Article Text

Abstract
Endosaccular flow disruption is an innovative method of treating wide-necked complex aneurysms. Currently four types of devices have obtained the CE mark for use within Europe. These are the Woven EndoBridge device (WEB), the Luna Aneurysm Embolization System, the Medina Embolic Device (Medtronic), and the Contour Neurovascular System. The aim of this article is to provide an overview of these devices and to summarize the evidence in the literature pertaining to the treatment of intracranial aneurysms with them.
- flow disruption
- WEB
- MED
- LUNA AES
- contour
Statistics from Altmetric.com
Introduction
The endovascular treatment of intracranial aneurysms has substantially progressed since the use of the Guglielmi detachable coils system in the 1990s.1 The International Subarachnoid Aneurysm Trial2 3 and the California Unruptured Aneurysm Study4 5 have shown better endovascular outcomes for patients than surgical clipping for both ruptured and unruptured aneurysms. In the wake of these findings, strategies to expand the numbers of aneurysms amenable to endovascular treatment have developed rapidly. Effective treatment of more complex aneurysms with coils alone is often not technically possible. This has led to the use of balloon remodeling and stent-assisted coiling techniques, which allowed the treatment of wide-necked and complex aneurysms and provided better occlusion and lower recurrence rates.6 Endoluminal flow diverting stents thus provide a more definitive solution for sidewall aneurysms. These devices create an initial flow diversion effect which induces aneurysm thrombosis, followed by definitive parent artery remodeling and subsequent resorption of intra-aneurysmal thrombus which, in a high percentage of patients with appropriately selected aneurysms, results in durable and complete occlusion.7 8
Although intraluminal flow diverting stents have provided an excellent option for the treatment of unruptured side wall aneurysms, they can be ineffective for the significant percentage of aneurysms (35–50%) which arise from bifurcations9 and they are not indicated for the treatment of ruptured aneurysms.
Endosaccular flow disrupting devices have been recently developed in an attempt to create intra-aneurysmal flow disruption and to create a definitive remodeling at the aneurysm–parent artery interface, similar to that seen with intraluminal flow diverters. Structurally, these devices are constructed of a tightly braided wire mesh that is subsequently configured into a roughly spherical or hemispherical shape. The entire device is designed to be deployed within the aneurysm, with the interstices of the mesh covering the aneurysm neck and reconstructing the aneurysm–parent artery interface. The implant disrupts the blood flow entering and exiting the aneurysm sac, resulting in stasis and thrombosis. The mesh across the aneurysm neck can support neoendothelial overgrowth and subsequently a durable and definitive aneurysm occlusion. These devices are optimally designed for the treatment of wide-necked aneurysms.10 Moreover, since the entire implant is intra-aneurysmal and requires no concomitant antiplatelet prophylaxis, this class of devices also represents an attractive solution for treating ruptured aneurysms.
Several endosaccular devices have been developed. These are the Woven EndoBridge (WEB) device (Microvention, Aliso Viejo, California, USA), the Luna Aneurysm Embolization System (LUNA AES; Medtronic, Irvine, California, USA), the Medina Embolic Device (MED; Medtronic), and the Contour Neurovascular System (Cerus Endovascular, Fremont, California, USA). The only FDA approved device in this group is the WEB, which was approved through the PMA pathway last year. This article will provide a review of the existing clinical experience with these four devices.
Device design
Woven EndoBridge (WEB)
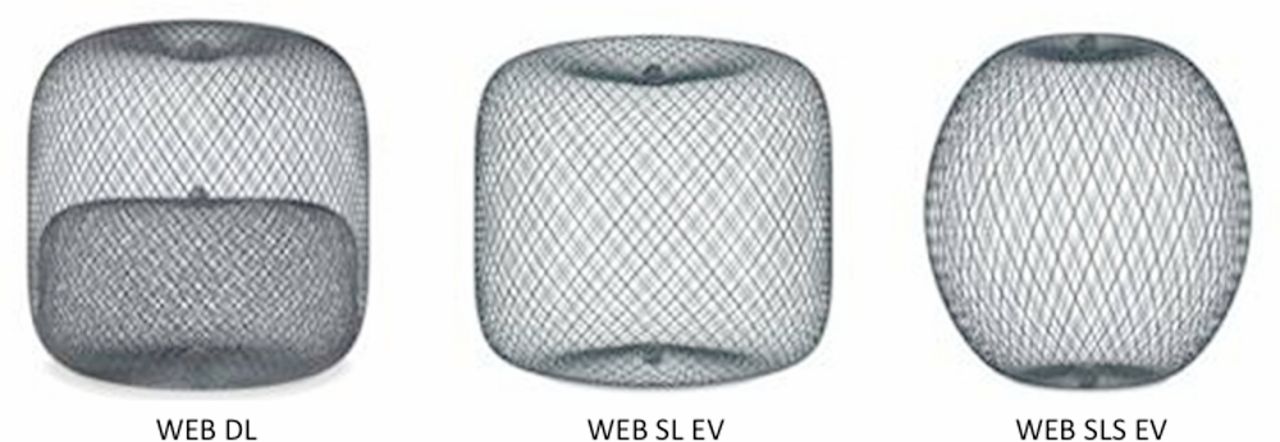
The WEB device (figure 1) was developed to treat wide-necked bifurcation aneurysms and is a retrievable, electrolytically detachable endosaccular nitinol braided cage. The WEB is by far the best studied and most-used endosaccular flow disruptor to date. The first type of WEB available was the WEB-DL (dual layer), which consisted of a second nitinol braid proximally placed in an outer nitinol braid. The double layer mesh was composed of between 216 and 288 braided wires, depending on the device size used. The WEB-SL (single layer) and WEB-SLS (single layer spherical) are lower profile versions that have between 114 and 216 braided wires. The reduction in the number of wires was aimed at balancing radial force and porosity while still promoting rapid thrombosis.11 The more spherically shaped SLS device allows for the treatment of aneurysms with more tapered necks.12 More recently, Enhanced Visualization (EV) WEB-SL and WEB-SLS devices, constructed from Drawn Filled Tube (DFT) nitinol wire, have become available. These newer WEB SL-EV and SLS-EV devices are compatible with smaller microcatheters and also allow for better intraprocedural visualization. The advancement in the design and visibility of the WEB and the ability to deliver the newer devices through smaller inner diameter microcatheters has resulted in a progressive enlargement of the clinical indications for the WEB with smaller aneurysms now being treatable with the device.
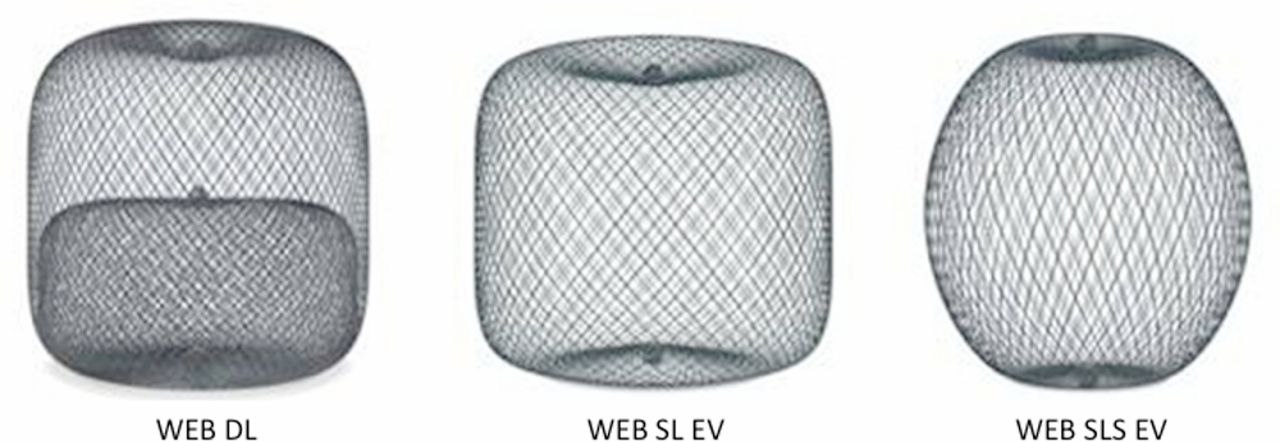
The Woven EndoBridge (WEB) device is available in three different designs. The WEB DL-EV is a mesh sphere composed of two layers of braided nitinol/platinum wires. The WEB SL-EV and WEB SLS-EV devices are composed of single layers of braided nitinol. Radio-opaque platinum/iridium markers join the proximal and distal ends of the braids and allow accurate position of the device.
Medina Embolic Device (MED)
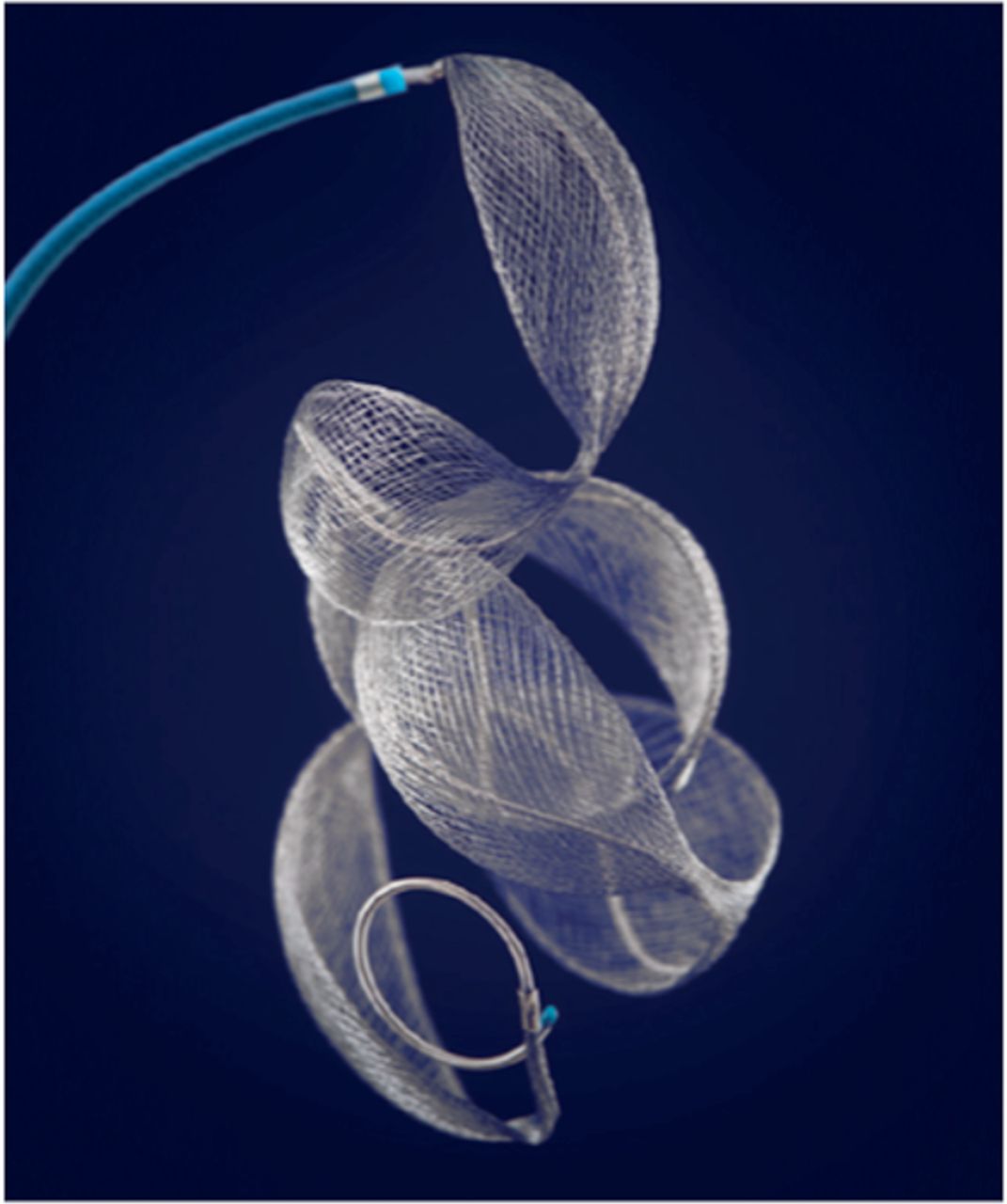
The Medina Embolic Device (MED) is a three-dimensional layered structure created from a radiopaque shape set core wire and shape memory alloy filaments (figure 2). This forms a self-expanding mesh containing multiple leaflets resembling petals that provide density and flow diversion. These petals are orientated along the long axis of the core wire and on deployment the device forms a spherical shape. The petals unfold and anchor within the sac wall and aneurysm neck. This design is meant to allow the MED to act as both a neck-bridging device and endosaccular flow disrupter. Before final mechanical detachment the device can be resheathed and redeployed in a similar fashion to standard coils. The MED is thus a hybrid system combining the design of a detachable coil with an endosaccular flow disruptor. The device is available in sizes between 5 and 10 mm and is delivered via a 0.021 inch microcatheter. The device is available in both ‘framing’ and ‘filler’ types, with framing MEDs designed to be deployed to form a basket into which filler MEDs are placed.

The Medina Embolic Device (MED) is composed of multiple self-expanding mesh ‘petals’. These petals are orientated along the long axis of the core wire and on deployment the device forms a spherical shape. The MED can be thought of as a hybrid device combining the design of a detachable coil with an endosaccular flow disruptor.
LUNA Aneurysm Embolization System (LUNA AES)
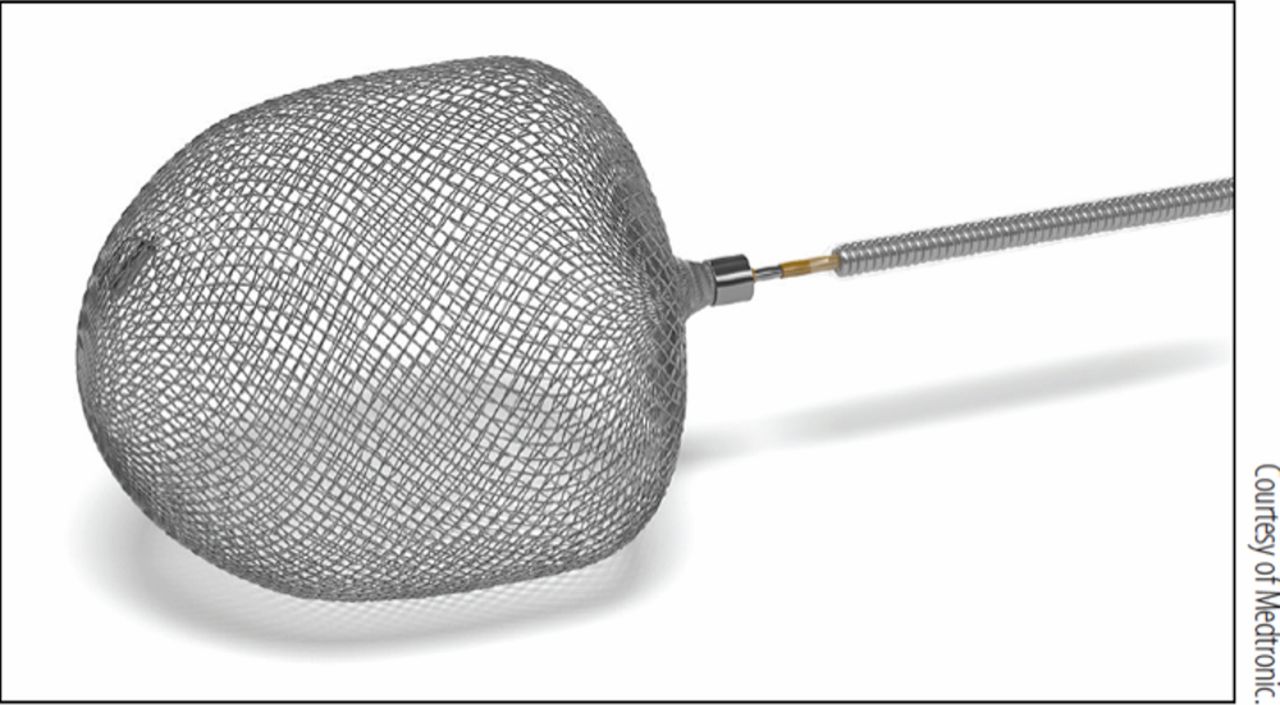
The LUNA AES is a self-expanding, mechanically detachable, ovoid endosaccular flow disruption device. It is made from a double layer of 72 nitinol 25 μm wire mesh (total 144 wires) secured at both proximal and distal ends (figure 3). The LUNA AES is indicated for saccular intracranial bifurcation and sidewall aneurysms with height 4.7–12.6 mm, width 3.0–8.5 mm, and is not limited by aneurysm dome-to-neck ratio. The device is delivered via a 0.027 inch microcatheter.
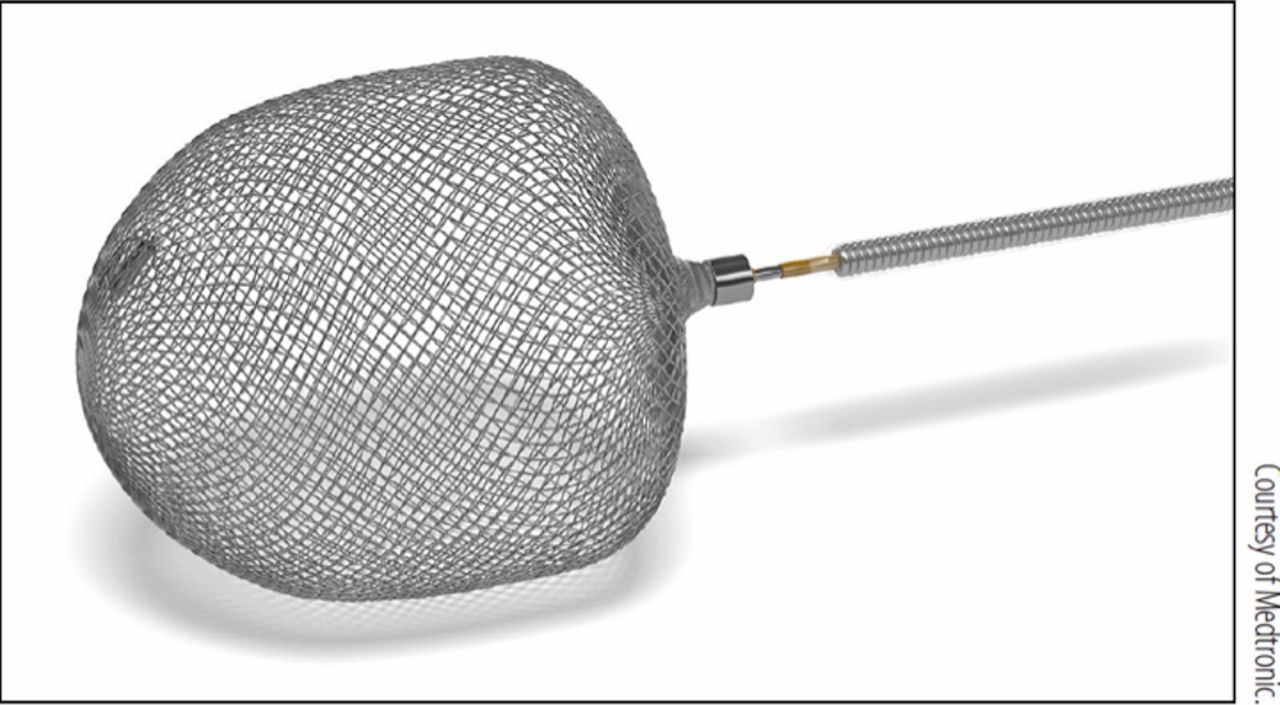
The LUNA Aneurysm Embolization System (LUNA AES) is a braided ovoid structure that is mechanically detached. A single proximal radio-opaque marker allows accurate positioning.
Contour
The Contour Neurovascular System is the newest device to enter the neurovascular market (figure 4). It is currently undergoing clinical evaluation prior to CE mark approval. The Contour is constructed from DFT nitinol, which exhibits radio-opaque properties similar to the WEB EV. There are 72 wires, which originate and terminate at the marker band. The double layer of 72 wires per layer effectively provides 144 wires across the aneurysm neck. In its unconstrained configuration the device adopts a flat disc-like shape; however, on deployment in the aneurysm and at the aneurysm neck, the device adopts a ‘cup’-like configuration (figure 4B) as it conforms to the shape of the lower half of the aneurysm and the aneurysm neck. It is self-anchoring for stability, can be resheathed, and is electrolytically detached. The device is available in 5, 7, 9, and 11 mm diameter sizes. As it is designed to be deployed at the neck and avoid the dome of the aneurysm, it is hoped that the device will be able to treat a larger array of aneurysms and will not be limited by aneurysm location or morphology. Sizing of the device is relatively straightforward and based on the maximum diameter of the aneurysm.

The Contour is the most recent device to enter the market and is currently undergoing clinical evaluation. The device is constructed from a double layer of 72 DFT wires. In its unconstrained configuration the device adopts a disc-like shape (A) and has a radio-opaque proximal marker (A, black arrow). Once deployed within the aneurysm, the device adopts a ‘cup’-like shape (B) and serves to act as both flow disruptor and flow redirector.
Preclinical studies
WEB
Initial in vivo studies of the WEB (n=24 aneurysms) demonstrated immediate complete flow cessation in 29% of aneurysms and near complete flow cessation in 54%. At follow-up, complete occlusion was seen in 33% and near complete occlusion in 58%. The histological analysis demonstrated organized thrombus within the aneurysm cavity and connective tissue forming across the aneurysm neck.13 In a further in vivo rabbit study of 36 elastase-induced aneurysms treated with the second generation WEB DL, 44% showed complete occlusion after device deployment with 67% of aneurysms showing neointimal coverage across the aneurysm neck at 12 months.14
MED
Fröhlich et al 15 sought to test the MED in 10 different patient-specific elastic vascular models. The aneurysms all arose from the internal carotid artery (ICA) and measured 4.7–11 mm. The models were connected to a pulsatile flow circuit with a blood-mimicking fluid. Intra-aneurysmal flow velocities were measured using conventional and high frequency angiography before and after each deployment. The aneurysm neck coverage by the device was assessed with flat detector CT and graded using a 3-point Likert scale (1: <50% coverage of the aneurysm orifice covered by MED petals; 2: 50–90% orifice covered by MED petals; and 3: >90% orifice covered by the MED petals). Two independent operators performed a total of 80 individual MED deployments. Analysis of flow characteristics showed a significant moderate correlation between neck coverage and intra-aneurysmal flow velocity reduction (FVR) (rho=0.42, 95% CI 0.21 to 0.59, p=0.002) as well as neck area and FVR (rho=−0.35, 95% CI −0.54 to −0.13, p=0.024). On multivariate regression analysis, both neck coverage and neck area were independent predictors of FVR. These findings were similar to those suggested by the clinical results of others.16 17
Fahed et al 18 were the first to perform an in vivo study on the MED. In this study, three different types of aneurysms were created consisting of six lateral wall common carotid artery aneurysms, 10 T-bifurcation aneurysms, and 36 lingual artery bifurcation aneurysms. Of the 48 aneurysms created, 32 were treated with the MED, either MEDs alone (n=16) (group 1) or the MED +coiling (n=16) (group 2), with a control coiling group (n=16) (group 3). The investigators noted that deployment of the first MED framing coil into its intended spheroid configuration in the necessary position to effectively close the neck with the petals was frequently unsuccessful. Petals that had initially been well placed across the aneurysm neck would alter position during continued deployment of the device, as may be expected. The deployment of the initial MED framing coil achieved contrast stagnation in only 3/16 cases (18.7%) treated with MEDs alone and in 4/16 aneurysms (25%) treated with MED plus coils. Furthermore, placement of further MEDs or coils strictly within the confines of the initial MED framer could not readily be achieved, particularly in wide-necked aneurysms. Bail-out devices, either balloons or stents, were frequently required. Only 2/16 (12.5%) group 1 aneurysms and 3/16 (18.7%) group 2 aneurysms showed complete or near complete occlusion on angiography performed at the end of the procedure compared with 10/16 (62.5%) aneurysms in group 3. At 3 months, 11/16 (68.7%) aneurysms in group 1, 9/16 (56.2%) aneurysms in group 2, and 8/16 (50%) aneurysms in group 3 showed complete or near complete occlusion and the authors state that final angiographic and pathological results were similar to standard treatment with platinum coils at 3 months.
LUNA AES
Kwon et al 19 conducted a preclinical in vivo study using the LUNA AES device. Of the 12 aneurysms treated, 10 (83%) demonstrated complete cessation of flow within 30 min. Of the 12 rabbits used in this study, four were euthanized at 1 month and angiography prior to this showed complete occlusion in three of the aneurysms and near complete occlusion in the remaining aneurysm. Histopathological assessment in these cases showed neointimal coverage at the neck in three aneurysms. Of the remaining eight rabbits, complete aneurysm occlusion was seen in seven aneurysms (87.5%). On histopathology at 3 months, all the aneurysms showed membranous tissue covering the device, organized loose connective tissue filling the entire aneurysm cavity and neointima crossing the neck. The authors suggested that the results meant that the device might be used to occlude both ruptured and unruptured intracranial aneurysms; however, they cautioned that the device is not suitable for complex, wide-necked, or fusiform aneurysms, and that the in vivo aneurysms were more regular than many aneurysms and, as such, the high rates of complete occlusion seen in the study may have been overstated.
Contour
To our knowledge there are no preclinical studies of the Contour device published in the English literature.
Clinical studies
WEB
The WEB device has been studied in several prospective, adjudicated, good clinical practice GCP studies. By some measures, therefore, it is one of the most carefully studied aneurysm therapies to date. The WEB Clinical Assessment of IntraSaccular Aneurysm Therapy (WEBCAST) study was a prospective single-arm GCP trial which evaluated the WEB-DL across 10 European centres. An independent clinical events adjudicator assessed clinical outcomes. An independent core laboratory adjudicated angiographic effectiveness outcomes. The study enrolled 51 patients with 51 aneurysms, the vast majority of which were unruptured (n=48, 94.1%). The majority of the aneurysms were located on the middle cerebral artery (MCA; n=29, 56.9%) and the basilar artery (n=12, 23.5%). In all aneurysms the neck was ≥4 mm with a mean average neck size of 5.8 mm. In the majority of cases the aneurysm fundus diameter was <10 mm (n=40, 80.4%) and the mean aneurysm size was 8.2 mm. Treatment with WEB was successfully completed in 48 patients; however, in the remaining three patients the device was removed due to it protruding into the bifurcation. Adjunctive devices were used in four patients (8.3%) that included coils and a stent to reduce protrusion of the WEB into the parent artery. Immediately post-implantation, only a minority of aneurysms showed complete occlusion (4/48, 8.3%). 25% (12/48) showed a neck remnant and an aneurysm remnant was reported in the remaining cases. Six-month angiographic follow-up was available in 41 cases and, of these, 23 (56.1%) showed complete occlusion, 12 (29.3%) showed neck remnant, and the remaining 6 had an aneurysmal remnant. Of these 41 patients, 39 had been treated only with the WEB device and in this cohort the results were similar, with 34 having either complete occlusion or neck remnant (87.2%). In terms of clinical complications, there were no intraoperative ruptures and no bleeding or rebleeding was seen in the 6-month follow-up period. Thromboembolic events occurred in 9/51 (17.7%), one of which resulted in a periprocedural stroke with postprocedural hemiparesis and aphasia (modified Rankin Scale (mRS) 1, reduction of fine motor skill with the right hand and, when tired, feeling slow with language) that persisted at 6 months (1.9%, 1/51). There were two deaths during the 6-month follow-up, one related to the presenting subarachnoid hemorrhage and another related to an underlying cancer (4.2%).20
The French Observatory evaluated the WEB-DL, WEB-SL, and WEB-SLS. It was a single-arm, prospective, multicenter GCP study that recruited patients at 10 sites across France to evaluate the use of the WEB in treatment of bifurcation aneurysms. The study enrolled 62 patients with 63 aneurysms, the majority of which were unruptured (n=51, 81.0%). Most of the aneurysms were located in the anterior circulation (n=54, 85.7%). Just over half of the aneurysms were located on the MCA (n=32, 50.8%), with 16 aneurysms (25.4%) located on the anterior communicating artery. The majority of the aneurysms were ≤10 mm in maximum diameter (n=52, 82.5%) and were wide-necked, ≥4 mm (n=57, 90.5%). Approximately half of the patients were treated with WEB-DL and half with WEB-SLS/SL. In all except one patient (98.4%) the treatment with WEB was performed successfully. Adjunctive devices were used in 7/62 aneurysms (11.3%). Of the 63 aneurysms treated, 58 aneurysms were evaluated at 1 year and complete occlusion was seen in 30/58 (51.7%) with neck remnant in 16/58 (27.6%). Interestingly, there was no significant difference in the outcome of patients treated with either the WEB-DL or the WEB-SL/SLS.
Intraoperatively, there were nine thromboembolic events in 8/62 patients (12.9%), one of which was associated with a permanent deficit (1.6%). Intraoperative rupture was seen in 1/62 patients (1.6%) and was asymptomatic. In another patient intracranial hemorrhage was detected on a CT scan performed 24 hours post-procedure and it was believed to be due to the antiplatelet medications. Mortality at 1 month was 0% and morbidity was observed in 2/62 (3.2%), one of which was related to a thromboembolic complication and another related to worsening of pre-existing mass effect from a partially thrombosed basilar tip aneurysm. At 1 year 59 patients were evaluated and there had been two deaths (3.4%), one related to the previously mentioned partially thrombosed basilar aneurysm and another unrelated to the treated aneurysm.
The WEBCAST 2 study was designed to evaluate the WEB single layer enhanced visualization devices (WEB SL-EV and WEB SLS-EV). It was a European study that enrolled patients at 10 centers. The study enrolled 55 patients with 55 aneurysms, four of which were ruptured. As with the WEBCAST study, the most common location for the aneurysms was the MCA (n=25, 45.5%) followed by the anterior communicating artery (n=16, 29.1%) and the basilar artery (n=9, 16.4%). The mean aneurysm dome size was 6.7±2.3 mm (range 2.8–17 mm) and the mean neck size was 4.6±1.1 mm (range 2.5–8 mm). Treatment with the WEB was successful in 53 patients (96.4%). An adjunctive device was needed in a single case. Immediate post-implantation angiographic assessment was not provided. One-year imaging follow-up was available for 50 patients, with complete occlusion seen in 27 (54%) and neck remnant in 13 (26%). Thrombeombolic complications were reported in eight cases (14.5%) and intraoperative rupture was seen in one patient (1.8%). At 1 month, procedural morbidity was observed in one patient (1.8%) and related to a thromboembolic event (mRS 3). At 1 year post-procedure, 51 patients were available for clinical assessment and at this point there had been one death related to a large retroperitoneal hemorrhage encountered during the WEB procedure (2%).21
Taking all the data from the WEBCAST, WEBCAST 2, and French Observatory studies, 168 patients were included with a total of 169 aneurysms, 14/169 (8.3%) of which were ruptured, 150/169 (88.8%) were unruptured, and 5/169 (3.0%) were recanalized following previous coiling. Approximately half (50.9%) of the aneurysms were located on the MCA with 36/169 (21.3%) located on the anterior communicating artery, 30/169 (17.8%) on the basilar artery, and the remaining 17/169 (10.1%) located on the ICA terminus. The mean aneurysm size was 7.0±2.5 mm (range 2.8–17.0 mm) and mean neck size was 5.2±1.6 mm (range 2.4–13.8 mm). The neck was ≥4 mm in 144/169 aneurysms (85.2%). Treatment was successfully performed in 163/169 aneurysms (96.4%) and adjunctive devices were used in 12/163 aneurysms treated with the WEB (7.4%). Anatomical results at 1 year were evaluated in 152/168 patients (90.5%) and 153/169 aneurysms (90.5%). Complete occlusion was seen in 81/153 (52.9%) and neck remnant was seen in 40/153 (26.1%), hence an adequate occlusion of 121/153 (79.1%). There was no significant difference in the rates of adequate occlusion between the different WEB devices, suggesting that the newer WEB-SL/SLS devices are as effective as the original WEB-DL while being easier to deploy via smaller microcatheters. There was no bleeding from an incompletely occluded aneurysm or neck remnant during the follow-up. Eleven aneurysms were retreated (6.9%). Clinical evaluation was available at 1 month in 167/168 patients (99.4%). Morbidity in each of these trials was defined as mRS >2 if the preoperative mRS was ≤2 (or in the case of a ruptured aneurysm) and as an increase of 1 point when the preoperative mRS was >2. At 1 month, thromboembolic events were noted in 24 patients (14.4%) with the majority being asymptomatic (n=11) or symptomatic without clinical sequelae (n=8), as defined above. Intraprocedural rupture was seen in two patients (1.2%) and intracranial hemorrhage in one patient (0.6%). At 1 year, 153 of the 168 patients enrolled were clinically evaluated. During this period of the follow-up there were five deaths (all-cause mortality 3.3%), three of which were unrelated to the aneurysm or procedure, one related to a worsening of mass effect from a partially thrombosed aneurysm (neuro-related mortality 0.7%), and one from a retroperitoneal hemorrhage (procedure-related mortality 0.7%)22 (see figures 5 and 6).

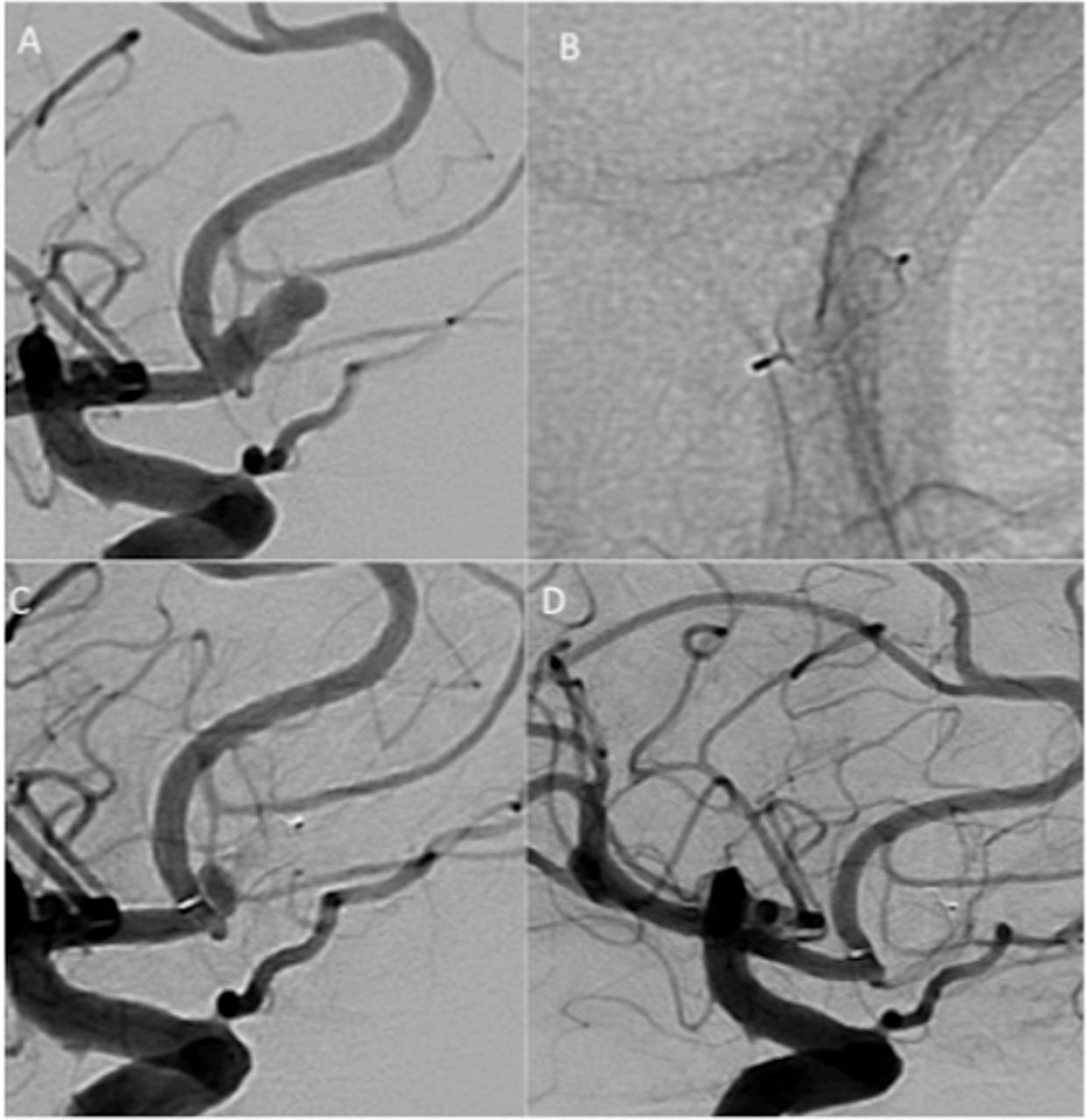
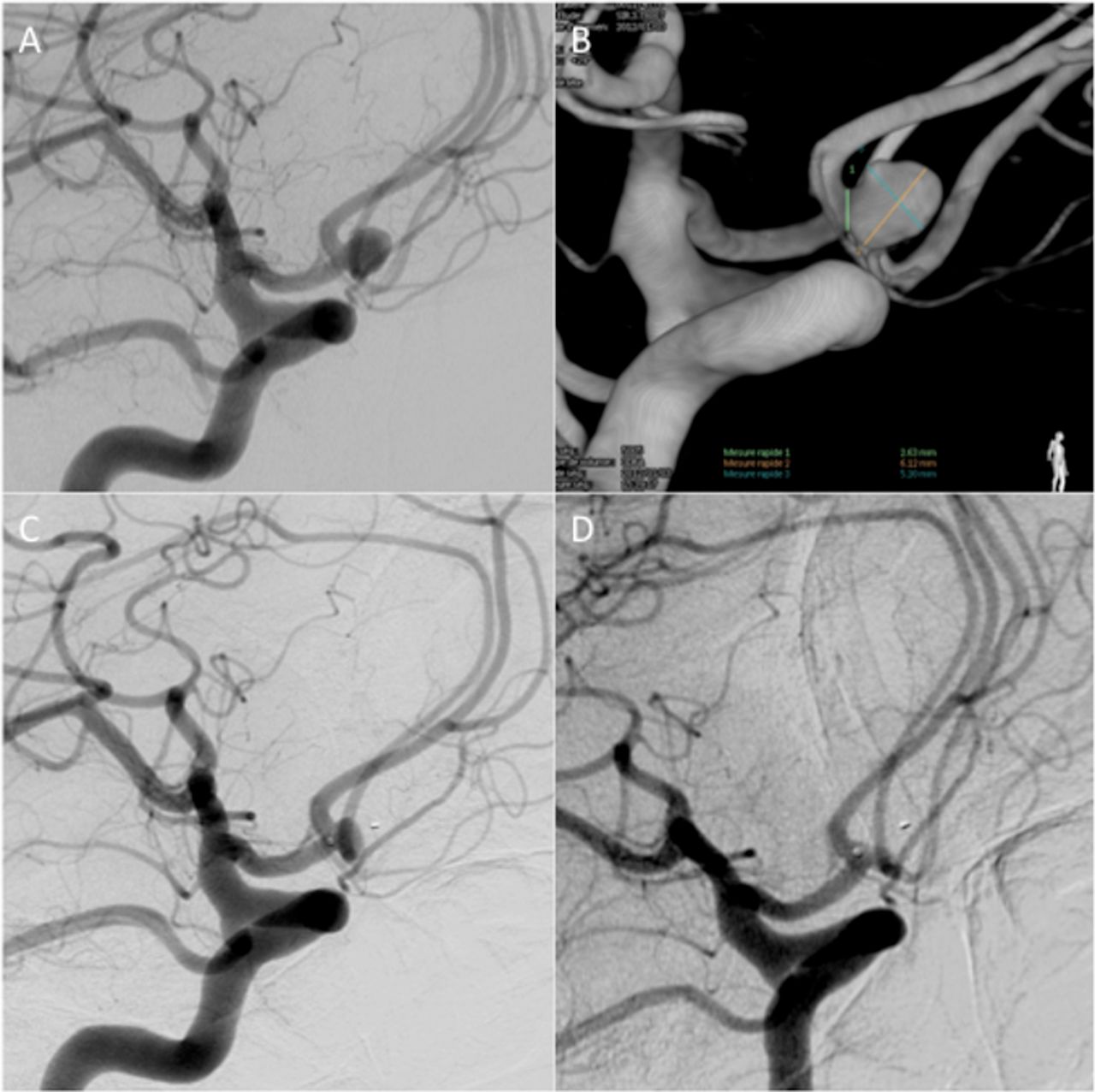
An incidental pericallosal aneurysm (A) was discovered in a patient with a positive family history of subarachnoid hemorrhage in a first-degree relative. The mean width of the aneurysm was 5 mm and mean height 5 mm. Treatment was performed with a single WEB SL-EV 6×4 mm (B). There was continued opacification of the aneurysm at the end of the procedure (C); however, on follow-up angiography at 6 months there was complete occlusion of the aneurysm (D).
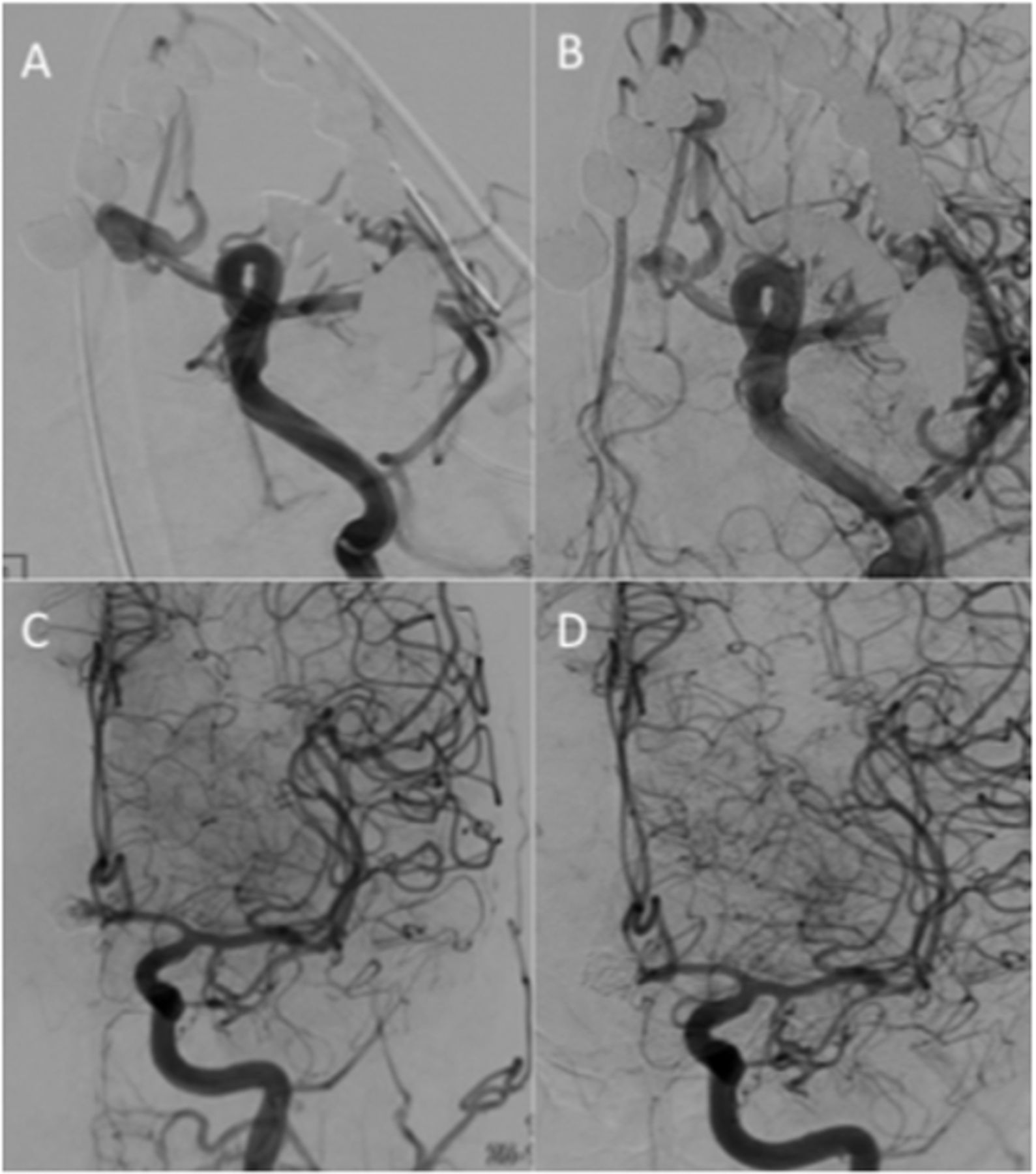
An aneurysm of the anterior communicating artery was found after routine investigation. The aneurysm had a mean dome width of 3.8 mm and mean dome height of 8.5 mm (A). The decision was taken to treat using a WEB SL-EV 6×5 mm, which conformed accurately to the oblong shape of the aneurysm (B) and demonstrates the softness of the device. There was significant contrast stasis seen at the end of the procedure (C) with complete occlusion of the aneurysm on 3-month angiography (D).
The US WEB-IT study is a prospective single-arm pivotal trial conducted at 21 US and six international centers.23 The study enrolled 150 patients with wide-necked bifurcation aneurysms (WNBAs) of both the anterior and posterior circulation with neck width ≥4 mm or dome-to-neck ratio ≥1 and <2. Both ruptured (n=9, 6.0%) and unruptured (n=141, 94.0%) aneurysms were included in the study, with the majority of the aneurysms located in the anterior circulation (n=91, 61.7%); the most common location was the basilar tip (n=59, 39.3%). The mean dome width was 6.4 mm (range 3.6–11.4 mm) and the mean neck size was 4.8 mm (range 2.0–8.2 mm). The mean dome-to-neck ratio was 1.4 (range 1.0–2.0). Three different WEB devices were available for use in the trial including the WEB DL-EV, WEB SL-EV, and WEB SLS-EV. The WEB SL-EV was the most frequently used subtype and accounted for just under three-quarters of all devices (n=107, 72.3%). Successful deployment of the WEB was achieved in 148 patients (98.7%). In the two cases that were unsuccessful, one was due to vessel tortuosity and the other was due to improper device size availability. There was one primary safety event (0.7%)—a day 22 post-procedure lobar hemorrhage. This was not directly related to the WEB device but to antiplatelet medication and underlying cerebrovascular disease. The mortality rate in the WEB-IT study was 0%. Fluoroscopy times averaged 30 min and, while this is more efficient with regard to actual operating times compared with other assisted coiling techniques, there is a considerable time commitment in case analysis, planning, and correct device selection beforehand.24 The WEB-IT study described two patients who had a periprocedural subarachnoid hemorrhage that resulted in minimal symptoms despite both being treated with dual antiplatelet therapy. The authors state that this is a reflection of the speed at which the WEB device is able to achieve hemostasis and aneurysm protection even in the setting of intraprocedural rupture. This finding was also observed in the early in vivo animal studies using the WEB.13 The 12-month results of the WEB-IT study were recently published. Of the 150 patients enrolled, 147 were followed up clinically at 12 months and 143 underwent follow-up imaging with catheter angiography. Complete aneurysm occlusion was seen in 53.8% (77/143) with adequate occlusion seen in 84.6% (121/143). Subgroup analysis, including gender, race, aneurysm location, site experience, sac width (<8 mm, ≥8 mm), aneurysm rupture status, and diameter of WEB used, all suggest there was no difference in the rate of achievement of either complete or adequate occlusion. Progressive aneurysm occlusion was seen over time and between the last angiogram at the time of treatment and the initial follow-up angiogram at 6 months; 91.5% (121/141) of the aneurysms showed an improvement in the occlusion status. Similarly, most aneurysms (88.5%; 116/131) were either stable or continued to improve in appearance between the 6-month and 12-month follow-up angiography. Overall, 14 patients (9.8%) underwent retreatment of the aneurysm. Clinically, only one primary safety event occurred (0.7%) and there were no events between 30 days and 12 months. Similarly, in the acute cases there were no recurrent aneurysm ruptures. On the basis of these data, the FDA approved the WEB device for use in the USA on December 31, 2018.
Although ruptured aneurysms were included in the previously mentioned trials as well as in retrospective series,25 there remained a concern that the WEB would not provide adequate protection against repeat rupture. To address this concern, the Clinical Assessment of WEB in Ruptured Aneurysms (CLARYS) trial was designed. CLARYS26 is a prospective multicenter evaluation conducted in 13 interventional neuroradiological departments in France and Germany. The study design meets GCP standards with independent monitoring and core laboratory evaluation. The primary endpoint is defined as the rebleeding rate at 1 month post-procedure. The secondary endpoints are the rate of adverse events related to the device, the procedure or the disease, the neurological evaluation at 1 month and 1 year based on mRS, the occlusion at 1 year based on the WEB Occlusion Scale (WOS), and the procedure and fluoroscopy time.
Between February 2016 and September 2017, 60 patients (31 women (51.7%); mean age 54.5±1.49 years) with 60 aneurysms were included in the study. The aneurysm locations were at the anterior communicating artery (26/60, 43.3%), the MCA bifurcation (23/60, 38.3%), the basilar apex (7/60, 11.7%), the anterior cerebral artery (2/60, 3.3%), the ICA terminus (1/60, 1.7%) and the posterior communicating artery (1/60, 1.7%). The WEB device was successfully implanted in 56/60 cases (95.0%). Although the full results of the study are yet to be published, topline results have been presented at several international conferences with the primary endpoint of repeat hemorrhage not occurring in a single patient (0%). Mortality at 1 month was 1.7% (n=1), which occurred 6 days after the subarachnoid hemorrhage and was a result of severe vasospasm. Morbidity, defined as mRS >2 if the pre-rupture mRS ≤2 or mRS +1 if pre-morbid mRS >2, was 15% (n=9) with five cases related to the initial subarachnoid hemorrhage, three related to vasospasm, and one case related to hydrocephalus. These initial results suggest that the WEB provides robust protection of ruptured aneurysms.
MED
The first publication regarding the clinical use of the MED device was published by Turk et al.27 This study included nine patients, seven of whom were treated solely with the MED. A MED framer coil was placed in all the aneurysms and the number of devices deployed ranged between 1 and 7 (average 2.8 devices per aneurysm), with the aneurysms measuring between 4.5 mm and 17 mm. Follow-up imaging was limited in this initial publication, and although only three of the aneurysms had follow-up at 1 month, all three showed >95% occlusion. The authors believed that, as with endoluminal flow diversion and other endosaccular flow disrupters, there would be progressive aneurysm occlusion over time. Subsequently Aguilar-Peréz et al published their single-center experience on the use of the MED. This group reported the results of 15 consecutive patients with 16 aneurysms. In this series an average of 3.4 MEDs per aneurysm were used (range 1–9). Follow-up imaging was available in 11 patients with modified Raymond–Roy occlusion II or better seen in eight patients. However, a criticism of the paper was that adjunctive devices were used in the majority of the cases, and although the authors explained in detail the potential problems with the MED, it did not allow an assessment of the MED to occlude aneurysms alone. Subsequently, Sourour et al 28 presented their findings of 12 patients with 13 aneurysms. In this series the authors used a single MED framer to obtain a basket in 12/13 aneurysms. They then proceeded to implant further MED fillers, standard coils, or both. The authors state that, as this was their first experience with the device, even if total exclusion of the aneurysm was seen, coils were used to fill the basket created by the MED framer. In this series three ruptured aneurysms were treated and average aneurysm dome size was 7.5±1.5 mm (range 5–10 mm) with an average neck size of 4.4±1.1 mm (range 2.2–7.3 mm). The authors also reported that an average of 2.5 deployments were needed to obtain a satisfactory position of the MED and, to our knowledge, this is the only publication that documented the number of deployments/redeployments needed to obtain a satisfactory position. Angiography at the end of the procedure showed 8/13 aneurysms (61.5%) were completely excluded from the circulation and this rose to 9/12 (75%) at 6 months. Haffaf et al 29 recently reported the 18-month angiographic results of 19 patients harboring 20 aneurysms. Embolization with the MED was feasible in all but two aneurysms. The authors reported that complete aneurysm occlusion was seen in 11/18 (61%) aneurysms at the end of the procedure with progressive occlusion seen on delayed angiography at 18 months (12/15, 80%). However, as with the series of Aguilar-Peréz et al, adjunctive devices (coils) were used in the majority of the aneurysms in both the series by Sourour et al and Haffaf et al and the ability of the MED to occlude aneurysms alone could not be assessed. The publication by the Karolinska group16 demonstrated the efficacy of the MED to occlude aneurysms when used as a sole device and, of the nine aneurysms treated with a single MED, only one aneurysm was completely occluded (11.1%) with four having a neck remnant (44.4%) (figures 7 and 8). Interestingly, the majority of aneurysms treated with multiple MEDs were completely occluded at follow-up (3/4, 75%). The authors recommended that a single MED should not be used to treat aneurysms given the low overall aneurysm occlusion rate. They went on to state that one of the principal problems was the inability to determine if the leaflets of the MED were covering the aneurysm neck, and this could explain the relatively low aneurysm occlusion rates seen by a single device.
An unruptured aneurysm arising from the left A1/A2 junction (A) treated with a single Medina Embolic Device (B) with reduction of flow seen within the aneurysm on the end-procedural angiography (C) and complete occlusion on the 3-month follow-up angiogram (D).

An unruptured anteriorly pointing aneurysm arising from the M1 segment of the middle cerebral artery (A) was treated with a single Medina Embolic Device. Contrast filling of the aneurysm was seen at the end of the procedure (B). The aneurysm remained patent on the 3-month angiogram (C) as well as on the delayed 11-month angiogram (D). The patient has been retreated with standard coiling.
This theory was later confirmed by Fröhlich et al 15 in their in vitro study and it confirmed one of the major weaknesses of the MED relative to the WEB and LUNA AES, both of which are guaranteed to cover the aneurysm neck if deployed correctly. The published reports on the use of the MED have reported acceptable safety with no aneurysmal ruptures and low levels of thromboembolic complications. Similarly, although only a few ruptured aneurysms have been treated, the device appears safe in this scenario. Complications encountered in the series by Perez et al 17 included one patient where the MED failed to detach and so was removed and the aneurysm was subsequently coiled. Compaction of the MEDs was also noted, requiring further coiling of the aneurysm remnant. This compression phenomenon has been reported with the WEB device—for example, in 25% cases reported by Sivan-Hoffman et al 30 and in 57.2% in the series by Cognard and Januel.31 Sourour et al 28 did not report this phenomenon as in the majority of their cases they used coils within the MED and the use of coils by these investigators was, in their early cases, to prevent compression of the MEDs. The Karolinska series also did not observe compaction of the MEDs; however, they did report changes in configuration of the device in two aneurysms. Similar changes were reported with the WEB device, with Cognard and Januel31 reporting a radiological deterioration in 71% of treated aneurysms and lower rates of shape change reported by Sivan-Hoffman et al.30
LUNA
A prospective European multicenter study to evaluate the safety and efficacy of the LUNA AES included 63 patients with 64 aneurysms.32 The majority of these aneurysms were unruptured (60/63, 95.2%), 76.6% being bifurcation or terminal aneurysms and majority being small to medium size (<5 mm 39.1%, 5–10 mm 57.8%) (figure 9).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A single LUNA Aneurysm Embolization System was implanted into an unruptured 6 mm anterior communicating artery aneurysm (A and B). There was persistent contrast opacification at the neck of the aneurysm seen on angiography performed at the end of the procedure (C). On delayed angiography (12 months) there was complete occlusion of the aneurysm with no evidence of device compaction or parent vessel stenosis.
Immediate postoperative adequate occlusion was low (11/61, 18%), with adequate occlusion, defined as Raymond–Roy occlusion grade I or II, achieved in 78% (49/60) and 79.2% (42/53) at 12 months and 36 months, respectively. At all time points the occlusion rate of small aneurysms was higher than for medium-sized aneurysms. The study had only two large aneurysms (>10 mm), one showing a neck remnant and the other showing complete filling. Parent vessel compromise immediately after the procedure, related to protrusion of the device, was not infrequent with a 3.3% rate of complete occlusion, a 3.3% rate of significant stenosis (>50% of parent vessel) and 6.6% with mild stenosis of ≤50%, with two ischemic events reported in the latter category. There was a significant relationship between LUNA AES protrusion and the occurrence of an ischemic event (p=0.0442).
Two of the 63 patients had major strokes (3.2%), one due to a procedure-related carotid dissection due to guiding catheter navigation that resolved without sequelae within 4 days and a second that occurred within 12 months and was related to treatment of a different aneurysm (mRS 3). Interestingly, there were no periprocedural complications directly attributed to the LUNA device itself. The rates of thromboembolic events were comparable to those seen with the WEB studies (9.6%, 7.6%, and 15%)10 33 34 as well as in large coiling series (7.1% in ATENA35 and 12.5% in CLARITY36). There was no occurrence of new or recurrent hemorrhage from any of the treated aneurysms.
Four patients had to be retreated by 12 months and three additional patients were retreated by 36 months follow-up. This was either due to migration (into a large partially thrombosed aneurysm) of the device resulting in recanalization of the aneurysm or suboptimal deployment of the device that was not appreciated at the time of the procedure. No evidence of a compression phenomenon, as described with the WEB device, was observed.
This study had a low morbidity and mortality. Furthermore, none of the LUNA AES-treated aneurysms rebled during the 36-month follow-up period. Whereas the WEB was developed to treat wide-necked aneurysms, the LUNA AES was developed to treat a broader array of aneurysms. The current study, however, had a majority of small to medium-sized aneurysms that were predominantly unruptured.
Technical nuances and limitations
WEB
The initial strategy when sizing the original WEB devices was to base the choice of WEB on the maximal diameter of the aneurysm and to aim to form the proximal recess at the detachment zone of the device. However, it was determined that this strategy resulted in undersizing of the device and recanalization at the aneurysm neck. Subsequently, sizing of the WEB devices changed to a +1 mm in diameter and −1 mm in height relative to these respective sizes in the treated aneurysms. It is believed that this oversizing in the diameter of the WEB results in greater mechanical stability of the device and reduces the likelihood of device compression. Oversizing of the device is possible due to the softness of the WEB. Herbreteau et al 37 analyzed 39 patients treated with the WEB and, according to the rule of +1 mm/−1 mm, the device was undersized in 11/39 patients (28.2%). Among the 38 patients with short-term angiographic follow-up, 10 had an undersized WEB (26.3%) and 28 had an appropriately sized WEB (73.7%). A change in the shape of the WEB was observed in 12/38 (31.6%) with short-term follow-up. A similar rate of shape change was observed among the undersized and appropriately sized WEBs. In patients with undersized WEBs, complete occlusion was seen in 50.0% of cases (5/10) and neck remnant in 20.0% of cases (2/10). In patients with an appropriately sized WEB, complete occlusion was seen in 64.3% (18/28) and neck remnant in 28.6% (8/28). Adequate occlusion was therefore seen in 70.0% of undersized WEB cases and 92.9% of appropriately sized cases. Complete aneurysm occlusion was seen more frequently in those cases where there was no shape change of the WEB (76.9% vs 25.0%, p=0.04). Therefore, although appropriate sizing of the device does not significantly alter the likelihood of a change in the shape of the WEB, it is important in achieving adequate occlusion.
‘Compression’ of the WEB cage was observed at first follow-up in eight of 14 cases (57.2%) and in an additional three of seven cases (42.8%) on delayed angiography in the series by Cognard and Januel.31 Other investigators have sought to further investigate these findings.37 38 The exact underlying mechanism involved is still debated. Although this may be related to device compression from arterial blood pressure—the so-called water-hammer effect—it may also be related to retraction of the device secondary to aneurysmal thrombosis or sac shrinkage.37 The WEB device has a concave proximal surface that creates a proximal recess often visible on follow-up examinations. This recess has been erroneously reported as a neck remnant and, as such, a 4-point scale to evaluate aneurysm exclusion has been proposed, including one grade that was opacification of the proximal recess (besides complete occlusion, neck remnant, and aneurysm remnant). All cases of opacification of the proximal recess were stable in the WEBCAST and French Observatory studies, and if these cases were included as complete occlusion, aneurysm status at mid-term follow-up was 69.0% complete occlusion, neck remnant in 20.7%, and aneurysm remnant in 10.3%.
MED
Sizing of the MED is based on similar principles to coils. The device can be withdrawn and repositioned as with coils, although it is difficult to predict the location of the petals as well as positioning of the petals at the aneurysm neck, which appears to be critical to the success of the device. It is also difficult to determine the position of the petals using advanced on-table imaging such as VasoCT. This difficulty in understanding the exact geometry of the device inside aneurysms has led some authors to caution against using a single MED to treat aneurysms,16 while others have negated these problems by using various adjunctive devices.17 39
LUNA
Sizing and device selection of the LUNA relies on the maximum height and width as measured on the diagnostic angiogram. After consulting the LUNA sizing chart (finding the height in the columns and the width in the row headings, the intersection indicating recommended implant size letter code (‘B’ through ‘J’)), the LUNA device product labelled with the corresponding size letter code is then selected. The main limitation for sizing is an irregularly shaped aneurysm. Due to the ovoid shape of the device, it is important that the proximal marker of the device slightly protrudes into the parent artery to avoid undersizing. The other limitation is the necessity to use a 0.027 inch microcatheter to enable device delivery.
Meta-analyses
Meta-analyses are currently only available for the WEB device given the limited published literature for the LUNA AES, the MED, and the Contour.
WEB
A meta-analysis conducted by Lv et al 40 analysed the results of 935 patients with 967 aneurysms with further subgroup analysis of studies published pre- and post-2013. The most frequent aneurysm locations were MCA (42.8%), the anterior communicating artery (23%), and the basilar artery (20.8%). The technical success rate of the WEB treatment procedure was 97% (95% CI 96% to 98%). In 11% of cases (95% CI 7% to 14%) adjunctive devices were used, and these were more likely to be required in patients with larger aneurysms and older patients; however, the use of adjunctive devices decreased in studies published after 2013. The thromboembolic rate was 8% (95% CI 6% to 11%), with a higher rate seen in studies published pre-2013 (10%) compared with studies published post-2013 (6%). The hemorrhagic complication rate was 2% (95% CI 1% to 3%). The morbidity pre-2013 was 5% (95% CI 2% to 9%) and post-2013 was 1% (95% CI 0% to 2%), with higher morbidity associated with the WEB-DL. Eighteen studies were used to evaluate the occlusion rate of the aneurysms, as this was not reported in one of the studies published. At short-term and mid-term follow-up, the complete occlusion rate was 55% (95% CI 50% to 60%) and the adequate occlusion rate was 81% (95% CI 76% to 85%). These results were similar to those reported by previous groups,41 42 although the difference seen over time was not previously shown. This suggests that, as with all new devices and techniques, patient selection, improvement in device design, and improved operator technique have had an impact on patient outcomes.
Current approval status
WEB
The WEB has received a CE mark and is available for clinical use in Europe. The FDA approved the WEB device for use in the USA on December 31, 2018
MED
The MED is currently not available for clinical use and is under development into a product known as the LIO device.
LUNA
The LUNA AES device is currently not available for clinical use and is under development into a product known as the ARTISSE device.
Contour
The Contour device does not currently have a CE mark. A multicenter European trial is currently being conducted.
Challenges and future prospects
WEB
The continued evolution of the WEB device has resulted in the device indication being expanded and, in all likelihood, data demonstrating the effectiveness of the device in ruptured aneurysms will be confirmatory. However, as the device is still often used to treat wide-necked aneurysms, the use of antiplatelet agents may be prudent in some cases. A surface modified WEB, similar to the PED Shield (Medtronic, Irvine, California, USA), would be a significant advantage in this regard.
MED and LUNA
As both the MED and the LUNA are undergoing redevelopment, it is impossible to speculate on how these new devices will behave. As mentioned above, surface modified devices would certainly be advantageous as would devices that could be deployed via 0.17 inch microcatheters, similar to the smaller WEB devices.
Contour
To date there is no published literature on the Contour device and therefore speculation on future iterations is not possible.
Conclusion
Endosaccular flow diversion continues to evolve at a rapid pace. Newer devices and advances in technology will hopefully allow safer and more robust aneurysm occlusion. Although early results are promising, longer term studies are required. Long-term follow-up data at 2, 3, and 5 year follow-up will shortly be available for the WEB, and this will allow a greater understanding of the efficacy of this device in particular. Similarly, the results of CLARYS are eagerly awaited.
References
Footnotes
Contributors PBh: manuscript preparation, review, editing, guarantor. SU: manuscript preparation, review, editing. CC: review, editing, contribution of cases. MP: review, editing. N-AS: review, editing. PBr: review, editing. TA: review, editing. LM: review, editing. KW: review, editing. DF: review, editing. ASA: review, editing. MS: review, editing, case contribution. HH: review, editing. LP: review, editing. LLLY - editing, review of manuscript, data collection.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PBh: consultant for phenox. CC: consultant for Stryker, Medtronic, Cerenovus and Microvention. MP: consultant for Medtronic, Stryker, MicroVention, Balt, Penumbra, Base Camp Vascular (share holder). N-AS: investor in Medina. PBr: consultant for Cerenovus. TA: consultant for Ablynx, Amnis Therapeutics, Anaconda, Cerenovus–Neuravi, Medtronic-Covidien, Rapid Medical. DF: consultant for Medtronic, Microvention, Penumbra, Balt, Cerenovus, Stryker; research support: Siemens, Microvention, Penumbra, Cerenovus; stockholder: Marblehead, Neurogami, Vascular Simulations; board member: Vascular Simulations. ASA: consultant for Balt, Johnson and Johnson, Leica, Medtronic, Microvention, Penumbra, Scientia, Siemens, Stryker; shareholder in Bendit, Cerebrotech, Endostream, Magneto, Marblehead, Neurogami, Serenity, Synchron, Triad Medical, Vascular Simulations. MS: consultant for Cerenovus and Archer Research. HH: co-founder and shareholder for phenox GmbH and femtos GmbH. LP: consultant for Balt, Cerus Endovascular, MicroVention, Phenox, Vesalio, Penumbra.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.