Article Text

Abstract
Background The effectiveness of mechanical thrombectomy (MT) in acute ischemic stroke due to large vessel occlusion is time-dependent. While only stroke centers with endovascular capabilities perform MT, many patients who had a stroke initially present to the closest primary stroke centers capable of administering earlier intravenous thrombolysis, and then require to be transferred to a comprehensive stroke center for MT.
Purpose To compare the outcomes of this care pathway (drip and ship (DS)) with that whereby patients are directly transferred to a comprehensive stroke center (mothership (MS)).
Methods We performed a systematic review and meta-analysis of published studies using several electronic databases to determine whether successful reperfusion (modified Thrombolysis In Cerebral Infarction ≥2b), functional independence at 90 days (modified Rankin Scale score ≤2), symptomatic intracranial hemorrhage, and 90-day mortality differed between those who underwent MT with the DS or the MS treatment pathway. Outcomes were meta-analyzed and the results expressed as adjusted relative risk (aRR) for the primary analysis and unadjusted relative risk (uRR) for secondary analysis.
Results Eight studies including 2068 patients were selected, including one study reporting results fully adjusted for baseline characteristics. Patients undergoing MS had better functional independence than those undergoing DS (uRR=0.87, 95% CI 0.81 to 0.93; aRR=0.87, 95% CI 0.77 to 0.98). No difference was found between the treatment pathways in successful reperfusion (uRR=1.05, 95% CI 0.95 to 1.15; aRR=1.00, 95% CI 0.92 to 1.10), symptomatic intracranial hemorrhage (uRR=1.37, 95% CI 0.91 to 2.06; aRR, 1.53, 95% CI 0.79 to 2.98), and 90-day mortality (uRR=1.00, 95% CI 0.84 to 1.19; aRR=1.21, 95% CI 0.89 to 1.64).
Conclusions Patients who had an acute ischemic stroke admitted directly to a comprehensive stroke center (MS patients) with endovascular capacities may have better 90-day outcomes than those receiving DS treatment. However, major limitations of current evidence (ie, retrospective studies and selection bias) suggest a need for adequately powered studies. Multicenter randomized controlled trials are expected to answer this question.
- stroke
- thrombectomy
- thrombolysis
Statistics from Altmetric.com
Introduction
Several randomized trials have demonstrated the clinical benefit of adding mechanical thrombectomy (MT) to standard medical therapy, compared with standard medical therapy alone, in the treatment of patients who have an acute ischemic stroke with large-vessel occlusion (LVO) of the anterior circulation.1 As a result, bridging IV thrombolysis therapy before MT has become the standard of care. Extensive data analyses showed a significant effect of the time period from stroke onset to reperfusion in determining the clinical outcome.2 3 MT is mainly performed in a comprehensive stroke center with on-site neuroendovascular capability. However, many patients with a stroke are initially transported to the nearest hospital where intravenous thrombolysis administration is available, necessitating a second transfer to a comprehensive stroke center. This may increase the overall time between onset of symptoms and reperfusion, possibly affecting the clinical outcome. The resulting dilemma created a debate about which is the optimal bridging therapy model.4 5 One treatment pathway is to transfer the patient initially to the nearest primary stroke center capable of initiating IV thrombolysis as early as possible (drip and ship (DS)), thereby lengthening the time to puncture and reperfusion.6 The second method is to transfer the patient directly to an endovascular-capable stroke center, where the bridging IV thrombolytic therapy is initiated, therefore reducing the time to puncture (mothership (MS)).
The optimal treatment pathway for these patients is not well established. Therefore, we aimed to conduct a systematic review and meta-analysis of the published data to determine whether the MS pathway provides better outcomes than DS in patients who have a stroke treated with MT.
Methods
This systematic review was reported according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines.7
Search strategy and selection criteria
We searched electronic databases (National Center for Biotechnology Information (NCBI)/National Library of Medicine (NLM), PubMed, and Ovid EMBASE) for English language studies published since January 2011, with the advent of MT, to October 2017. A combination of free-text and thesaurus terms for the concepts of ‘DS’, ‘MS’, ‘stroke’, and ‘thrombectomy’ was used to identify related literature. We also performed citation searches and searched reference lists of relevant studies. We included all type of studies published as original articles conducted in adult patients with acute ischemic stroke due to LVO of the anterior circulation. The interventions of interest were MT in a comprehensive stroke center preceded by IV thrombolysis in a primary stroke center (DS) or both MT and IV thrombolysis in a comprehensive stroke center (MS). Studies were not selected if they included patients who had a posterior circulation stroke, pediatric patients, primarily used the Merci device or intra-arterial pharmacotherapy, contained duplicate data on patients reported in other studies, had missing data in one of our outcomes of interest, or were cohorts with <20 patients. Conference abstracts were excluded. Our outcomes of interest were: functional independence defined as 90-day modified Rankin Scale (mRS) scores ≤2, successful reperfusion at the end of MT defined as modified Thrombolysis In Cerebral Infarction (mTICI) ≥2b, symptomatic intracerebral hemorrhage (sICH) and parenchymal hematoma (PH), and 90-day mortality (mRS score 6).
Seven studies were included after a full text review of studies identified through the screening process.8–14 We added another—our multicenter results study, for which a paper is under review as of May 2018, which involves several of the co-authors of the present manuscript,15 leading to a total of eight studies (figure 1 in the online-only supplementary data) involving a total of 2068 patients. A bibliography search of these studies did not disclose any additional relevant studies.
Supplementary file 1
Selection strategy, data extraction and quality assessment
Two reviewers (XA and BG) independently screened all titles/abstracts and performed full-text search within those publications for other potentially relevant citations. Disagreements were discussed and resolved through consensus or through recourse to a third reviewer (MI). Outcomes of interest for the DS and MS groups were independently extracted by two reviewers (MI and BG) for each study. The following variables where collected for each included study: study design, time period, endovascular device used, occlusion location, and thrombolysis rate. When available, age, National Institutes of Health Stroke Scale (NIHSS), and Alberta Stroke Programme Early CT Score (ASPECTS) at baseline were noted. We summarized the effect estimates with corresponding 95% CI for each study, using risk ratios (RR) reporting, both adjusted RR (aRR) and unadjusted RR (uRR), alongside the list of variables accounted for in the adjustment. In addition, time from symptom onset to IV thrombolysis, time from symptom onset to groin puncture, and time from symptom onset to successful reperfusion for the MS and DS patients in each study were collected. The data extracted were crosschecked and any disagreements were resolved by recourse to another reviewer (XA).
We assessed the quality of studies using checklists published by the National Institutes of Health relevant to each identified study design, according to the Newcastle Ottawa Scale (figure 2 in the online supplementary data)
Statistical analysis
We used random-effects meta-analyses to pool the estimates for each comparison. For our primary analysis, we used aRRs, and uRRs were used in our secondary analysis. Heterogeneity between studies was quantified with the I2 statistic (with ≥50% indicating substantial heterogeneity). We carried out random-effects meta-analyses for time from symptom onset to thrombolysis, time from symptom onset to puncture, and time from symptom onset to successful reperfusion. Some studies reported only median values together with range or IQR: we derived means and SD, which were needed for meta-analysis of continuous outcomes using statistical methods described by Luo et al 8 and Wan et al.9 All statistical analyses were performed using Stata version 15.1 (StataCorp, USA).
Results
Study characteristics
Study and population characteristics are summarized in table 1. Of these studies, one was a randomized controlled trial of stent-retriever thrombectomy, reporting outcomes by management method (MS or DS).10 One study reported outcome results after adjustment for baseline patients characteristics,16 and one after adjustment for time from symptoms onset to puncture.17 Times from symptom onset to thrombolysis, from symptom onset to groin puncture, and from symptom onset to successful reperfusion are listed in table 2. All patients included in these studies were treated with modern neurothrombectomy devices (stent retriever and/or contact aspiration). All studies defined functional independence as a 90-day mRS score ≤2. The definition of sICH was variable, and defined as one of the following: an increase in NIHSS score ≥4 points; any increase from baseline in NIHSS score11; parenchymal hematoma type 1 or 2 according to European Cooperative Acute Stroke Study (ECASS) criteria18 or sICH as defined by Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): local or remote PH type 2 associated with an increase of ≥4 points in the NIHSS score.19 The measure of successful reperfusion differed between studies, and included TICI ≥2, or mTICI ≥2b.
Study baseline characteristics
Mean time metrics
Time metrics
Based on available data from included studies, patients following the MS pathway had shorter time values than those following the DS pathway, including symptoms onset to thrombolysis (mean difference=16.85 min, 95% CI −21.83 to 11.86) (figure 3 in the online-only supplementary data), symptoms onset to puncture (mean difference=83.05 min, 95% CI –89.09 to 77.01) (figure 4 in the online-only supplementary data), and symptoms onset to successful reperfusion (mean difference=94.33 min, 95% CI –100.42 to 88.24) (figure 5 in the online-only supplementary data).
Clinical outcomes
Adjusted analysis
Based on the one available study,16 patients undergoing MS had better functional outcomes than those undergoing DS (aRR=0.87, 95% CI 0.77 to 0.98). The 90-day mortality was similar (aRR=1.21, 95% CI 0.89 to 1.64). No significant difference was seen for sICH (aRR=1.53, 95% CI 0.79 to 2.98).
Unadjusted analysis
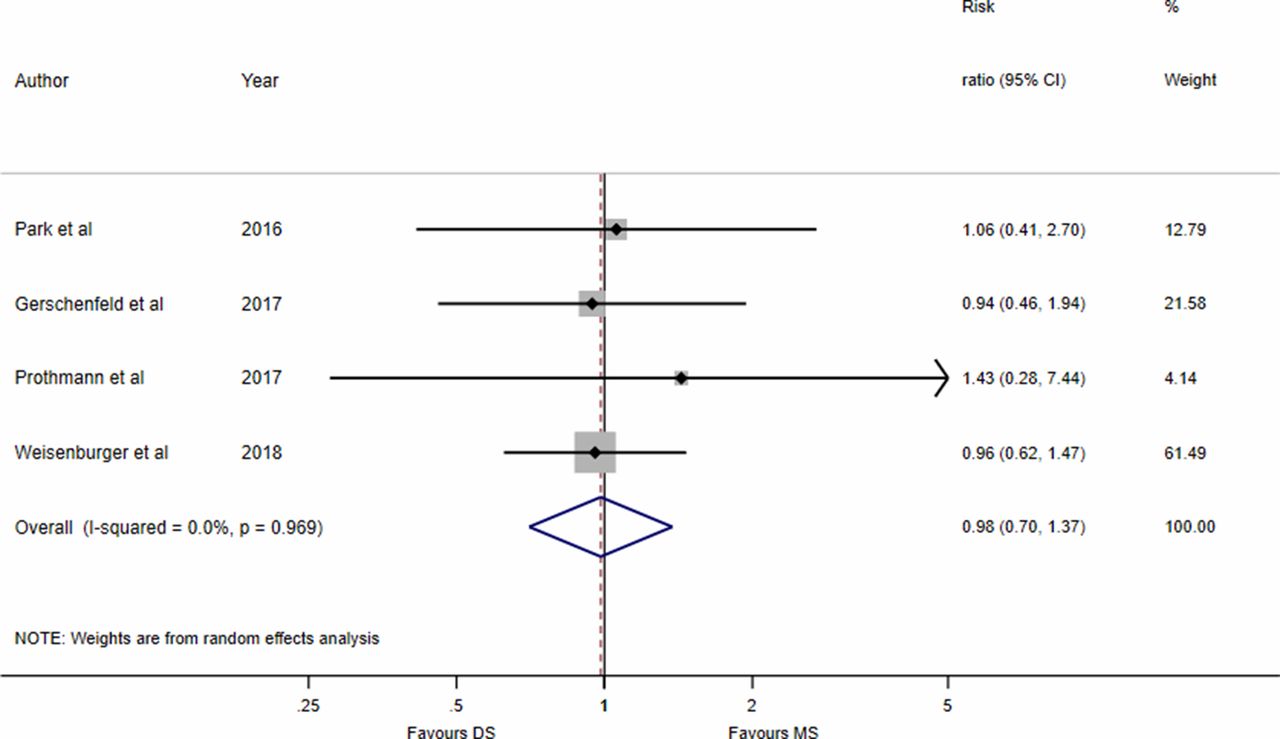
Based on eight studies, patients undergoing MS had better functional outcomes than those undergoing DS (uRR=0.87, 95% CI 0.81 to 0.93, I2=0.0%) (figure 1). Similar 90-day mortality was found in the MS and DS groups (uRR=1.00, 95% CI 0.84 to 1.19, I2=0.0%) (figure 2). I 2 statistics did not show significant heterogeneity for both outcomes. There was no significant difference in the rates of sICH (uRR=1.37, 95% CI 0.91 to 2.06, I2=0.0%) and PH (uRR=0.99, 95% CI 0.7 to 1.37, I2=0.0%) (figure 3), with no heterogeneity across studies.

Meta-analyses of studies comparing (A) successful reperfusion (modified Thrombolysis In Cerebral Infarction (mTICI) or TICI ≥2b, and (B) good functional outcomes (90-day modified Rankin Scale score ≤2, in patients who underwent mechanical thrombectomy in the mothership (MS) and drip and ship (DS) models.
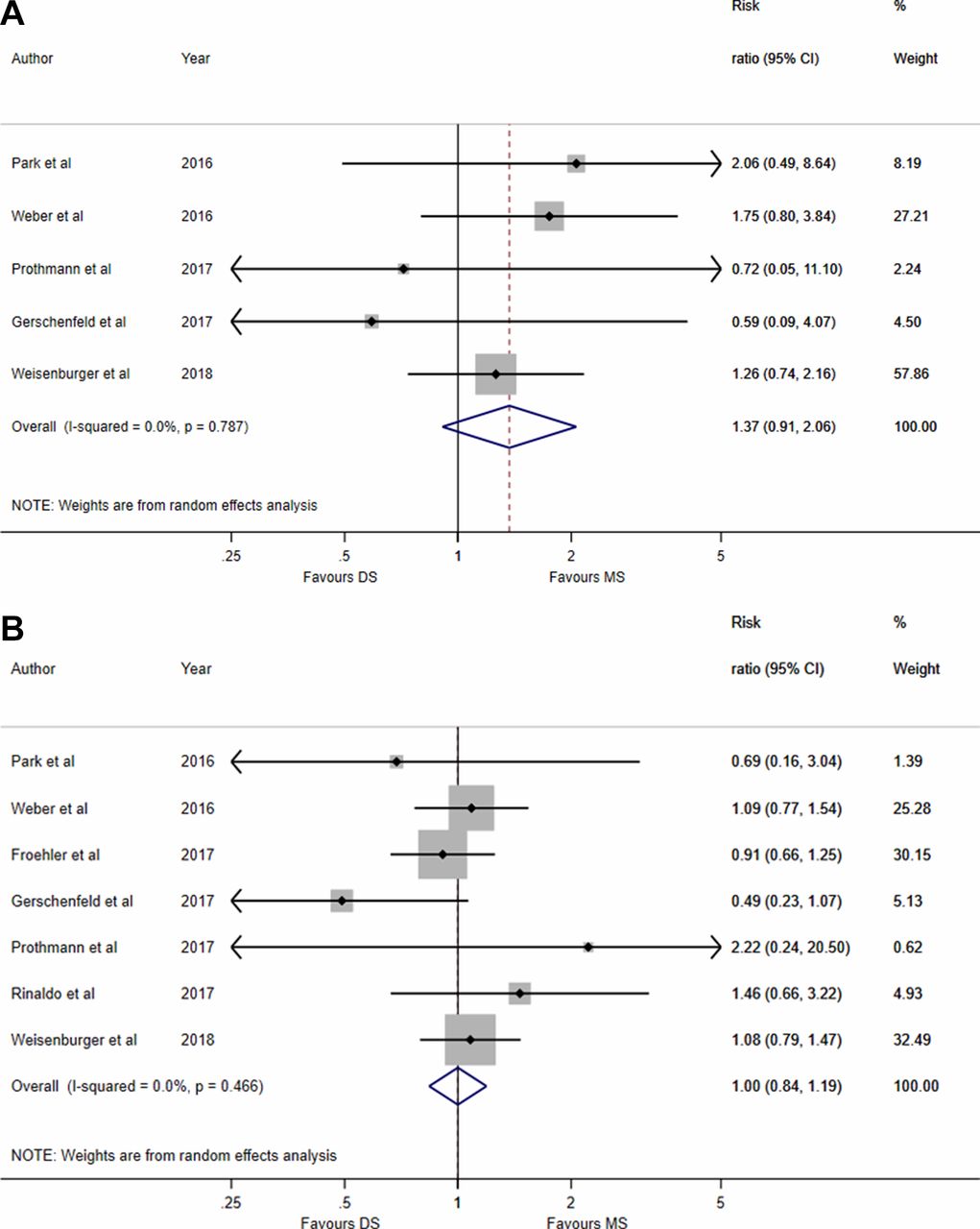
Meta-analyses of studies comparing (A) rates of symptomatic intracranial hemorrhage within 24 hours, and (B) 90-day mortality (modified Rankin Scale score 6) in patients who underwent mechanical thrombectomy in the mothership (MS) and drip and ship (DS) models.

{kind=link}
{kind=link}
{kind=link}
Meta-analyses of studies comparing rates of parenchymal hematoma within 24 hours in patients who underwent mechanical thrombectomy in the mothership (MS) and drip and ship (DS) models. CI indicates CI.
Procedural outcomes
There was no difference between MS and DS management in the successful reperfusion rates (aRR=1.00, 95% CI 0.92 to 1.10; uRR=1.05, 95% CI 0.95 to 1.15, I2=81.8%). A wide heterogeneity between studies was observed.
Discussion
This meta-analysis aimed to achieve a better understanding of whether administration of IV thrombolysis in comprehensive stroke centers, while avoiding early pretreatment in primary stroke centers, provided additional benefits to the prognosis of patients treated with MT, as this theoretically shortens time-to-puncture but delays IV thrombolysis. Our results show two major findings1: patients undergoing MS have a higher probability of achieving 90-day functional independence than those treated in DS,2 MS seems safe since the rates of sICH and PH, and 90-day mortality were similar to those seen in patients following the DS pathway. Arterial puncture was performed 83 min earlier in MS, and thrombolysis was surprisingly administered 16 min earlier also in MS.
Extensive data have shown that higher rates of successful reperfusion and shorter time between symptom onset and reperfusion are predictors of good outcomes after MT.3 20–23 In our meta-analysis, we found no significant differences in rates of successful reperfusion between the two treatment models. However, the heterogeneity between included studies was important, limiting the accuracy of our results. The majority of studies showed shorter time of onset-to-thrombolysis in the DS model, while there were shorter onset-to-puncture and onset-to-reperfusion times in the MS model. These delays could be explained by the better management and in-hospital workflow and/or by the fact that patients included in the MS group were closer to the comprehensive stroke center than DS patients were to the primary stroke center. The significantly better clinical outcomes we found in patients undergoing MT with the MS model is probably accounted for by the shorter time-to-reperfusion, a proven important predictor of good outcome.3 21
The observed difference between treatment models could be explained by several factors. IV thrombolysis without MT logically achieves low recanalization rates in patients with LVO.24 However, several studies have highlighted the role of prior IV thrombolysis in facilitating later recanalization with MT, both in achieving higher rates of successful reperfusion and requiring fewer passes during MT.25 26 However, these studies did not correlate their findings with time of symptom onset to thrombolysis, and compared results only for patients undergoing bridging therapy before MT with patients treated only with MT. Therefore, the added value of earlier IV thrombolysis achieved in the DS model might have compensated, at least in part, for the longer onset-to-reperfusion time. Another explanation for the small differences might be the heterogeneity of baseline characteristics between the two different models in the analyzed studies. Baseline characteristics were heterogeneous in two of the eight studies for NIHSS and ASPECT scores,15 17 while data concerning ASPECTS were not available in four other studies11–14. No correlation was found in a meta-regression analysis performed to account for these differences in baseline data between the two groups.
Our analysis showed a trend toward a higher sICH rate in the MS pathway, without statistical significance. The 90-day mortality was identical between the two groups reporting the potential safety of the MS approach. Randomized trials comparing direct MT with bridging therapy, such as the ongoing SWIFT-DIRECT trial, will determine the benefit of prior IV thrombolysis in patients with a stroke treated with MT and directly admitted to comprehensive stroke centers.
The continuing argument about the benefits of DS or MS, especially in geographical areas where comprehensive neuroendovascular centers are few and far apart, should be resolved by randomized trials. Such data should be incorporated in the implementation of reliable conditional probability models, which will be tailored for each geographical area and therefore able to incorporate geolocation mapping for the transportation of patients with an ischemic stroke for MT. The main limitation of our analysis is that patients were admitted to the nearest center whatever the endovascular capacities of that center. Our findings highlight that the workflow was better in comprehensive stroke centers than in primary stroke centers. We hope that some answers to the open questions presented will be provided by the ongoing RACECAT trial (NCT02795962), comparing MS and DS.
Conclusions
This meta-analysis reported that patients undergoing IV thrombolysis and MT in a comprehensive stroke centers, without going first to a primary stroke center (MS) had better 90-day functional outcomes than patients undergoing IV thrombolysis in primary stroke centers first (DS); there were no concerns about safety. These results do not correlate with the current guidelines, which recommend rapid transport of patients with a stroke to the nearest primary stroke center capable of providing IV thrombolytic therapy, even if they are being considered for MT.
References
Footnotes
MI and XA contributed equally.
Contributors MI: substantial contribution to conception of the work, acquisition, analysis, and interpretation of data. XA: substantial contribution to the acquisition, analysis, and interpretation of data. NT, FZ, US-G, MP, RB, MM, SB, RA, ES, GM, LH, J-CL, SR, BL: revision of the work for important intellectual content. CB: revision of the work for important intellectual content; substantial contribution to the conception of the work, acquisition, analysis, and interpretation of data. BG: revision of the work for important intellectual content; final approval of the version published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement N/A.