Article Text

Abstract
Background and aim Intracranial vertebrobasilar artery (VBA) stenosis portends a stroke and death rate of 8.5–22.8% annually despite medical therapy. Stenting has emerged as a treatment option but also carries substantial risk. Awake stenting under local anesthesia to minimize major procedural complication was investigated.
Methods Between January 2007 and December 2008, 43 of 46 consecutive patients with severe symptomatic intracranial VBA stenosis underwent elective angioplasty assisted with self-expanding Wingspan stent under local anesthesia at our institute. All data were collected prospectively.
Results All 43 patients tolerated the stenting procedure under local anesthesia well. Forty-two patients (97.7%) were stented successfully. Within 30 days, there were three periprocedural strokes, including thromboembolic infarct, pontine perforator infarct and intracranial hemorrhage, without fatality. In addition, five patients had intraoperative brainstem transient ischemic attacks (TIAs) seconds after the deployment of the stent delivery system across the tortuous VBA. The symptoms and signs included impaired consciousness (n=5), dysarthria (n=3), convulsion (n=2), conjugate horizontal gaze palsy (n=2), nystagmus (n=2) and pinpoint pupils (n=1). There was angiographic evidence of VBA straightening without thromboembolism. The TIAs resolved within minutes of prompt removal of the delivery catheter.
Conclusions VBA stenting under local anesthesia is feasible with a 7% periprocedural stroke risk. Awake stenting allows timely detection of intraoperative TIAs. The mechanism of intraoperative TIA appears to be stent delivery system induced VBA straightening and distortion of its vascular tree. A devastating stroke may ensue if the TIA is not detected and distortion of VBA perforators is not reversed promptly.
- Atherosclerosis
- stenosis
- stroke
- complication
- stent
Statistics from Altmetric.com
Severe atherosclerotic intracranial vertebrobasilar artery (VBA) stenosis portends a stroke and death rate of 8.5–22.8% per year despite medical therapy.1–4 Stenting has emerged as a therapeutic option for stroke prevention but also carries a substantial risk (6.7–45%) of procedure related cerebrovascular events, including thromboembolic stroke, perforator stroke, intracranial hemorrhage (ICH) or death.5–10 A recent systematic review showed that periprocedural complications were significantly higher in the posterior circulation than in the anterior circulation (12.1% vs 6.6%).11 Most investigators perform intracranial stenting under general anesthesia,5 8 10 12 which may mask procedure related neurological changes during stenting and contribute to higher risk of devastating complications. Awake stenting under local anesthesia allows timely detection of acute neurological changes and may reduce the risk of major procedural complication. The objective of this study was to investigate VBA stenting under local anesthesia to minimize major procedural complications.
Methods
Subjects
Between January 2007 and December 2008, 46 consecutive patients with symptomatic severe atherosclerotic stenosis (≥70%) of intracranial VBA underwent elective angioplasty with the Wingspan stent (Boston Scientific, Fremont, California, USA) at Beijing Tiantan Hospital. Awake stenting under local anesthesia was performed in 43 patients, including 23 with vertebral artery (VA) stenosis (22 with VA stenosis and one with stenoses at VA and communicating segment of the right internal carotid artery) and 20 with basilar artery (BA) stenosis (18 with BA stenosis, one with stenoses at BA and lacerum segment of the left internal carotid artery and one with stenoses at BA and the left middle cerebral artery). Stenting under general anesthesia was performed in the remaining three patients (two with VA stenosis and one with BA stenosis). Patient demographics, clinical data, images and follow-up information were prospectively collected. The study was approved by the institutional ethics committee of our hospital. Written informed consent was obtained before each stenting procedure. Patients were given aspirin 300 mg plus clopidogrel 75 mg daily for 3 days or more before the operation, and for at least 1 month after stenting. Then, either aspirin or clopidogrel was continued for life. Modifiable atherosclerotic risk factors were also managed per guidelines.
Stenting procedure
Awake stenting was performed under local anesthesia with 1% lidocaine by experienced interventional neuroradiologists. Intravenous infusion of nimodipine (0.6 mg/h) was started 2 h before the procedure to prevent intraoperative vasospasm. A bolus of 3000 units of heparin was given intravenously at the beginning of the procedure, followed by infusion at a rate of 800 units/h. A 6 French gauge guiding catheter was advanced to the distal V2 segment of VA through a 6 French gauge femoral sheath. An assembly of microcatheter and 0.014 inch, 300 cm microwire was used in all patients. Under roadmap guidance, the assembly was carefully steered through the target lesion and placed into the P3 or P4 segment of the posterior cerebral artery. After the microcatheter was removed, the Gateway balloon (Boston Scientific), which was sized to approximate the length of the lesion, with its diameter at 80% of the adjacent non-diseased segment, was advanced over the microwire, centered across the lesion and inflated slowly at 6–8 atmospheric pressure with a 50% mixture of iodinated contrast and saline. Conventional angiography was then repeated, followed by advancement of the Wingspan stent delivery system over the microwire across the target lesion, deployment of the stent and then removal of the delivery catheter. The length of the stent was chosen to cover the stenosis in addition to up to 3 mm proximally and distally. The stent diameter was sized to exceed the diameter of the normal parent vessel by 0.5–1.0 mm. Technical success was defined as target lesion completely covered by stent, resulting in a ≤50% residual stenosis with good anterograde blood flow.
Evaluation of complications
Blood pressure was tightly controlled (systolic blood pressure 100–120 mm Hg) with infusion of nimodipine or urapidil hydrochloride to prevent hyperperfusion syndrome immediately after stent placement. Brain CT was performed instantly to exclude ICH. Brain MRI was performed if the patient had a new ischemic event and had no contraindication for MRI.
Neurologic events during stenting and within 30 days of the procedure were assessed by stroke neurologists. Probable cause of the neurological event was determined with consensus in a multidisciplinary meeting attended by stroke neurologists, neuroradiologists and interventional neuroradiologists.
Results
All 43 patients tolerated the stenting procedure under local anesthesia well, including three patients who also underwent stenting of stenosis in the anterior circulation at the same session, without the use of sedatives or other medications. The technical success rate of stent placement was 97.7% (42/43). Stent placement failure occurred in one of the initial five patients. The Wingspan stent system could not achieve the site distal to the patient's BA stenosis following balloon predilatation. Table 1 summarizes the patient characteristics and angiographic outcome after stenting.
Patient characteristics and angiographic outcome after stenting in 43 patients
There was no periprocedural mortality but there were three (7.0%) major periprocedural complications. One was a thromboembolic infarct in the right temporo-occipital area after BA stenting which occurred in the patient with failed Wingspan stent placement. The cause was acute BA occlusion from severe dissection distal to the lesion site, presumably due to the intima of the tortuous BA injured by the gap left between the tip and the outer sheath of the stent system while it was advanced forward. The BA occlusion was successfully treated with two balloon expandable stents following intra-arterial thrombolysis. The second was a left pontine perforator infarct following BA stenting, presumably due to perforator occlusion. The remaining one was parenchymal and subarachnoid hemorrhages during VA stenting, resulting from perforation of a posterior cerebral artery branch by the tip of the microwire. All of the three patients recovered with mild to moderate disability (n=2) or a baseline National Institutes of Health Stroke Scale 2 (n=1) at day 30.
Interestingly, severe brainstem transient ischemic attacks (TIAs) were observed intraoperatively in five patients (11.6%), including three patients with BA stenosis and two with VA stenosis adjacent to the vertebrobasilar junction (table 2). The attacks occurred within seconds of the deployment of the stent delivery system into tortuous intracranial VBA with its distal end in BA (figure 1). The symptoms and signs of the TIAs included sudden loss of consciousness and clonic movement of bilateral extremities (n=1), decreased levels of consciousness and dysarthria, with or without hemiparesis (n=2), decreased levels of consciousness, nystagmus and conjugate horizontal gaze palsy with pinpoint pupils (n=1) or convulsion (n=1). There was no angiographic evidence of thromboembolism in the VBA and its main branches. However, stent delivery system induced straightening of the target vessel was noticed on angiography (figure 1). The TIAs were most severe within seconds or minutes following onset. They started to alleviate soon after prompt withdrawal of the stent delivery system, and completely resolved within 5–30 min. All of the five patients were doing well without neurological sequalae. Follow-up CT and MRI showed no new infarction.
Clinical data for the five patients who had brainstem TIAs during awake stenting

Case No 3 (table 2) had a basilar artery stenosis of 80% (A). Balloon angioplasty reduced the stenosis to 20% (B). A transient ischemic attack occurred soon after the stent delivery system was placed across the target lesion in the basilar artery. The delivery catheter was noted to induce straightening of the basilar artery (C). After removal of the stent delivery system, symptoms and signs resolved within 8 min (D).
Discussion
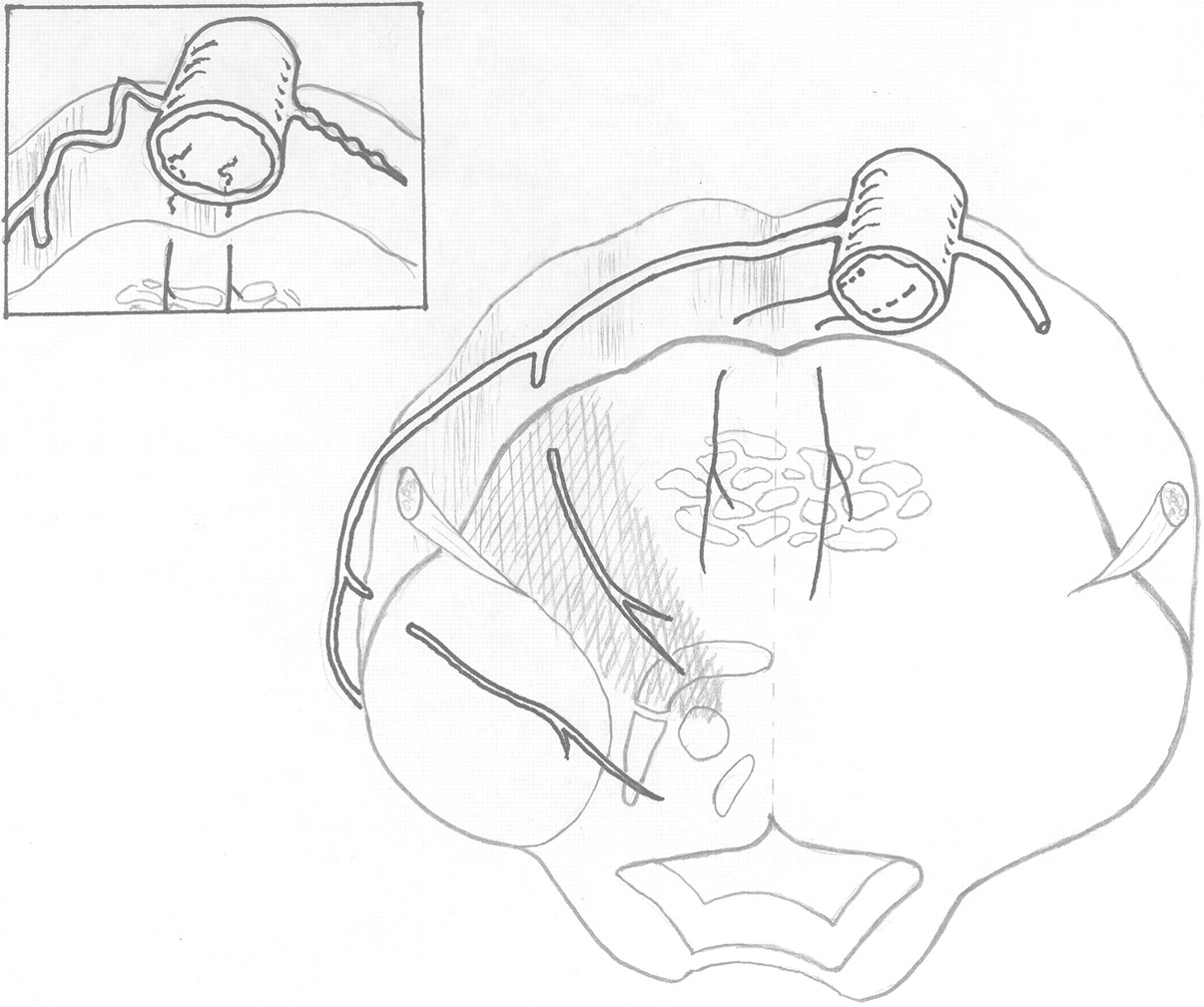
In this single center study, we demonstrated that stenting of severe intracranial VBA stenosis under local anesthesia was associated with a low risk of periprocedural stroke. We also showed that awake stenting allows detection of intraoperative TIAs and reversal of potentially devastating brainstem ischemia. The intraoperative brainstem TIA is a previously unrecognized complication because it can only be detected with neuromonitoring under local anesthesia. The acute impairment of consciousness and associated brainstem signs could not be explained by involvement of any single perforator. They are most likely the result of bilateral brainstem ischemia.13 14 The timings of the events and prompt resolution of the symptoms following the removal of the stent delivery catheter also ruled out the displacement of atheroma by the stent into the ostia of small perforating vessels (snowplowing) or stent struts covering the perforator's ostia.15 There was angiographic evidence of VBA straightening without thromboembolism in the artery and its main branches. We therefore propose the mechanism of the TIAs as illustrated in figure 2. Placement of the Wingspan stent delivery system across the target lesion induces straightening of the tortuous VBA, leading to kinking and overstretching of the perforators. Such acute distortion of the VBA vascular tree may impair perforator blood flow, resulting in bilateral brainstem ischemia. The deformed VBA and its perforators normalize if the stent delivery catheter is withdrawn immediately. A devastating stroke may ensue if the TIA is not detected and distortion of the VBA perforators is not reversed promptly.
{kind=link}
{kind=link}
The right lower sketch shows the anatomy of the basilar artery vascular tree before placement of the stent delivery system in the basilar artery. The left upper sketch shows kinking and overstretching of multiple perforators due to stent delivery system induced straightening of the basilar artery.
The Wingspan stent system has been well studied in intracranial stenosis.12 16 17 The existing data indicated high rates of technical success and reasonable levels of periprocedural adverse events. However, the procedural risk from intracranial VBA stenting is a major concern, with a mortality rate as high as 10.7%.16
The rate of major procedural complications in our case series was lower and less severe than that reported previously.5 8 10 16 One of the most reasonable explanations is that we performed awake stenting under local anesthesia that was able to avoid potentially devastating stroke from stent delivery system induced distortion or rupture of the VBA vascular tree.
Our findings have significant clinical implications. (1) Acute neurological changes are unlikely to be detected intraoperatively if the stenting is performed under general anesthesia. (2) Stent delivery system induced distortion of the VBA vascular tree may be a potential risk of devastating brainstem ischemia or vessel rupture. (3) Tortuous BA or angled lesion might be a predictor of procedural complications. (4) Improvement in the flexibility of the Wingspan stent system may be beneficial. (5) It is essential to advance the stent delivery catheter and to deploy the stent very gently without delay at the target lesion, regardless of the type of anesthesia (general or local) or stent (self-expanding or balloon expandable).
There were several limitations in this study. (1) The clinical features of brainstem ischemia described above might be incomplete, as it was not possible to do a full neurological examination intraoperatively. (2) There was no direct angiographic evidence of VBA perforator distortion due to limited spatial resolution of the digital subtraction angiography. Additional studies are necessary to prove that prolonged or significant distortion of the VBA vascular tree would lead to irreversible impairment of blood flow or rupture of the vessels, resulting in devastating ischemia or hemorrhage. (3) This study has not reported on the long term outcome of the patients as we wished to describe the brainstem TIA from stenting in detail. We will report on the long term outcome of our patients following Wingspan stenting in the future.
In summary, VBA stenting under local anesthesia is feasible with a 7% periprocedural stroke risk. Awake stenting allows timely detection of intraoperative TIAs. The mechanism of intraoperative TIA appears to be stent delivery system induced VBA straightening and distortion of its vascular tree. A devastating stroke may ensue if the TIA is not detected and distortion of the VBA perforators is not reversed promptly.
Key message
Most investigators perform intracranial stenting under general anesthesia, which may mask procedure related neurological changes during stenting. Awake stenting under local anesthesia allows timely detection of acute neurological changes and may reduce the risk of major procedural complications. In this study, severe brainstem TIA, a previously unrecognized complication, was observed in five (11.6%) of 43 patients with VBA stenosis, in addition to procedure related stroke in three patients (7.0%). The TIA mechanism appears to be stent delivery system induced VBA straightening and distortion of its vascular tree. A devastating stroke may ensue if the TIA is not detected and distortion of the VBA perforators is not reversed promptly.
Acknowledgments
We thank Dr Marc Chimowitz, Medical University of South Carolina, for excellent discussions and suggestions.
References
Footnotes
Funding This study was supported by the Ministry of Health of The People's Republic of China (2004BA714B-7) (20080527) to W-JJ.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Beijing Tiantan Hospital.
Provenance and peer review Commissioned; not externally peer reviewed.