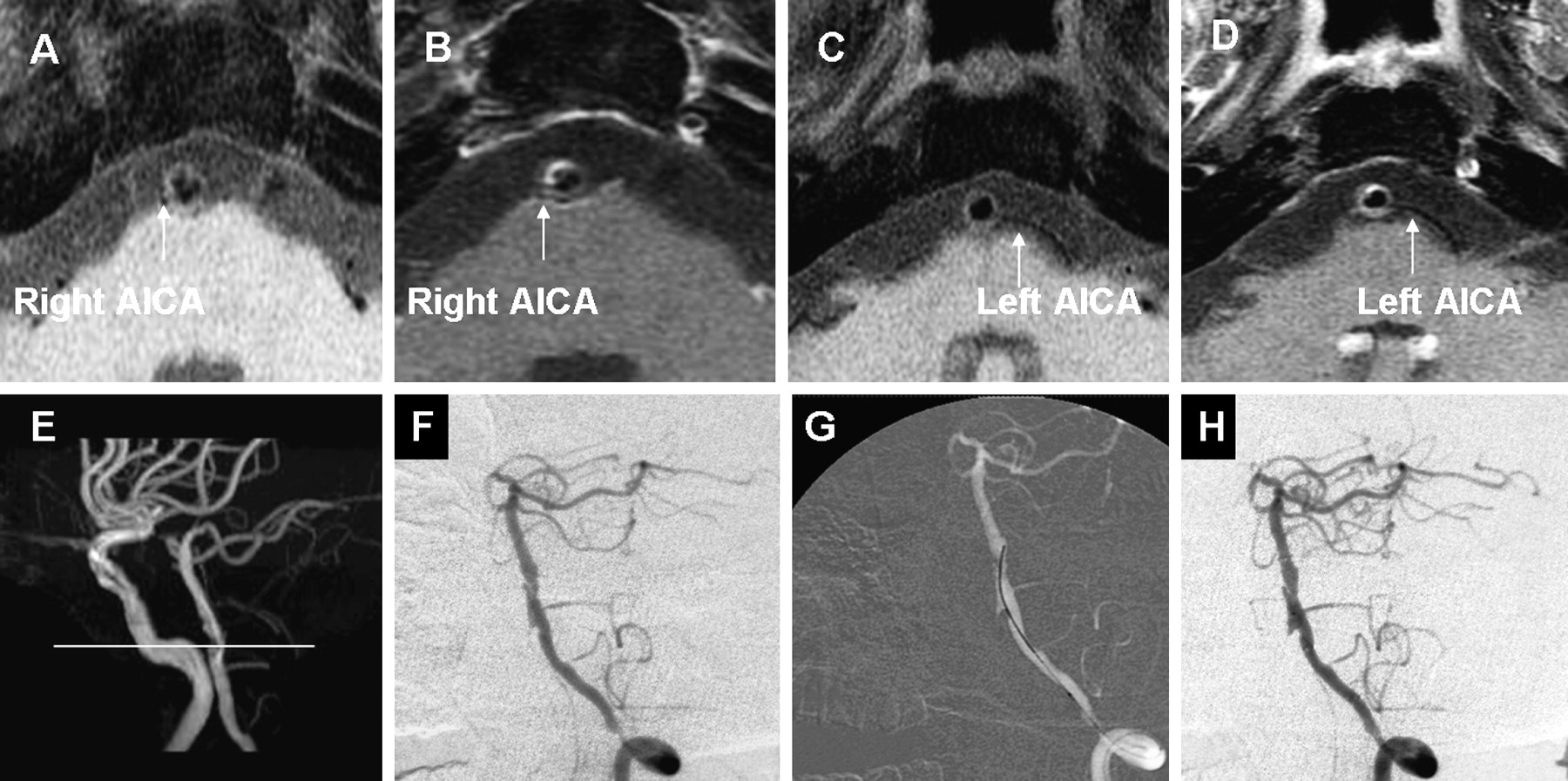
A 56-year-old man with a history of hypertension, hyperlipidemia and cigarette smoking presented with recurrent transient attacks of vertigo, diplopia and left hemiparesis for 2 months. The diagnostic angiogram showed BA stenosis at the level of the AICAs and focal stenosis at the intracranial segment (V4) of the left vertebral artery. CT perfusion scan revealed a significant perfusion deficit in the posterior circulation (images not shown). HRMRI T1WI (figure 3A) and postcontrast T1WI (figure 3B) showed, at the slice of the narrowest site of BA, an eccentric plaque at the anterior side of the BA wall protruding the BA lumen, separating it into two lumen similar with the dissection lesion. Combined with this HRMRI finding and diagnostic angiogram, the microwire should navigate through the ‘true lumen’ (posterior), avoiding through the ‘false lumen’ (anterior) which may cause the occurrence of iatrogenic dissection. The right AICA was visualized at the opposite side of the atherosclerotic lesion on T1WI (figure 3A) and postcontrast T1WI (figure 3B). In the proximal slice, the left AICA was free of atherosclerotic lesion on T1WI (figure 3C) and postcontrast T1WI (figure 3D). These findings suggested that the likelihood of the AICAs occlusion secondary to the stenting should be very low. Compared with that on T1WI (figure 3A), the slight enhancement by visual identification at the surface of the BA plaque and the right AICA ostium was found on postcontrast T1WI (figure 3B). This suggested that neovasculature or inflammation may involve BA plaque and the right AICA ostium. Both the BA and the distal vertebral artery lesions were stented with 4 mm×20 mm Wingspan stents following Gateway balloon (3 mm×15 mm) dilatation without compromising the bilateral AICAs (figure 3H). The patient was doing well without additional TIAs on clopidogrel, aspirin, statin and antihypertensive agent during the 3 month follow-up.

{kind=link}
{kind=link}
{kind=link}
At the narrowest slice of the basilar artery (BA), T1 weighted image (T1WI) (A) and postcontrast TIWI (B) showed an eccentric plaque protruding the BA lumen. The right anterior cerebellar artery (AICA) (arrow) was visualized at the opposite side of the atherosclerotic lesion on T1WI (A) and postcontrast T1WI (B). The slight enhancement at the surface of the BA plaque and the right AICA ostium was found on postcontrast T1WI (B). In the proximal slice, the left AICA (arrow) was free of atherosclerotic lesion on T1WI (C) and postcontrast T1WI (D). MR angiography showed a high resolution MRI scan cover the narrowest site of the BA (E). The diagnostic angiogram showed the BA plaque protruding the BA lumen similar to dissection, and left distal vertebral artery stenosis (not optimal projection) (F). The microwire navigated through the posterior lumen (G). Both the BA and vertebral artery stenosis were stented without compromising branch arteries (H).
Discussion
HRMRI has been increasingly used in the investigation of intracranial vascular pathologies.4–9 We report the use of HRMRI images to guide endovascular therapy of atherosclerotic BA disease. Our case studies are unique in the following features.
First, we used HRMRI to delineate the morphology of the atherosclerotic lesion and anatomical relation of the plaque with the ostia of the major branch arteries. Of note, angioplasty may result in ‘snow plowing’ or forceful displacement of atheromatous material into branch–vessel ostia.10 11 This phenomenon can occur in as many as 30% of patients with coronary atherosclerotic disease, resulting in branch–vessel occlusion at rates as high as 19%.12 The BA plaque HRMRI may help us to estimate the likelihood of occlusion of the branch artery or perforators by stenting and avoid unnecessary complications. When an atherosclerotic plaque is at the opposite of major side branches (such as AICA or PICA), the likelihood of branch arteries occlusion should be very low, as these branch vessels would not be influenced by the angioplasty ‘snow plowing’ effect. On the other hand, we should use a subsized balloon to pre-dilate BA stenosis with a low balloon inflation pressure, followed by placement of a self-expanding stent, or use a balloon stent with a low balloon inflation pressure when encountering a BA plaque with branch arteries.
Second, without delineation of the anatomical relationship between ‘the false and true lumen’ in case No 3 by combined HRMRI and angiogram findings, endovascular intervention would be associated with a higher risk of complications due to possible iatrogenic dissection by incorrect microwire advancement that may lead to arterial rupture or occlusion of multiple perforating arteries. This study shows that HRMRI may have potential application in the treatment of acute traumatic dissections by identification of true and false lumens.
Third, enhancement area of carotid plaque on postcontrast T1WI containing extensive neovasculature and accumulations of macrophages and T cells has been regarded as one of the most important characteristics of vulnerable plaques.13 14 Our study suggests that the enhancement on postcontrast T1WI may reflect the vulnerable nature of an active BA advanced atherosclerotic plaque.
Our study indicates that HRMRI of the BA wall is complementary to BA catheter angiogram. HRMRI may help minimize the risk of periprocedural complications of endovascular therapy.
Key messages
High resolution MR imaging (HRMRI) has been used to study intracranial atherosclerotic plaques. Three patients with symptomatic basilar artery (BA) atherosclerotic disease underwent BA wall HRMRI under a 3 T MR scanner before BA stenting. HRMRI clearly identified the eccentric atherosclerotic plaque at the opposite side of the adjacent branch arteries. The BA stenosis was stented without compromise of the adjacent branch arteries in the three patients. HRMRI may delineate the eccentric atherosclerotic plaque and the ostia of the major side branches of the BA and that may be helpful in guiding BA stenting with a reduced complication risk.
References
Footnotes
Funding The study was supported by the National Natural Science Foundation of China (81070925) and Medical Capital Development Fund of Beijing, China (2009-1937), to W-JJ; and PLA 11.5th Medical Foundation (06Q070) to XL.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Beijing Tiantan Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.