 Lorena Jiménez-Sánchez1
Lorena Jiménez-Sánchez1 Olivia K. L. Hamilton1,2Una Clancy2,3Ellen V. Backhouse2,3
Olivia K. L. Hamilton1,2Una Clancy2,3Ellen V. Backhouse2,3 Catriona R. Stewart2,3
Catriona R. Stewart2,3 Michael S. Stringer2,3
Michael S. Stringer2,3 Fergus N. Doubal2,3
Fergus N. Doubal2,3 Joanna M. Wardlaw2,3,4*
Joanna M. Wardlaw2,3,4*- 1Translational Neuroscience PhD Programme, Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom
- 2Edinburgh Dementia Research Centre in the UK Dementia Research Institute, Edinburgh, United Kingdom
- 3Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom
- 4Lothian Birth Cohorts, University of Edinburgh, Edinburgh, United Kingdom
Background: Cerebral small vessel disease (SVD) is a common cause of stroke, mild cognitive impairment, dementia and physical impairments. Differences in SVD incidence or severity between males and females are unknown. We assessed sex differences in SVD by assessing the male-to-female ratio (M:F) of recruited participants and incidence of SVD, risk factor presence, distribution, and severity of SVD features.
Methods: We assessed four recent systematic reviews on SVD and performed a supplementary search of MEDLINE to identify studies reporting M:F ratio in covert, stroke, or cognitive SVD presentations (registered protocol: CRD42020193995). We meta-analyzed differences in sex ratios across time, countries, SVD severity and presentations, age and risk factors for SVD.
Results: Amongst 123 relevant studies (n = 36,910 participants) including 53 community-based, 67 hospital-based and three mixed studies published between 1989 and 2020, more males were recruited in hospital-based than in community-based studies [M:F = 1.16 (0.70) vs. M:F = 0.79 (0.35), respectively; p < 0.001]. More males had moderate to severe SVD [M:F = 1.08 (0.81) vs. M:F = 0.82 (0.47) in healthy to mild SVD; p < 0.001], and stroke presentations where M:F was 1.67 (0.53). M:F did not differ for recent (2015–2020) vs. pre-2015 publications, by geographical region, or age. There were insufficient sex-stratified data to explore M:F and risk factors for SVD.
Conclusions: Our results highlight differences in male-to-female ratios in SVD severity and amongst those presenting with stroke that have important clinical and translational implications. Future SVD research should report participant demographics, risk factors and outcomes separately for males and females.
Systematic Review Registration: [PROSPERO], identifier [CRD42020193995].
Introduction
Cerebral small-vessel disease (SVD) is a disorder of the brain small penetrating blood vessels leading to white and deep gray matter damage, and is a major cause of stroke (1) and dementia (2).
Sex differences occur in many vascular diseases (3), and they can also be expected in the context of SVD. SVD is most commonly sporadic, although there are rare familial types, like cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), which although not sex-linked, seems to affect males more severely than females (4). Covert SVD is common in older persons, where differences in male:female incidence or severity have not been assessed. Several studies of stroke of any type have recruited more males than females and reported a higher age-adjusted incidence in males, but higher severity in females. However, as reviewed elsewhere, it is unclear whether these conclusions reflect underlying sex-specific biological differences, recruitment bias, or other factors (5). On average, females are older than males at stroke onset, more likely to live alone and have more severe baseline deficits (6), which could explain their increased pre-hospital delay, and their higher severity in first-ever acute stroke (7). These factors can affect females' eligibility for stroke research studies, with a bias toward recruitment of milder strokes, and for stroke treatment, as females are less likely to be treated with IV thrombolysis than males (8). Interestingly, females were more likely to refuse participation in stroke clinical trials than males independently of their age (9).
Globally, females tend to live longer than males but there is a lack of sex and gender-stratified data in aging research (10) that may impede more personalized care in older populations; especially when biological factors, treatments, or social disparities may differ between sexes (11). Understanding male:female differences in incidence or severity of disease, particularly of common diseases like SVD, is now a World Health Organization imperative.
We aimed to explore if there are sex differences in covert or clinical presentations of SVD by assessing the sex ratio of participants with clinical or radiological evidence of SVD recruited to a range of studies, and whether any difference could be explained by male:female differences in risk factors or the severity of SVD features.
Methods
We followed the Preferred Reported Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines and registered the protocol on PROSPERO on July 2, 2020 (CRD42020193995) (12).
Data Sources and Search Strategy
We identified relevant studies in two ways.
First, we examined studies that had been included in four recent published systematic reviews of different aspects of SVD, whose search terms were similar as for the current work, and identified studies that met our current inclusion criteria (see below). The four systematic reviews addressed (a) early life risk factors for SVD (13), (b) cognitive dysfunction in SVD (14), (c) neuropsychiatric and cognitive symptoms in SVD (15), and (d) cerebral blood flow in SVD (16). We used the four published systematic reviews as a highly efficient way to access a large relevant literature, a practice which is now endorsed as part of the drive toward reducing research waste, improving efficiency, and best practice in evidence synthesis (17, 18). These systematic reviews had already been thoroughly screened and quality assessed, had each been conducted according to PRISMA guidelines, used relevant search terms, performed study quality assessment, had undergone peer review, and been published (Table 1) (13–16). Each systematic review had assessed a very large literature on a different aspect of SVD, enabling us to assess a very large number of relevant studies as efficiently as possible.
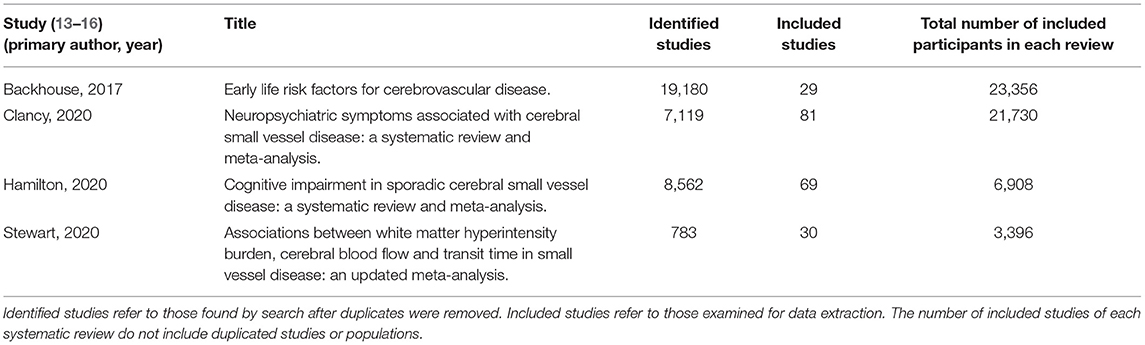
Table 1. Systematic reviews.
Second, we designed an independent search to supplement all the studies collected from the four systematic reviews with recent publications. We used a search strategy modified from a published protocol (14) to identify studies including participants with clinical (stroke or cognitive presentations) or non-clinical presentations of sporadic or monogenic SVD (e.g., CADASIL). Stroke presentations included lacunar syndromes with corresponding small subcortical infarct on neuroimaging, or that excluded other causes of symptoms. Cognitive presentations included vascular cognitive impairment, either vascular mild cognitive impairment—VaMCI—or vascular dementia—VaD. Non-clinical presentations included radiological evidence of SVD—e.g., white matter hyperintensities (WMH), lacunes of presumed vascular origin, small subcortical infarcts or cerebral microbleeds (CMBs) on brain magnetic resonance imaging (MRI) (19)—in the absence of clinical diagnosis (generally in community-dwelling populations), i.e., “covert” SVD. We aimed to explore trends across time by comparing recent and previously published studies (see Results, Trends across time) and decided to use January, 1, 2015 as the starting publication date for recent studies. Thus, January, 1, 2015 was the first date used for the independent search. We searched MEDLINE through OVID for human studies published in English or Spanish from January, 1, 2015 to May, 26, 2020 as follows: Cerebral Small Vessel Diseases/ OR (small vessel disease or small vessel-disease or CSVD or SVD).ti.ab. OR stroke,Lacunar/ OR [(lesion* or hyperinten*) adj3 white matter].ti.ab. OR Leukoaraiosis/ OR lacune*.ti.ab. OR [(lacun* or subcort* or ischemi* or ischaemi* or silent or microscopic) adj3 lesion*).ti,ab.]. Since the used search strategy was modified from one of these systematic reviews' protocol, only the most recent 150 journal articles among the 4,871 filtered results were examined to avoid retrieving duplicated studies that were already present in the database. The electronic search was carried out on May, 26, 2020.
Study Selection
We included cross-sectional and longitudinal studies published in English or Spanish that considered clinical diagnosis of SVD, radiological markers for SVD or studies reporting on patients with stroke that provided data according to stroke subtype (cortical or lacunar stroke). We excluded studies that did not report proportions of males and females or stroke subtype in the case of studies in stroke, review papers other than the included systematic reviews, editorials, communications, case reports, case series and conference abstracts, studies about other neurodegenerative conditions (e.g., Parkinson's disease, Alzheimer's Disease, non-vascular, or mixed dementia), inflammatory disorders (e.g., encephalitis/meningitis/vasculitis), single-sex populations (e.g., pregnancy studies), and genetic-based studies that only recruited from families. To avoid possible confounding factors related to large vessel disease, studies that recruited participants based on cardiovascular events (e.g., heart failure) and diffuse cardiovascular disease (e.g., atherosclerosis) were also excluded. The population of interest was patients presenting with stroke-related SVD (lacunar stroke), cognitive impairment found to have radiological features of SVD on neuroimaging, or participants with no clinical presentation found to have radiological features of SVD on neuroimaging (covert SVD). SVD radiological features included WMH, lacunes, small subcortical infarcts, CMBs, silent brain infarcts, or prior hemorrhage.
Where more than one study presented data on the same population, the study considering the most information about SVD clinical diagnosis, radiological markers, or risk factors for SVD was selected.
Data Extraction
Screening, full-text review, study selection and data extraction were independently carried out by five authors (LJ-S, OKLH, EVB, UC, and CRS). Studies included in the published systematic reviews had already been assessed by two researchers. Studies identified in the new literature search were assessed by one researcher and cross-checked with another researcher in the case of uncertainty about inclusion.
We extracted data on the primary author, date of publication, country of recruited participants, study type (cross-sectional or longitudinal), clinical or non-clinical presentation of participants (including lacunar or subcortical stroke or hemorrhagic forms of SVD, subjective memory or cognitive complaints, VaMCI, VaD, or covert SVD), number of subjects, total sex ratio of participants, mean age of participants and sex-stratified mean age of participants, stratified sex ratio by clinical diagnosis of SVD, radiological features of SVD (presence and severity of WMH, lacunes, small subcortical infarcts, CMBs, silent brain infarcts or prior hemorrhage) or SVD score if provided. We calculated mean ages if not reported and data were available. Hypertension and current or ever-smoking data were recorded if available, since these are key modifiable risk factors known to worsen SVD (20), and calculated sex-stratified percentages of hypertension and smoking. An initial screening of papers indicated that there would be few sex-stratified data to explore other risk factors. We only extracted baseline data in longitudinal studies.
Statistical Analysis
We performed all analyses and generated plots using R (version 3.2.3) (21). We calculated sex ratios of study participants or SVD groups of all the included studies and compared sex ratio per type of SVD presentation. Our principal summary measure was the median sex ratio per study setting, SVD presentation and severity.
Since recruitment can be affected by different factors across different settings, we classified studies into community-based, hospital-based, or mixed (where participants were recruited from both community and hospitals). To investigate whether differences in sex ratios were influenced by study size, we calculated a new variable: Δ sex ratio = |a constant of the global population sex ratio (22) – sex ratio of each study|. We log-transformed sizes of recruited populations due to their skewed distribution and then assessed the correlation of Δ sex ratio with the log-transformed size of the recruited populations per study population type.
To explore trends across time and countries, we classified studies by year of publication and country of recruited participants, respectively. To explore trends across severity and presentations of SVD, we then classified participants into healthy to mild SVD (mild covert SVD) vs. moderate to severe SVD (stroke presentations, cognitive presentations, moderate to severe covert SVD and genetic SVD; detailed in Table 2).
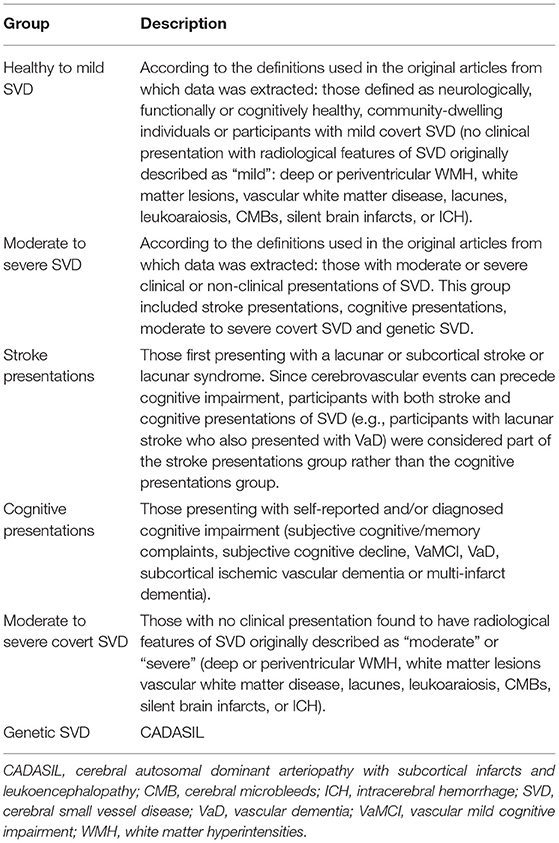
Table 2. Study classification by SVD severity and presentation.
For quantitative analyses, we used Shapiro-Wilk tests to check for data normality. Sex ratio and sex-stratified data were not normally distributed, so we used non-parametric statistical tests. We used the Mann-Whitney-Wilcoxon test to explore comparisons between two groups and the Kruskal-Wallis test to explore comparisons between more than two groups. If the result of the Kruskal-Wallis test was significant, we further analyzed data by pairwise Mann-Whitney-Wilcoxon followed by Bonferroni post-hoc correction. We assessed correlations using Spearman's rank correlation coefficient. In text, we present data as median (interquartile range, IQR) with significance threshold set at p < 0.05.
Study Quality Assessment
We performed a quality assessment of all the studies identified through the systematic reviews and the supplementary search of the recent literature as previously (14), rated on a scale from 0 to 8 according to STROBE guidelines, and calculated the median and IQR of the quality score. To check sensitivity, we re-ran the meta-analyses excluding studies with quality scores lower than the median quality score of all included studies.
Risk of Bias Assessment
Bias refers to factors that can systematically affect the observations and conclusions of the study, making them differ from the truth (23). Relevant biases for this systematic review could be explored in studies that compared SVD incidence, severity, or risk factors in strata by sex. However, since very few studies have been published specifically on male-to-female ratios in SVD, and none (to our knowledge) aimed specifically to assess male:female differences in SVD, risk of bias was not assessed in this study.
Results
We found 241 relevant journal articles in the four published systematic reviews and the independent search. After filtering by language, full texts of 228 publications were assessed against inclusion/exclusion criteria (Figure 1). We extracted data and meta-analyzed 123 studies that met the inclusion/exclusion criteria (n = 36,910 total participants) (24–146). Two studies included genetic SVD (CADASIL) (79, 83) and 121 studies included sporadic SVD (characteristics of the included studies are summarized in Supplementary Table 1). Studies were conducted from 1989 to 2020 in 23 countries across six continents (Europe 43; Asia 39; North America 35; South America 3; Australia 2; Africa 1).
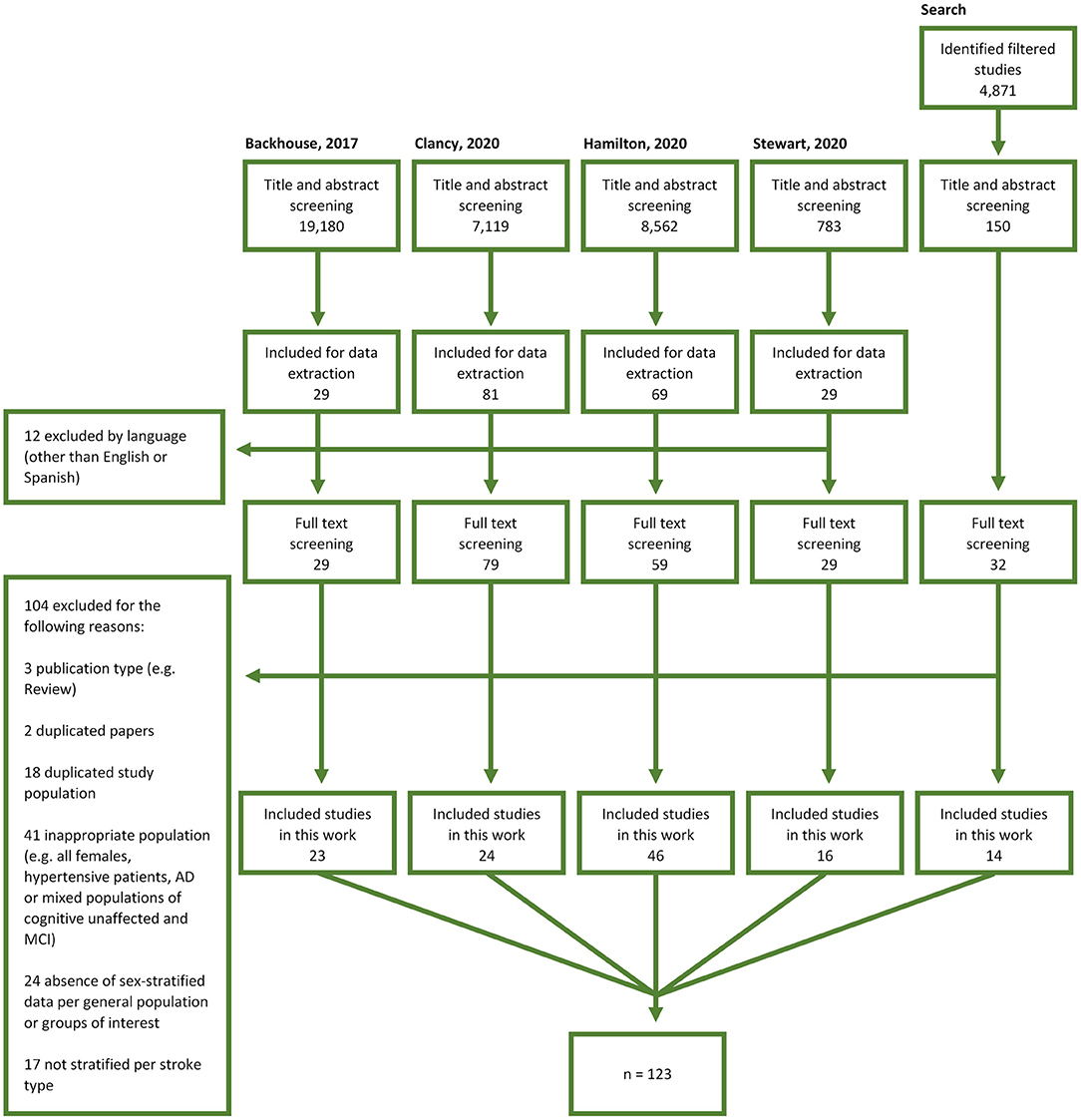
Figure 1. Study selection flow diagram. AD, Alzheimer's Disease; MCI, mild cognitive impairment.
None of the included studies reported data regarding non-binary participants. Hence, for simplicity and without prejudice, sex ratios are referred to as male:female ratios.
Trends Across Study Settings
Our literature search retrieved 53 community-based (n = 29,323 participants) (24–76), 67 hospital-based (n = 7,337 participants) (77–143), and three mixed studies (n = 250 participants) (144–146). The global sex ratio of all included studies was 0.92 (0.65). Sex ratios differed across study setting (H = 24.35, df = 2, p < 0.001), being greater in hospital-based studies (i.e., more males than females) than in community-based studies: 1.16 (0.70) vs. 0.79 (0.35), respectively (pcorrected < 0.001; Figure 2A). Considering that the mean age of the participants of the included studies was 67, the sex ratio of community-based studies was closer to the expected general population sex ratio (0.89 in a 70-year old population) (22) than that of the hospital-based studies.
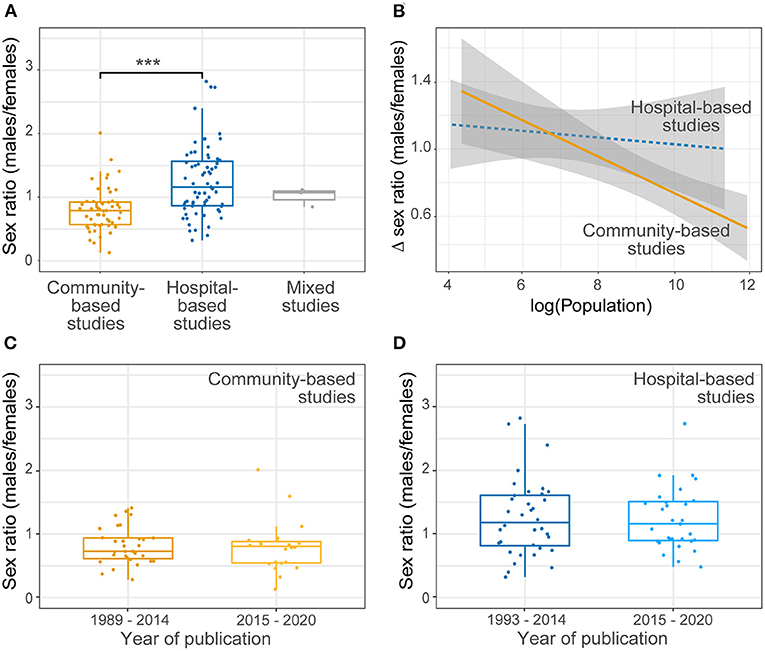
Figure 2. Sex ratio of SVD studies across study setting and time. (A) Comparison of sex ratios per study type. Significant differences were found between sex ratios of community-based (CB) and hospital-based (HB) studies (pcorrected < 0.001). (B) Correlation between the sex ratio difference and the size of the recruited sample. Δ sex ratio = |sex ratio of general population – sex ratio of each study|. Given that the mean age of the participants of the included studies was 67, general population sex ratio corresponds to 70-year old population (89 males per 100 females) (22). There was a negative correlation between Δ sex ratio and the size of the population recruited in community studies (yellow, rhoSpearman = −0.46, p < 0.001) but not in hospital studies (blue, rhoSpearman = −0.10, p = 0.43). (C,D) Comparison of sex ratios across time. No significant differences were found between sex ratios of recent studies compared with those previously published considering all included studies (n2015−2020 = 53 vs. n1989−2014 = 67, U = 1,814, p = 0.75), (C) CB studies (n2015−2020 = 22 vs. n1989−2014 = 31, U = 372, p = 0.58) or (D) HB studies (n2015−2020 = 31 vs. n1993−2014 = 36, U = 551, p = 0.93). ***p < 0.001.
Sex ratio varied with study size in community-based but not in hospital-based studies: in community-based studies, the sex ratio was closer to that of the general population when the sample size was larger (rhoSpearman = −0.46, p < 0.001; Figure 2B); there was no effect of sample size on sex ratio in hospital-based studies (rhoSpearman = −0.10; p = 0.43; Figure 2B).
Trends Across Time
We classified studies per year of publication into recent (from 2015 to 2020) and previously published (until and including 2014) studies.
Considering all the included studies, there were no significant differences between sex ratios of recent studies compared with earlier publications (U = 1,814, p = 0.75). This finding was consistent after classifying by study type (U = 372, p = 0.58 in community-based studies; U = 551, p = 0.93 in hospital-based studies; Figures 2C,D). Mixed studies (144–146) were not included in this analysis since only three were retrieved by our literature search, all published recently.
Trends Across Countries
We classified community-based and hospital-based studies by country of recruitment (Figure 3). For clarity, studies that recruited participants from more than one country (37, 63, 83, 109, 127) and mixed studies (144–146) were excluded.
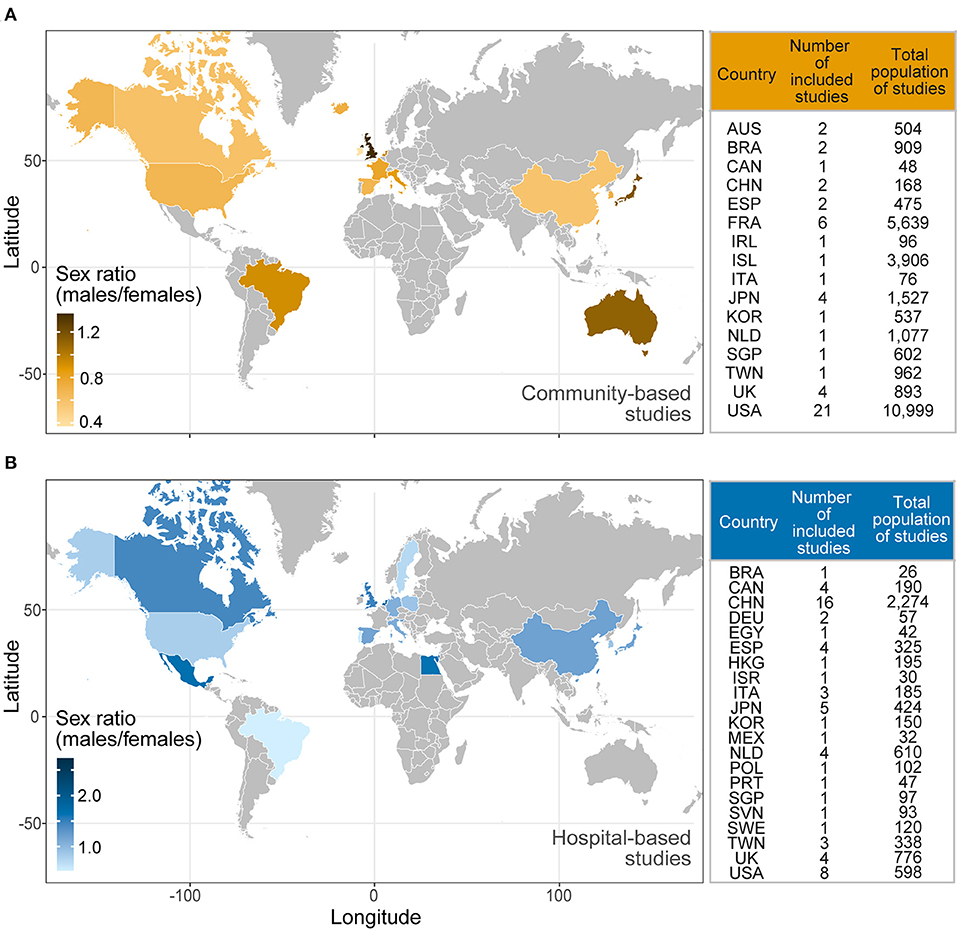
Figure 3. Sex ratio of SVD studies across the world. Colored world maps representing the mean sex ratio of the total number of participants of (A) community-based and (B) hospital-based studies. Darker shades in the color gradient correspond to higher sex ratios (i.e., more males than females). The tables on the right specify the country of recruited participants, the number of included studies and the total population of included studies per study type. Neither multicentre nor mixed studies were represented in these maps. AUS, Australia; BRA, Brazil; CAN, Canada; CHN, China; DEU, Germany; EGY, Egypt; ESP, Spain; FRA, France; HKG, Hong Kong; IRL, Ireland; ISR, Israel; ITA, Italy; JPN, Japan; KOR, Korea; MEX, Mexico; NLD, The Netherlands; POL, Poland; PRT, Portugal; SGP, Singapore; SVN, Slovenia; SWE, Sweden; TWN, Taiwan; UK, United Kingdom; USA, The United States of America.
Amongst community-based studies, the highest sex ratio was found in participants recruited from the United Kingdom [1.36 (0.19), four studies, n = 893] and the lowest in participants recruited from the Republic of Ireland (0.37, one study, n = 96; Figure 3A). The largest recruited population came from the USA (21 studies, n = 10,999 participants), with a median sex ratio of 0.67 (0.36). Regarding hospital-based studies, the highest sex ratio was found in participants recruited from Singapore (2.73, one study, n = 97) and the lowest in participants recruited in Brazil (0.53, one study, n = 26; Figure 3B). The largest recruited population came from China (16 studies, n = 2,274 participants), with a median sex ratio of 1.08 (0.48).
There were no obvious regional trends across countries for sex ratio vs. the total number of participants for either community-based or hospital-based studies.
Severity and Presentation of SVD
The included studies enrolled n = 25,972 healthy to mild SVD participants (no SVD presentation or mild covert SVD, Table 2) and n = 10,938 moderate to severe SVD participants (clinical presentation and/or high radiological burden of SVD, Table 2). The sex ratio was higher in healthy to mild SVD [1.08 (0.81)] than in moderate to severe SVD [0.82 (0.47)], U = 3,031, p < 0.001 (Figure 4A).
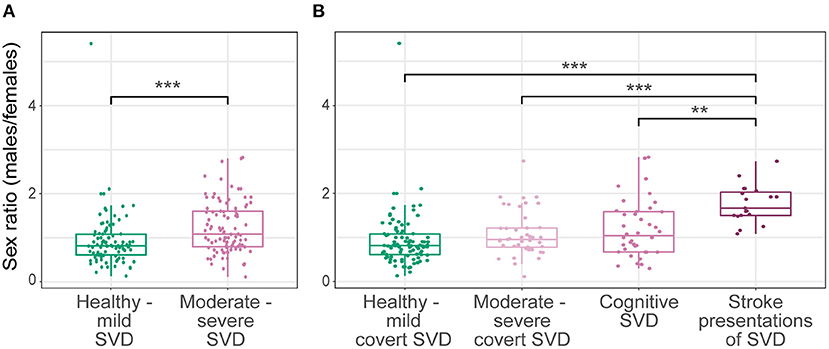
Figure 4. Sex ratio across SVD severity and presentation. Sex ratio of healthy to mild SVD compared with (A) moderate to severe SVD and (B) stratified moderate to severe SVD. Significant differences were found between SVD severity groups i.e., sex ratios of healthy to mild SVD and moderate to severe SVD (A; U = 3,031, p < 0.001). Significant differences were also found between SVD presentation groups (H = 36.58, df = 3, p < 0.001) i.e., stroke presentations of SVD compared with healthy to mild covert SVD, moderate to severe covert SVD or cognitive SVD (B; pcorrected < 0.001, pcorrected < 0.001, pcorrected = 0.003, respectively). **p < 0.01, ***p < 0.001.
We further classified moderate to severe SVD participants into cognitive or stroke presentations or moderate to severe covert SVD (Table 2, Figure 4B). We excluded CADASIL studies due to insufficient data (79, 83). Sex ratios differed significantly between SVD presentations (H = 36.58, df = 3, p < 0.001). Participants with stroke showed the highest sex ratio, 1.67 (0.53), compared with healthy to mild covert SVD [0.82 (0.47), pcorrected < 0.001], cognitive SVD [1.03 (0.91), pcorrected = 0.003], and moderate to severe covert SVD [0.96 (0.44), pcorrected < 0.001].
Since community-based studies recruited mostly healthy participants and presented lower sex ratios, we repeated the severity analysis restricted to hospital-based studies (77–143), and found similar trends. Across SVD severity, the sex ratio was higher in moderate to severe SVD [1.26 (0.87)] than in healthy to mild SVD [0.90 (0.58)], U = 1,240, p < 0.001. Across SVD presentations, the sex ratio was higher in stroke presentations [1.67 (0.55)] than in healthy to mild covert SVD [0.90 (0.58), pcorrected < 0.001], cognitive SVD [1.11 (0.81), pcorrected = 0.037], and moderate to severe covert SVD [1.13 (0.87) pcorrected = 0.02], H = 21.82, df = 3, p < 0.001.
Age and Risk Factors for SVD
Only 10 studies (38, 64, 65, 69, 73, 81, 102, 111, 136, 143) (2,953 participants) provided sufficient data to calculate the sex-stratified participants' age. There was no significant difference in median age between total recruited males [63.78 (9.71)] and females [64.45 (13.71), U = 49.5, p > 0.99].
Only two studies (73, 81) provided data to calculate sex-stratified SVD risk factors (hypertension and smoking), which were insufficient to perform further analyses.
Quality Assessment
The median study quality score was 5.5 (1). As a sensitivity analysis, quantitative analyses were re-run excluding all studies with a quality score <5.5/8. All the trends observed in the total included studies were consistent in the subset of higher-quality studies (score ≥ 5.5/8; Supplementary Table 2).
Discussion
This meta-analysis of 123 studies (24–146) including 36,910 participants demonstrates sex differences in SVD across study settings, by SVD severity and presentation. A greater male-to-female ratio was found in hospital-based (77–143) compared to community-based studies (24–76) (Figure 2), and in moderate to severe SVD, particularly in stroke presentations (Figure 4). The pattern was consistent across recent (2015–2020) and previous (1989–2014) studies (Figures 2C,D), and world regions (Figure 3). To the best of our knowledge, this is the first systematic review and meta-analysis to explore sex differences in SVD and has important implications. The apparent presence of more severe SVD in males, particularly amongst those presenting with stroke, may indicate differences in risk factor exposures, susceptibility to SVD, adherence to risk factor interventions, or differences in study recruitment. Awareness of these differences, which were robust to study location and population, may help inform approaches to mitigate the long-term effects of covert SVD and for secondary prevention of SVD-related stroke. Unfortunately, very few studies reported risk factor differences between males and females and even age was not commonly reported. Furthermore, future studies should report male and female demographics, risk factors and outcomes, not just total sample data.
The different sex ratios between community-based and hospital-based studies may reflect differences in recruitment in these settings. Typically, females are older and have more disability at stroke onset (7), which may affect study eligibility. For example, ischemic stroke patients older than 80 years have higher rates of disability following thrombolysis treatment (147) and are less likely to be recruited into stroke trials (148). Furthermore, women with stroke may present with non-traditional symptoms like altered mental status (149), which could be overlooked or misdiagnosed (150, 151), and are important since atypical and neuropsychiatric symptoms are increasingly recognized to associate with SVD (15). Sex differences in clinical presentations are also present in dementia (152) but none of the included studies reported these in VaCI or VaD. Moreover, informal carers of dependent persons in the UK are more likely to be middle-aged women with multiple roles until later life (70+) (153). Thus, females may be reluctant to participate in studies due to care responsibilities or may normalize their early symptoms while providing care. Caregiving roles vary by country (154), socioeconomic status and culture of care (155), which might explain why more females seemed to participate in Chinese hospital-based studies compared with the UK or Canada (Figure 3B) since Chinese males are traditionally the predominant caregivers for older parents (156). Some of the aforementioned factors that may alter female recruitment to SVD studies have recently been highlighted as contributors to lower enrolment of women in stroke clinical trials more generally (157).
It could also be that SVD is more prevalent and/or severe in males than in females, increasing the likelihood of males becoming participants in studies investigating severe SVD. In support of this, male-sex was an independent predictor of severity of SVD in an adjusted analysis, albeit in a 62% male population (20). Similarly, a greater prevalence of stroke, higher cognitive impairment and cerebral atrophy have been reported in men with CADASIL (158). Sex differences can be driven by sex-specific biological factors e.g., sexual dimorphism in endothelial function (159). In premenopausal females, oestrogens enhance endothelial production of vasodilator factors (160). This may explain young males having greater vasoconstrictor tone compared to pre-menopausal females (159) and male endothelial function becoming suboptimal under certain insults. We found no differences in age between recruited males and females, although fewer data were available for this analysis. Different lifestyle-related risk factors could also contribute to the sex-specific severity of SVD, e.g., utilization of preventative health care services, smoking, or hypertension. Interestingly, the prevalence of smoking and hypertension is higher among males in most countries (161, 162), varying with ethnicity (163). Unfortunately, there were insufficient data to determine if sex-specific risk factor effects were driving the sex ratio difference in SVD severity and presentation.
The unequal sex ratios found here may be explained by factors with different contributions across different settings, evidenced by the different effect of study size on sex ratio within community-based and hospital-based studies (Figure 2B), or in the context of higher SVD severity and stroke presentations. The lack of difference between sex ratios of recent and earlier studies (Figures 2C,D) suggests that the same factors may have operated long term.
The implications for future research and clinical practice are varied and important. The lack of sex-stratified data, previously reported in brain structural studies (164) and aging research (10), hampers translational research and personalized care. Results should be reported and analyzed by sex, especially when biological factors, treatments or social disparities may differ between sexes (11). This was addressed recently (165, 166) in support of the Sex and Gender Equity in Research (SAGER) guidelines (167) and the European Commission second report on Gendered Innovations (168), which provides guidance for researchers to incorporate sex, gender and intersectional analysis across several research topics. Future studies should also identify and try to avoid recruitment bias, explore whether SVD is more frequently underestimated or misdiagnosed in females and investigate reasons why males may be more severely affected. Larger sample sizes may help to reduce sampling variability at least within community-based studies with a majority of functionally healthy individuals (Figure 2B). If the disease in females is going unrecognized, doctors and the public could be educated to better recognize atypical symptoms in females. If males are more severely affected or exposed to certain lifestyle factors, trials may need to target drivers of males' vulnerability and health promotion campaigns could be designed to have more impact on males.
This study had limitations. First, it was not possible to explore common risk factors of SVD due to the scarcity of sex-stratified data. Also, other risk factors and their differences between sexes were not explored (e.g., lower educational attainment, associated with increased risk of SVD in later life) (13). Most studies are from industrialized countries (Figure 3), so our results might not fully represent other populations. Since this study relied on studies' own criteria for SVD severity, future explorations could investigate heterogeneity in study criteria and attempt further standardization efforts. Future work could also explore the sex-stratified functional status of participants, which may affect eligibility criteria and result in exclusion of females who are more functionally disabled (6, 8, 169).
The study also has strengths. We included studies from four recent systematic reviews, which covered different aspects of SVD (and therefore likely different literatures), each had assessed a large literature, and the source files were immediately available to us. We did not use our older systematic reviews as the included literature would not have been so up to date or comprehensive. We hope that our approach might encourage other groups to evaluate their high-quality systematic reviews in the same way. A broad approach was taken to capture changes across time, study settings, different cultural or ethnic groups, SVD severity and presentation. The included studies were conducted from 1989 to 2020, recruited 36,910 participants from the community and/or hospitals in 23 countries across six continents, and explored a wide range of SVD radiological features and presentations. Our results highlight sex-specific variability in study participation, SVD severity, and presentation. These findings are relevant for future research and clinical practice, but much more work is needed to unmask sex-specific biological and social disparities and disentangle their contributions to sex differences in SVD.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
LJ-S carried out the independent literature search, extracted the data, performed the meta-analyses, and drafted the manuscript. OKLH, EVB, UC, and CRS carried out the literature search of their corresponding systematic reviews and provided their databases and reviewed and edited the manuscript. MSS co-supervised one of the systematic reviews (conducted by CRS) and checked and edited the manuscript. FND co-supervised one of the systematic reviews (conducted by UC) and checked and edited the manuscript. JMW conceived and managed the project, designed the protocol, checked the search strategy, supervised the contributing meta-analyses, reviewed uncertain articles, advised on the meta-analysis and interpretation of data, and reviewed and edited the manuscript. The final draft of the manuscript was approved by all authors.
Funding
This research was funded, in part, by the Wellcome Trust [Grant No. 108890/Z/15/Z]. For the purpose of open access, the author has applied a CC BY public copyright license to any Author Accepted manuscript version arising from this submission. LJ-S is a Translational Neuroscience PhD student funded by Wellcome (108890/Z/15/Z). OKLH was a Translational Neuroscience PhD student funded by the College of Medicine and Veterinary Medicine at the University of Edinburgh. OKLH was supported by a Translational Neuroscience PhD student funded by the College of Medicine and Veterinary Medicine at the University of Edinburgh. UC was funded by a Chief Scientist Office of Scotland Clinical Academic Fellowship (CAF/18/08) and Stroke Association Princess Margaret Research Development Fellowship (2018). EVB was funded by the Sackler Foundation, the Stroke Association, British Heart Foundation and Alzheimer's Society through the R4VaD Study. MSS was funded by the Fondation Leducq (ref no. 16 CVD 05) and EU Horizon 2020 (PHC-03-15, project No 666881, SVDs@Target) and the MRC UK Dementia Research Institute at the University of Edinburgh (UK DRI LTD, funded by the UK Medical Research Council, Alzheimer's Society and Alzheimer's Research UK). FND was funded by a Stroke Association Garfield Weston Foundation (TSALECT 2015/04) Senior Clinical Lectureship and NHS Research Scotland. JMW was funded by the Stroke Association, British Hearth Foundation, Row Fogo Charitable Trust, Fondation Leducq (Perivascular Spaces Transatlantic Network of Excellence), and EU Horizon 2020 (SVDs@Target) and the MRC UK Dementia Research Institute at the University of Edinburgh (UK DRI LTD, funded by the UK Medical Research Council, Alzheimer's Society and Alzheimer's Research UK). All authors hold grants from government/charitable agencies. The funding sources had no role in the study design, execution, analysis, interpretation of the data, decision to publish, or preparation of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer CC declared a past co-authorship with one of the authors JMW to the handling editor.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.756887/full#supplementary-material
Abbreviations
CADASIL, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; CMBs, cerebral microbleeds; MRI, magnetic resonance imaging; ICH, intracerebral hemorrhage; SVD, cerebral small vessel disease; VaD, vascular dementia; VaCI, vascular cognitive impairment; WMH, white matter hyperintensities.
References
1. Pasi M, Cordonnier C. Clinical relevance of cerebral small vessel diseases. Stroke. (2020) 51:47–53. doi: 10.1161/STROKEAHA.119.024148
2. Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. Lancet Neurol. (2019) 18:684–96. doi: 10.1016/S1474-4422(19)30079-1
3. Gao Z, Chen Z, Sun A, Deng X. Gender differences in cardiovascular disease. Med Novel Technol Dev. (2019) 4:100025. doi: 10.1016/j.medntd.2019.100025
4. Chabriat H, Hervé D, Duering M, Godin O, Jouvent E, Opherk C, et al. Predictors of clinical worsening in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy: prospective cohort study. Stroke. (2016) 47:4–11. doi: 10.1161/STROKEAHA.115.010696
5. Carcel C, Woodward M, Balicki G, Koroneos GL. Sousa D, Cordonnier C, et al. Trends in recruitment of women and reporting of sex differences in large-scale published randomized controlled trials in stroke. Int J Stroke. (2019) 14:931–8. doi: 10.1177/1747493019851292
6. Di Carlo A, Lamassa M, Baldereschi M, Pracucci G, Basile AM, Wolfe CD, et al. Sex differences in the clinical presentation, resource use, and 3-month outcome of acute stroke in Europe: data from a multicenter multinational hospital-based registry. Stroke. (2003) 34:1114–9. doi: 10.1161/01.STR.0000068410.07397.D7
7. Roquer J, Campello AR, Gomis M. Sex differences in first-ever acute stroke. Stroke. (2003) 34:1581–5. doi: 10.1161/01.STR.0000078562.82918.F6
8. Strong B, Lisabeth LD, Reeves M. Sex differences in IV thrombolysis treatment for acute ischemic stroke: a systematic review and meta-analysis. Neurology. (2020) 95:e11–22. doi: 10.1212/WNL.0000000000009733
9. O'Neill ZR, Deptuck HM, Quong L, Maclean G, Villaluna K, King-Azote P, et al. Who says “no” to participating in stroke clinical trials and why: an observational study from the Vancouver Stroke Program. Trials. (2019) 20:1–6. doi: 10.1186/s13063-019-3434-0
10. Rochon PA, Mason R, Gurwitz JH. Increasing the visibility of older women in clinical research. Lancet. (2020) 395:1530–2. doi: 10.1016/S0140-6736(20)30849-7
11. Madsen TE, Guo D. Sex differences in modifiable stroke risk factors: the next step in personalized stroke prevention. (2020). doi: 10.1212/WNL.0000000000010983
12. Jiménez-Sanchez L, Hamilton OK, Clancy U, Backhouse EV, Stewart CR, Stringer MS, et al. Sex differences in Cerebral Small Vessel Disease: a systematic review and meta-analysis. medRxiv. (2021). doi: 10.1101/2021.03.04.21252853
13. Backhouse EV, McHutchison CA, Cvoro V, Shenkin SD, Wardlaw JM. Early life risk factors for cerebrovascular disease: a systematic review and meta-analysis. Neurology. (2017) 88:976–84. doi: 10.1212/WNL.0000000000003687
14. Hamilton OK, Backhouse EV, Janssen E, Jochems AC, Maher C, Ritakari TE, et al. Cognitive impairment in sporadic cerebral small vessel disease: a systematic review and meta-analysis. Alzheimer's Dementia. (2021) 17:665–85. doi: 10.1002/alz.12221
15. Clancy U, Gilmartin D, Jochems AC, Knox L, Doubal FN, Wardlaw JM. Neuropsychiatric symptoms associated with cerebral small vessel disease: a systematic review and meta-analysis. Lancet Psychiatry. (2021) 2021:4. doi: 10.1016/S2215-0366(20)30431-4
16. Stewart CR, Stringer MS, Shi Y, Thrippleton MJ, Wardlaw JM. Associations between white matter hyperintensity burden, cerebral blood flow and transit time in small vessel disease: an updated meta-analysis. Front Neurol. (2021) 12:621. doi: 10.3389/fneur.2021.647848
17. Macleod MR, Michie S, Roberts I, Dirnagl U, Chalmers I, Ioannidis JP, et al. Biomedical research: increasing value, reducing waste. Lancet. (2014) 383:101–4. doi: 10.1016/S0140-6736(13)62329-6
18. Guyatt GH, Oxman AD, Schünemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. (2011) 64:380–2. doi: 10.1016/j.jclinepi.2010.09.011
19. Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. (2013) 12:822–38. doi: 10.1016/S1474-4422(13)70124-8
20. Staals J, Makin SD, Doubal FN, Dennis MS, Wardlaw JM. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology. (2014) 83:1228–34. doi: 10.1212/WNL.0000000000000837
21. R Core Team. R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing (2020).
22. United Nations, Economic Do, Social Affairs. World Population Prospects: The 2017 Revision, Key Findings and Advance Tables. New York, NY (2017).
23. Higgins J. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1. 0 [updated March 2011]. The Cochrane Collaboration. (2011). Available online at: www.cochrane-handbook.org (accessed September 28, 2021).
24. Kim C-M, Alvarado RL, Stephens K, Wey H-Y, Wang DJ, Leritz EC, et al. Associations between cerebral blood flow and structural and functional brain imaging measures in individuals with neuropsychologically defined mild cognitive impairment. Neurobiol Aging. (2020) 86:64–74. doi: 10.1016/j.neurobiolaging.2019.10.023
25. Cedres N, Machado A, Molina Y, Diaz-Galvan P, Hernández-Cabrera JA, Barroso J, et al. Subjective cognitive decline below and above the age of 60: a multivariate study on neuroimaging, cognitive, clinical, and demographic measures. J Alzheimer's Dis. (2019) 68:295–309. doi: 10.3233/JAD-180720
26. Dolui S, Tisdall D, Vidorreta M, Jacobs Jr DR, Nasrallah IM, Bryan RN, et al. Characterizing a perfusion-based periventricular small vessel region of interest. NeuroImage Clin. (2019) 23:101897. doi: 10.1016/j.nicl.2019.101897
27. Legdeur N, Visser PJ, Woodworth DC, Muller M, Fletcher E, Maillard P, et al. White matter hyperintensities and hippocampal atrophy in relation to cognition: the 90+ study. J Am Geriatr Soc. (2019) 67:1827–34. doi: 10.1111/jgs.15990
28. Mishra A, Chauhan G, Violleau M-H, Vojinovic D, Jian X, Bis JC, et al. Association of variants in HTRA1 and NOTCH3 with MRI-defined extremes of cerebral small vessel disease in older subjects. Brain. (2019) 142:1009–23. doi: 10.1093/brain/awz024
29. Puzo C, Labriola C, Sugarman MA, Tripodis Y, Martin B, Palmisano JN, et al. Independent effects of white matter hyperintensities on cognitive, neuropsychiatric, and functional decline: a longitudinal investigation using the National Alzheimer's Coordinating Center Uniform Data Set. Alzheimer's Res Ther. (2019) 11:1–13. doi: 10.1186/s13195-019-0521-0
30. Staffaroni AM, Cobigo Y, Elahi FM, Casaletto KB, Walters SM, Wolf A, et al. A longitudinal characterization of perfusion in the aging brain and associations with cognition and neural structure. Hum Brain Mapp. (2019) 40:3522–33. doi: 10.1002/hbm.24613
31. Tsapanou A, Habeck C, Gazes Y, Razlighi Q, Sakhardande J, Stern Y, et al. Brain biomarkers and cognition across adulthood. Hum Brain Mapp. (2019) 40:3832–42. doi: 10.1002/hbm.24634
32. Yao H, Mizoguchi Y, Monji A, Yakushiji Y, Takashima Y, Uchino A, et al. Low-grade inflammation is associated with apathy indirectly via deep white matter lesions in community-dwelling older adults: the Sefuri study. Int J Mol Sci. (2019) 20:1905. doi: 10.3390/ijms20081905
33. Croall ID, Tozer DJ, Moynihan B, Khan U, O'Brien JT, Morris RG, et al. Effect of standard vs. intensive blood pressure control on cerebral blood flow in small vessel disease: the preserve randomized clinical trial. J Am Med Assoc Neurol. (2018) 75:720–7. doi: 10.1001/jamaneurol.2017.5153
34. Kuriyama N, Ozaki E, Mizuno T, Ihara M, Mizuno S, Koyama T, et al. Association between α-Klotho and deep white matter lesions in the brain: a pilot case control study using brain MRI. J Alzheimer's Dis. (2018) 61:145–55. doi: 10.3233/JAD-170466
35. Puglisi V, Bramanti A, Lanza G, Cantone M, Vinciguerra L, Pennisi M, et al. Impaired cerebral haemodynamics in vascular depression: insights from transcranial doppler ultrasonography. Front Psychiatry. (2018) 9:316. doi: 10.3389/fpsyt.2018.00316
36. Shokouhi M, Qiu D, Samman Tahhan A, Quyyumi AA, Hajjar I. Differential associations of diastolic and systolic pressures with cerebral measures in older individuals with mild cognitive impairment. Am J Hypertens. (2018) 31:1268–77. doi: 10.1093/ajh/hpy104
37. Van Rooden S, van den Berg-Huysmans AA, Croll PH, Labadie G, Hayes JM, Viviano R, et al. Subjective cognitive decline is associated with greater white matter hyperintensity volume. J Alzheimer's Dis. (2018) 66:1283–94. doi: 10.3233/JAD-180285
38. Bahrani AA, Powell DK Yu G, Johnson ES, Jicha GA, Smith CD. White matter hyperintensity associations with cerebral blood flow in elderly subjects stratified by cerebrovascular risk. J Stroke Cerebrovasc Dis. (2017) 26:779–86. doi: 10.1016/j.jstrokecerebrovasdis.2016.10.017
39. Squarzoni P, Tamashiro-Duran JH, Duran FL, Leite CC, Wajngarten M, Scazufca M, et al. High frequency of silent brain infarcts associated with cognitive deficits in an economically disadvantaged population. Clinics. (2017) 72:474–80. doi: 10.6061/clinics/2017(08)04
40. Shi L, Miao X, Lou W, Liu K, Abrigo J, Wong A, et al. The spatial associations of cerebral blood flow and spontaneous brain activities with White matter Hyperintensities—an exploratory study using multimodal magnetic resonance imaging. Front Neurol. (2017) 8:593. doi: 10.3389/fneur.2017.00593
41. Xu X, Chan QL, Hilal S, Goh WK, Ikram MK, Wong TY, et al. Cerebral microbleeds and neuropsychiatric symptoms in an elderly Asian cohort. J Neurol Neurosurg Psychiatry. (2017) 88:7–11. doi: 10.1136/jnnp-2016-313271
42. Chung C-P, Chou K-H, Chen W-T, Liu L-K, Lee W-J, Chen L-K, et al. Cerebral microbleeds are associated with physical frailty: a community-based study. Neurobiol Aging. (2016) 44:143–50. doi: 10.1016/j.neurobiolaging.2016.04.025
43. Promjunyakul N-o, Lahna DL, Kaye JA, Dodge HH, Erten-Lyons D, Rooney WD, et al. Comparison of cerebral blood flow and structural penumbras in relation to white matter hyperintensities: a multi-modal magnetic resonance imaging study. J Cerebr Blood Flow Metabol. (2016) 36:1528–36. doi: 10.1177/0271678X16651268
44. Vemuri P, Lesnick TG, Przybelski SA, Knopman DS, Preboske GM, Kantarci K, et al. Vascular and amyloid pathologies are independent predictors of cognitive decline in normal elderly. Brain. (2015) 138:761–71. doi: 10.1093/brain/awu393
45. Yamawaki M, Wada-Isoe K, Yamamoto M, Nakashita S, Uemura Y, Takahashi Y, et al. Association of cerebral white matter lesions with cognitive function and mood in Japanese elderly people: a population-based study. Brain Behav. (2015) 5:e00315. doi: 10.1002/brb3.315
46. Annweiler C, Annweiler T, Bartha R, Herrmann F, Camicioli R, Beauchet O. Vitamin D and white matter abnormalities in older adults: a cross-sectional neuroimaging study. Eur J Neurol. (2014) 21:1436–e95. doi: 10.1111/ene.12511
47. Mortamais M, Portet F, Brickman AM, Provenzano FA, Muraskin J, Akbaraly TN, et al. Education modulates the impact of white matter lesions on the risk of mild cognitive impairment and dementia. Am J Geriatr Psychiatry. (2014) 22:1336–45. doi: 10.1016/j.jagp.2013.06.002
48. Sarabia-Cobo CM, Pérez V, Hermosilla C, Nuñez MJ, de Lorena P. Apathy and leukoaraiosis in mild cognitive impairment and Alzheimer's disease: multicenter diagnostic criteria according to the latest studies. Dement Geriatr Cogn Dis Extra. (2014) 4:228–35. doi: 10.1159/000363227
49. Sims R, Katzel L, Lefkowitz D, Siegel E, Rosenberger W, Manukyan Z, et al. Association of fasting glucose with subclinical cerebrovascular disease in older adults without Type 2 diabetes. Diabetic medicine. (2014) 31:691–8. doi: 10.1111/dme.12385
50. Sun X, Liang Y, Wang J, Chen K, Chen Y, Zhou X, et al. Early frontal structural and functional changes in mild white matter lesions relevant to cognitive decline. J Alzheimer's Dis. (2014) 40:123–34. doi: 10.3233/JAD-131709
51. Wiegman AF, Meier IB, Schupf N, Manly JJ, Guzman VA, Narkhede A, et al. Cerebral microbleeds in a multiethnic elderly community: demographic and clinical correlates. J Neurol Sci. (2014) 345:125–30. doi: 10.1016/j.jns.2014.07.024
52. Farfel JM, Nitrini R, Suemoto CK, Grinberg LT, Ferretti REL, Leite REP, et al. Very low levels of education and cognitive reserve: a clinicopathologic study. Neurology. (2013) 81:650–7. doi: 10.1212/WNL.0b013e3182a08f1b
53. Minn Y-K, Suk S-H, Park H, Cheong J-S, Yang H, Lee S, et al. Tooth loss is associated with brain white matter change and silent infarction among adults without dementia and stroke. J Korean Med Sci. (2013) 28:929–33. doi: 10.3346/jkms.2013.28.6.929
54. Nebes RD, Snitz BE, Cohen AD, Aizenstein HJ, Saxton JA, Halligan EM, et al. Cognitive aging in persons with minimal amyloid-β and white matter hyperintensities. Neuropsychologia. (2013) 51:2202–9. doi: 10.1016/j.neuropsychologia.2013.07.017
55. Hernández MdCV, Booth T, Murray C, Gow AJ, Penke L, Morris Z, et al. Brain white matter damage in aging and cognitive ability in youth and older age. Neurobiol Aging. (2013) 34:2740–7. doi: 10.1016/j.neurobiolaging.2013.05.032
56. Bartley M, Bokde A, Ewers M, Faluyi Y, Tobin W, Snow A, et al. Subjective memory complaints in community dwelling healthy older people: the influence of brain and psychopathology. Int J Geriatr Psychiatry. (2012) 27:836–43. doi: 10.1002/gps.2794
57. Salarirad S, Staff RT, Fox HC, Deary IJ, Whalley L, Murray AD. Childhood intelligence and brain white matter hyperintensities predict fluid intelligence age 78–81 years: a 1921 Aberdeen birth cohort study. Age Ageing. (2011) 40:562–7. doi: 10.1093/ageing/afr065
58. Stewart R, Godin O, Crivello F, Maillard P, Mazoyer B, Tzourio C, et al. Longitudinal neuroimaging correlates of subjective memory impairment: 4-year prospective community study. Br J Psychiatry. (2011) 198:199–205. doi: 10.1192/bjp.bp.110.078683
59. Villeneuve S, Massoud F, Bocti C, Gauthier S, Belleville S. The nature of episodic memory deficits in MCI with and without vascular burden. Neuropsychologia. (2011) 49:3027–35. doi: 10.1016/j.neuropsychologia.2011.07.001
60. Qiu C, Cotch M, Sigurdsson S, Jonsson P, Jonsdottir M, Sveinbjrnsdottir S, et al. Cerebral microbleeds, retinopathy, and dementia: the AGES-Reykjavik Study. Neurology. (2010) 75:2221–8. doi: 10.1212/WNL.0b013e3182020349
61. Godin O, Maillard P, Crivello F, Alpérovitch A, Mazoyer B, Tzourio C, et al. Association of white-matter lesions with brain atrophy markers: the three-city Dijon MRI study. Cerebrovasc Dis. (2009) 28:177–84. doi: 10.1159/000226117
62. Anderson JF, Saling MM, Srikanth VK, Thrift AG, Donnan GA. Individuals with first-ever clinical presentation of a lacunar infarction syndrome: is there an increased likelihood of developing mild cognitive impairment in the first 12 months after stroke? J Neuropsychol. (2008) 2:373–85. doi: 10.1348/174866408X288846
63. Miranda B, Madureira S, Verdelho A, Ferro J, Pantoni L, Salvadori E, et al. Self-perceived memory impairment and cognitive performance in an elderly independent population with age-related white matter changes. J Neurol Neurosurg Psychiatry. (2008) 79:869–73. doi: 10.1136/jnnp.2007.131078
64. Christensen H, Anstey KJ, Parslow RA, Maller J, Mackinnon A, Sachdev P. The brain reserve hypothesis, brain atrophy and aging. Gerontology. (2007) 53:82–95. doi: 10.1159/000096482
65. Schretlen D, Inscore A, Vannorsdall T, Kraut M, Pearlson G, Gordon B, et al. Serum uric acid and brain ischemia in normal elderly adults. Neurology. (2007) 69:1418–23. doi: 10.1212/01.wnl.0000277468.10236.f1
66. Au R, Massaro JM, Wolf PA, Young ME, Beiser A, Seshadri S, et al. Association of white matter hyperintensity volume with decreased cognitive functioning: the Framingham Heart Study. Arch Neurol. (2006) 63:246–50. doi: 10.1001/archneur.63.2.246
67. Elkins J, Longstreth W, Manolio T, Newman A, Bhadelia R, Johnston S. Education and the cognitive decline associated with MRI-defined brain infarct. Neurology. (2006) 67:435–40. doi: 10.1212/01.wnl.0000228246.89109.98
68. Wright CB, Paik MC, Brown TR, Stabler SP, Allen RH, Sacco RL, et al. Total homocysteine is associated with white matter hyperintensity volume: the Northern Manhattan Study. Stroke. (2005) 36:1207–11. doi: 10.1161/01.STR.0000165923.02318.22
69. Deary IJ, Leaper SA, Murray AD, Staff RT, Whalley LJ. Cerebral white matter abnormalities and lifetime cognitive change: a 67-year follow-up of the Scottish Mental Survey of 1932. Psychol Aging. (2003) 18:140. doi: 10.1037/0882-7974.18.1.140
70. Dufouil C, Alperovitch A, Tzourio C. Influence of education on the relationship between white matter lesions and cognition. Neurology. (2003) 60:831–6. doi: 10.1212/01.WNL.0000049456.33231.96
71. Tsukishima E, Saito H, Shido K, Kobashi G, Ying-Yan G, Kishi R, et al. Long-term blood pressure variability and cerebrovascular changes on ct in a community-based elderly population. J Epidemiol. (2001) 11:190–8. doi: 10.2188/jea.11.190
72. de Groot JC, de Leeuw F-E, Oudkerk M, Hofman A, Jolles J, Breteler MM. Cerebral white matter lesions and depressive symptoms in elderly adults. Arch Gen Psychiatry. (2000) 57:1071–6. doi: 10.1001/archpsyc.57.11.1071
73. Liao D, Cooper L, Cai J, Toole J, Bryan N, Burke G, et al. The prevalence and severity of white matter lesions, their relationship with age, ethnicity, gender, and cardiovascular disease risk factors: the ARIC Study. Neuroepidemiology. (1997) 16:149–62. doi: 10.1159/000368814
74. Boone KB, Miller BL, Lesser IM, Mehringer CM, Hill-Gutierrez E, Goldberg MA, et al. Neuropsychological correlates of white-matter lesions in healthy elderly subjects: a threshold effect. Arch Neurol. (1992) 49:549–54. doi: 10.1001/archneur.1992.00530290141024
75. Tupler LA, Coffey CE, Logue PE, Djang WT, Fagan SM. Neuropsychological importance of subcortical white matter hyperintensity. Arch Neurol. (1992) 49:1248–52. doi: 10.1001/archneur.1992.00530360046016
76. Rao SM, Mittenberg W, Bernardin L, Haughton V, Leo GJ. Neuropsychological test findings in subjects with leukoaraiosis. Arch Neurol. (1989) 46:40–4. doi: 10.1001/archneur.1989.00520370042017
77. Jin H, Ding Z, Lian S, Zhao Y, He S, Zhou L, et al. Prevalence and risk factors of white matter lesions in Tibetan patients without acute stroke. Stroke. (2020) 51:149–53. doi: 10.1161/STROKEAHA.119.027115
78. Zhou Y-N, Gao H-Y, Zhao F-F, Liang Y-C, Gao Y, Liu X-H, et al. The study on analysis of risk factors for severity of white matter lesions and its correlation with cerebral microbleeds in the elderly with lacunar infarction. Medicine. (2020) 99:18865. doi: 10.1097/MD.0000000000018865
79. Jokumsen-Cabral A, Aires A, Ferreira S, Azevedo E, Castro P. Primary involvement of neurovascular coupling in cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy. J Neurol. (2019) 266:1782–8. doi: 10.1007/s00415-019-09331-y
80. Kate M, Gioia L, Jeerakathil T, Hill MD, Gould B, McCourt R, et al. Aggressive blood pressure reduction is not associated with decreased perfusion in leukoaraiosis regions in acute intracerebral hemorrhage patients. PLoS ONE. (2019) 14:e0213645. doi: 10.1371/journal.pone.0213645
81. Liang Y, Chen Y-K, Liu Y-L, Mok VC, Ungvari GS, Chu WC, et al. Exploring causal pathways linking cerebral small vessel diseases burden to poststroke depressive symptoms with structural equation model analysis. J Affect Disord. (2019) 253:218–23. doi: 10.1016/j.jad.2019.04.092
82. Liang C, Zhang J, Liu H, Ma J, An Z, Xia W, et al. Association of COL4A2 gene polymorphisms with lacunar stroke in Xinjiang Han populations. J Mol Neurosci. (2019) 69:133–9. doi: 10.1007/s12031-019-01342-8
83. Ling Y, De Guio F, Jouvent E, Duering M, Hervé D, Guichard JP, et al. Clinical correlates of longitudinal MRI changes in CADASIL. J Cerebral Blood Flow Metabol. (2019) 39:1299–305. doi: 10.1177/0271678X18757875
84. Liu X, Chen L, Cheng R, Luo T, Lv F, Fang W, et al. Altered functional connectivity in patients with subcortical ischemic vascular disease: a resting-state fMRI study. Brain Res. (2019) 1715:126–33. doi: 10.1016/j.brainres.2019.03.022
85. Liu G, Tan X, Dang C, Tan S, Xing S, Huang N, et al. Regional shape abnormalities in thalamus and verbal memory impairment after subcortical infarction. Neurorehabil Neural Repair. (2019) 33:476–85. doi: 10.1177/1545968319846121
86. Liu R, Wu W, Ye Q, Gu Y, Zou J, Chen X, et al. Distinctive and pervasive alterations of functional brain networks in cerebral small vessel disease with and without cognitive impairment. Dement Geriatr Cogn Disord. (2019) 47:55–67. doi: 10.1159/000496455
87. Manso-Calderón R, Cacabelos-Pérez P, Sevillano-García MD, Herrero-Prieto ME, González-Sarmiento R. The impact of vascular burden on behavioural and psychological symptoms in older adults with dementia: the BEVASDE study. Neurol Sci. (2020) 41:165–74. doi: 10.1007/s10072-019-04071-3
88. Oudeman EA, Greving JP, Van den Berg-Vos RM, Biessels GJ, Bron EE, van Oostenbrugge R, et al. Nonfocal transient neurological attacks are associated with cerebral small vessel disease. Stroke. (2019) 50:3540–4. doi: 10.1161/STROKEAHA.119.025328
89. Reginold W, Sam K, Poublanc J, Fisher J, Crawley A, Mikulis DJ. The efficiency of the brain connectome is associated with cerebrovascular reactivity in persons with white matter hyperintensities. Hum Brain Mapp. (2019) 40:3647–56. doi: 10.1002/hbm.24622
90. Rudilosso S, Laredo C, Mancosu M, Moya-Planas N, Zhao Y, Chirife O, et al. Cerebral perfusion and compensatory blood supply in patients with recent small subcortical infarcts. J Cerebral Blood Flow Metabol. (2019) 39:1326–35. doi: 10.1177/0271678X18758548
91. Staszewski J, Skrobowska E, Piusińska-Macoch R, Brodacki B, Stepień A. IL-1α and IL-6 predict vascular events or death in patients with cerebral small vessel disease—Data from the SHEF-CSVD study. Adv Med Sci. (2019) 64:258–66. doi: 10.1016/j.advms.2019.02.003
92. Tsai H-H, Pasi M, Tsai L-K, Chen Y-F, Chen Y-W, Tang S-C, et al. Superficial cerebellar microbleeds and cerebral amyloid angiopathy: a magnetic resonance imaging/positron emission tomography study. Stroke. (2020) 51:202–8. doi: 10.1161/STROKEAHA.119.026235
93. Wu X, Ge X, Du J, Wang Y, Sun Y, Han X, et al. Characterizing the penumbras of white matter hyperintensities and their associations with cognitive function in patients with subcortical vascular mild cognitive impairment. Front Neurol. (2019) 10:348. doi: 10.3389/fneur.2019.00348
94. Yu D, Hennebelle M, Sahlas DJ, Ramirez J, Gao F, Masellis M, et al. Soluble epoxide hydrolase-derived linoleic acid oxylipins in serum are associated with periventricular white matter hyperintensities and vascular cognitive impairment. Transl Stroke Res. (2019) 10:522–33. doi: 10.1007/s12975-018-0672-5
95. Zhang L, Sun W-h, Xing M, Wang Y, Zhang Y, Sun Q, et al. Medial temporal lobe atrophy is related to learning strategy changes in amnestic mild cognitive impairment. J Int Neuropsychol Soc. (2019) 25:706–17. doi: 10.1017/S1355617719000353
96. Ishibashi M, Kimura N, Aso Y, Matsubara E. Effects of white matter lesions on brain perfusion in patients with mild cognitive impairment. Clin Neurol Neurosurg. (2018) 168:7–11. doi: 10.1016/j.clineuro.2018.02.030
97. Kim HJ, Park S, Cho H, Jang YK, San Lee J, Jang H, et al. Assessment of extent and role of tau in subcortical vascular cognitive impairment using 18F-AV1451 positron emission tomography imaging. J Am Med Assoc Neurol. (2018) 75:999–1007. doi: 10.1001/jamaneurol.2018.0975
98. Lisiecka-Ford DM, Tozer DJ, Morris RG, Lawrence AJ, Barrick TR, Markus HS. Involvement of the reward network is associated with apathy in cerebral small vessel disease. J Affect Disord. (2018) 232:116–21. doi: 10.1016/j.jad.2018.02.006
99. Anor CJ, O'Connor S, Saund A, Tang-Wai DF, Keren R, Tartaglia MC. Neuropsychiatric symptoms in Alzheimer disease, vascular dementia, and mixed dementia. Neurodegener Dis. (2017) 17:127–34. doi: 10.1159/000455127
100. Yuan J-L, Wang S-K, Guo X-J, Teng L-l, Jiang H, Gu H, et al. Disconnections of cortico-subcortical pathways related to cognitive impairment in patients with leukoaraiosis: a preliminary diffusion tensor imaging study. Eur Neurol. (2017) 78:41–7. doi: 10.1159/000477899
101. Zhong G, Zhang R, Jiaerken Y, Yu X, Zhou Y, Liu C, et al. Better correlation of cognitive function to white matter integrity than to blood supply in subjects with leukoaraiosis. Front Aging Neurosci. (2017) 9:185. doi: 10.3389/fnagi.2017.00185
102. Bella R, Cantone M, Lanza G, Ferri R, Vinciguerra L, Puglisi V, et al. Cholinergic circuitry functioning in patients with vascular cognitive impairment–no dementia. Brain Stimul. (2016) 9:225–33. doi: 10.1016/j.brs.2015.09.013
103. Hashimoto T, Yokota C, Koshino K, Shimomura R, Hino T, Moriguchi T, et al. Cerebral blood flow and metabolism associated with cerebral microbleeds in small vessel disease. Ann Nucl Med. (2016) 30:494–500. doi: 10.1007/s12149-016-1086-7
104. Hsu Y-H, Huang C-F, Lo C-P, Wang T-L, Yang C-C, Tu M-C. Frontal assessment battery as a useful tool to differentiate mild cognitive impairment due to subcortical ischemic vascular disease from Alzheimer disease. Dement Geriatr Cogn Disord. (2016) 42:331–41. doi: 10.1159/000452762
105. Turk M, Zaletel M, Oblak JP. Characteristics of cerebral hemodynamics in patients with ischemic leukoaraiosis and new ultrasound indices of ischemic leukoaraiosis. J Stroke Cerebrovasc Dis. (2016) 25:977–84. doi: 10.1016/j.jstrokecerebrovasdis.2015.12.045
106. Brookes RL, Hollocks MJ, Khan U, Morris RG, Markus HS. The Brief Memory and Executive Test (BMET) for detecting vascular cognitive impairment in small vessel disease: a validation study. BMC Med. (2015) 13:1–8. doi: 10.1186/s12916-015-0290-y
107. Hsu J-L, Lee W-J, Liao Y-C, Lirng J-F, Wang S-J, Fuh J-L. Posterior atrophy and medial temporal atrophy scores are associated with different symptoms in patients with Alzheimer's disease and mild cognitive impairment. PLoS ONE. (2015) 10:e0137121. doi: 10.1371/journal.pone.0137121
108. Brookes RL, Herbert V, Paul S, Hannesdottir K, Markus HS, Morris RG. Executive dysfunction, awareness deficits and quality of life in patients with cerebral small vessel disease: a structural equation model. Neuropsychology. (2014) 28:247. doi: 10.1037/neu0000015
109. Delrieu J, Desmidt T, Camus V, Sourdet S, Boutoleau-Bretonnière C, Mullin E, et al. Apathy as a feature of prodromal Alzheimer's disease: an FDG-PET ADNI study. Int J Geriatr Psychiatry. (2015) 30:470–7. doi: 10.1002/gps.4161
110. Ledesma-Amaya LI, Salvador-Cruz J, Rodríguez-Agudelo Y, Valencia-Flores M, Arauz A. Alteraciones neuropsicológicas asociadas en pacientes con infarto lacunar. Acta Colombiana de Psicología. (2014) 17:43–52. doi: 10.14718/ACP.2014.17.2.5
111. Pinkhardt EH, Issa H, Gorges M, Jürgens R, Lulé D, Heimrath J, et al. Do eye movement impairments in patients with small vessel cerebrovascular disease depend on lesion load or on cognitive deficits? A video-oculographic and MRI study. J Neurol. (2014) 261:791–803. doi: 10.1007/s00415-014-7275-1
112. Zi W, Duan D, Zheng J. Cognitive impairments associated with periventricular white matter hyperintensities are mediated by cortical atrophy. Acta Neurol Scand. (2014) 130:178–87. doi: 10.1111/ane.12262
113. Deguchi K, Kono S, Deguchi S, Morimoto N, Kurata T, Ikeda Y, et al. novel useful tool of computerized touch panel–type screening test for evaluating cognitive function of chronic ischemic stroke patients. J Stroke Cerebrovasc Dis. (2013) 22:e197–206. doi: 10.1016/j.jstrokecerebrovasdis.2012.11.011
114. Fang M, Feng C, Xu Y, Hua T, Jin A-P, Liu X-Y. Microbleeds and silent brain infarctions are differently associated with cognitive dysfunction in patients with advanced periventricular leukoaraiosis. Int J Med Sci. (2013) 10:1307. doi: 10.7150/ijms.6430
115. Kim HJ, Kang SJ, Kim C, Kim GH, Jeon S, Lee JM, et al. The effects of small vessel disease and amyloid burden on neuropsychiatric symptoms: a study among patients with subcortical vascular cognitive impairments. Neurobiol Aging. (2013) 34:1913–20. doi: 10.1016/j.neurobiolaging.2013.01.002
116. Narasimhalu K, Wiryasaputra L, Sitoh YY, Kandiah N. Post-stroke subjective cognitive impairment is associated with acute lacunar infarcts in the basal ganglia. Eur J Neurol. (2013) 20:547–51. doi: 10.1111/ene.12032
117. Sudo FK, Alves CEO, Alves GS, Ericeira-Valente L, Tiel C, Moreira DM, et al. White matter hyperintensities, executive function and global cognitive performance in vascular mild cognitive impairment. Arq Neuropsiquiatr. (2013) 71:431–6. doi: 10.1590/0004-282X20130057
118. van Norden AG, van Uden IW, de Laat KF, Gons RA, Kessels RP, van Dijk EJ, et al. Cerebral microbleeds are related to subjective cognitive failures: the RUN DMC study. Neurobiol Aging. (2013) 34:2225–30. doi: 10.1016/j.neurobiolaging.2013.03.021
119. Li C, Ling X, Liu S, Xu A, Zhang Y, Xing S, et al. Abnormalities of magnetic resonance spectroscopy and diffusion tensor imaging are correlated with executive dysfunction in patients with ischemic leukoaraiosis. J Clin Neurosci. (2012) 19:718–22. doi: 10.1016/j.jocn.2011.07.052
120. Quinque EM, Arélin K, Dukart J, Roggenhofer E, Streitbuerger D-P, Villringer A, et al. Identifying the neural correlates of executive functions in early cerebral microangiopathy: a combined VBM and DTI study. J Cerebral Blood Flow Metabol. (2012) 32:1869–78. doi: 10.1038/jcbfm.2012.96
121. Yi L, Wang J, Jia L, Zhao Z, Lu J, Li K, et al. Structural and functional changes in subcortical vascular mild cognitive impairment: a combined voxel-based morphometry and resting-state fMRI study. PLoS ONE. (2012) 7:e44758. doi: 10.1371/journal.pone.0044758
122. Fernández PJ, Campoy G, Santos JMG, Antequera MM, García-Sevilla J, Castillo A, et al. Is there a specific pattern of attention deficit in mild cognitive impairment with subcortical vascular features? Evid Attent Netw Test Dementia Geriatr Cogn Disord. (2011) 31:268–75. doi: 10.1159/000327165
123. Xiong YY, Wong A, Mok VC, Tang WK, Lam WW, Kwok TC, et al. Frequency and predictors of proxy-confirmed post-stroke cognitive complaints in lacunar stroke patients without major depression. Int J Geriatr Psychiatry. (2011) 26:1144–51. doi: 10.1002/gps.2652
124. Hassan MA, Helmy SM, Rabah AM, Ameen AI, Helmy H. Assessment of patients with lacunar infarction: a magnetic resonance spectroscopic and psychometric study. Egypt J Neurol Psychiatry Neurosurg. (2010) 47:1–10.
125. Pascual B, Prieto E, Arbizu J, Marti-Climent J, Olier J, Masdeu JC. Brain glucose metabolism in vascular white matter disease with dementia: differentiation from Alzheimer disease. Stroke. (2010) 41:2889–93. doi: 10.1161/STROKEAHA.110.591552
126. Seo SW, Ahn J, Yoon U, Im K, Lee JM, Tae Kim S, et al. Cortical thinning in vascular mild cognitive impairment and vascular dementia of subcortical type. J Neuroimaging. (2010) 20:37–45. doi: 10.1111/j.1552-6569.2008.00293.x
127. Staekenborg SS, Su T, van Straaten EC, Lane R, Scheltens P, Barkhof F, et al. Behavioural and psychological symptoms in vascular dementia; differences between small-and large-vessel disease. J Neurol Neurosurg Psychiatry. (2010) 81:547–51. doi: 10.1136/jnnp.2009.187500
128. Price CC, Garrett KD, Jefferson AL, Cosentino S, Tanner JJ, Penney DL, et al. Leukoaraiosis severity and list-learning in dementia. Clin Neuropsychol. (2009) 23:944–61. doi: 10.1080/13854040802681664
129. Zhou A, Jia J. Different cognitive profiles between mild cognitive impairment due to cerebral small vessel disease and mild cognitive impairment of Alzheimer's disease origin. J Int Neuropsychol Soc. (2009) 15:898–905. doi: 10.1017/S1355617709990816
130. Gainotti G, Ferraccioli M, Vita MG, Marra C. Patterns of neuropsychological impairment in MCI patients with small subcortical infarcts or hippocampal atrophy. J Int Neuropsychol Soc. (2008) 14:611–9. doi: 10.1017/S1355617708080831
131. Nordlund A, Rolstad S, Klang O, Lind K, Hansen S, Wallin A. Cognitive profiles of mild cognitive impairment with and without vascular disease. Neuropsychology. (2007) 21:706. doi: 10.1037/0894-4105.21.6.706
132. Nordahl CW, Ranganath C, Yonelinas AP, DeCarli C, Reed BR, Jagust WJ. Different mechanisms of episodic memory failure in mild cognitive impairment. Neuropsychologia. (2005) 43:1688–97. doi: 10.1016/j.neuropsychologia.2005.01.003
133. van Zandvoort MJ, Van der Grond J, Kappelle L, De Haan E. Cognitive deficits and changes in neurometabolites after a lacunar infarct. J Neurol. (2005) 252:183–90. doi: 10.1007/s00415-005-0629-y
134. Garrett KD, Browndyke JN, Whelihan W, Paul RH, DiCarlo M, Moser DJ, et al. The neuropsychological profile of vascular cognitive impairment—no dementia: comparisons to patients at risk for cerebrovascular disease and vascular dementia. Archiv Clin Neuropsychol. (2004) 19:745–57. doi: 10.1016/j.acn.2003.09.008
135. Graham N, Emery T, Hodges J. Distinctive cognitive profiles in Alzheimer's disease and subcortical vascular dementia. J Neurol Neurosurg Psychiatry. (2004) 75:61–71.
136. Van Zandvoort M, De Haan E, Van Gijn J, Kappelle LJ. Cognitive functioning in patients with a small infarct in the brainstem. J Int Neuropsychol Soc. (2003) 9:490–4. doi: 10.1017/S1355617703000146
137. Kramer J, Reed BR, Mungas D, Weiner M, Chui H. Executive dysfunction in subcortical ischaemic vascular disease. J Neurol Neurosurg Psychiatry. (2002) 72:217–20. doi: 10.1136/jnnp.72.2.217
138. Maeshima S, Moriwaki H, Ozaki F, Okita R, Yamaga H, Ueyoshi A. Silent cerebral infarction and cognitive function in middle-aged neurologically healthy subjects. Acta Neurol Scand. (2002) 105:179–84. doi: 10.1034/j.1600-0404.2002.1o068.x
139. Yuspeh RL, Vanderploeg RD, Crowell TA, Mullan M. Differences in executive functioning between Alzheimer's disease and subcortical ischemic vascular dementia. J Clin Exp Neuropsychol. (2002) 24:745–54. doi: 10.1076/jcen.24.6.745.8399
140. Aharon-Peretz J, Kliot D, Tomer R. Behavioral differences between white matter lacunar dementia and Alzheimer's disease: a comparison on the neuropsychiatric inventory. Dement Geriatr Cogn Disord. (2000) 11:294–8. doi: 10.1159/000017252
141. Yamauchi H, Fukuyama H, Shio H. Corpus callosum atrophy in patients with leukoaraiosis may indicate global cognitive impairment. Stroke. (2000) 31:1515–20. doi: 10.1161/01.STR.31.7.1515
142. Binetti G, Padovani A, Magni E, Bianchetti A, Scuratti A, Lenzi G, et al. Delusions and dementia: clinical and CT correlates. Acta Neurol Scand. (1995) 91:271–5. doi: 10.1111/j.1600-0404.1995.tb07003.x
143. Lewine R, Hudgins P, Risch SC, Walker EF. Lowered attention capacity in young, medically healthy men with magnetic resonance brain hyperintensity signals. Neuropsychiatry Neuropsychol Behav Neurol. (1993) 6:38–42.
144. Johansson M, Stomrud E, Lindberg O, Westman E, Johansson PM, van Westen D, et al. Apathy and anxiety are early markers of Alzheimer's disease. Neurobiol Aging. (2020) 85:74–82. doi: 10.1016/j.neurobiolaging.2019.10.008
145. Atwi S, Metcalfe AW, Robertson AD, Rezmovitz J, Anderson ND, MacIntosh BJ. Attention-related brain activation is altered in older adults with white matter hyperintensities using multi-echo fMRI. Front Neurosci. (2018) 12:748. doi: 10.3389/fnins.2018.00748
146. Goncalves C, Pinho MS, Cruz V, Gens H, Oliveira F, Pais J, et al. Portuguese version of Wechsler Memory Scale−3rd edition's utility with demented elderly adults. Appl Neuropsychol Adult. (2017) 24:212–25. doi: 10.1080/23279095.2015.1135440
147. Kim D, Ford G, Kidwell C, Starkman S, Vinuela F, Duckwiler G, et al. Intra-arterial thrombolysis for acute stroke in patients 80 and older: a comparison of results in patients younger than 80 years. Am J Neuroradiol. (2007) 28:159–63.
148. Suri MFK, Qureshi AI. Recruitment of ischemic stroke patients in clinical trials in general practice and implications for generalizability of results. J Vasc Interv Neurol. (2012) 5:27.
149. Berglund A, Schenck-Gustafsson K, von Euler M. Sex differences in the presentation of stroke. Maturitas. (2017) 99:47–50. doi: 10.1016/j.maturitas.2017.02.007
150. Newman-Toker DE, Moy E, Valente E, Coffey R, Hines AL. Missed diagnosis of stroke in the emergency department: a cross-sectional analysis of a large population-based sample. Diagnosis. (2014) 1:155–66. doi: 10.1515/dx-2013-0038
151. Yu AY, Penn AM, Lesperance ML, Croteau NS, Balshaw RF, Votova K, et al. Sex differences in presentation and outcome after an acute transient or minor neurologic event. J Am Med Assoc Neurol. (2019) 76:962–8. doi: 10.1001/jamaneurol.2019.1305
152. Lövheim H, Sandman P-O, Karlsson S, Gustafson Y. Sex differences in the prevalence of behavioral and psychological symptoms of dementia. Int Psychogeriatr. (2009) 21:469–75. doi: 10.1017/S1041610209008497
153. Dahlberg L, Demack S, Bambra C. Age and gender of informal carers: a population-based study in the UK. Health Soc Care Community. (2007) 15:439–45. doi: 10.1111/j.1365-2524.2007.00702.x
154. Gabe J, Monaghan L, Hollinrake S. Key concepts in medical sociology. In: Publishing S, editor, Informal Care. London: SAGE Publications Ltd (2016). 196–200.
155. Verbakel E, Tamlagsrønning S, Winstone L, Fjær EL, Eikemo TA. Informal care in Europe: findings from the European Social Survey (2014) special module on the social determinants of health. Eur J Public Health. (2017) 27(suppl.1):90–5. doi: 10.1093/eurpub/ckw229
156. Chappell NL, Kusch K. The gendered nature of filial piety—a study among Chinese Canadians. J Cross Cult Gerontol. (2007) 22:29–45. doi: 10.1007/s10823-006-9011-5
157. Carcel C, Reeves M. Under-enrollment of women in stroke clinical trials: what are the causes and what should be done about it? Stroke. (2021) 52:452–7. doi: 10.1161/STROKEAHA.120.033227
158. Gunda B, Hervé D, Godin O, Bruno M, Reyes S, Alili N, et al. Effects of gender on the phenotype of CADASIL. Stroke. (2012) 43:137–41. doi: 10.1161/STROKEAHA.111.631028
159. Stanhewicz AE, Wenner MM, Stachenfeld NS. Sex differences in endothelial function important to vascular health and overall cardiovascular disease risk across the lifespan. Am J Physiol Heart Circulat Physiol. (2018) 315:H1569–88. doi: 10.1152/ajpheart.00396.2018
160. Duckles SP, Krause DN. Mechanisms of cerebrovascular protection: oestrogen, inflammation and mitochondria. Acta Physiol. (2011) 203:149–54. doi: 10.1111/j.1748-1716.2010.02184.x
161. World Health Organization. WHO Global Report on Trends in Prevalence of Tobacco Smoking 2000–2025. Geneva: World Health Organization (2018).
162. Zhou B, Bentham J, Di Cesare M, Bixby H, Danaei G, Cowan MJ, et al. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19· 1 million participants. Lancet. (2017) 389:37–55. doi: 10.1016/S0140-6736(16)31919-5
163. Howard VJ, Madsen TE, Kleindorfer DO, Judd SE, Rhodes JD, Soliman EZ, et al. Sex and race differences in the association of incident ischemic stroke with risk factors. J Am Med Assoc Neurol. (2019) 76:179–86. doi: 10.1001/jamaneurol.2018.3862
164. Martin S, Valdés Hernández MdC. Data Extraction and Analysis of the Systematic Search on Gender Differences on Brain MRI Structures and Connectivity: 2000–2017. Edinburgh: University of Edinburgh, Centre for Clinical Brain Sciences, Department of Neuroimaging Sciences (2017).
165. Miles J. The Importance of Sex and Gender Reporting. In Support of the SAGER Guidelines. Amsterdam: Elsevier (2020).
166. Gibney E. The researcher fighting to embed analysis of sex and gender into science. Nature. (2020) 588:209–209. doi: 10.1038/d41586-020-03336-8
167. Heidari S, Babor TF, De Castro P, Tort S, Curno M. Sex and gender equity in research: rationale for the SAGER guidelines and recommended use. Res Integr Peer Rev. (2016) 1:1–9. doi: 10.1186/s41073-016-0007-6
168. Schiebinger L, Klinge I. Gendered Innovations 2: How Inclusive Analysis Contributes to Research and Innovation. Luxembourg: Publications Office of the European Union (2020).
Keywords: cerebral small vessel disease (SVD), sex differences, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), lacunar stroke, vascular dementia (VaD)
Citation: Jiménez-Sánchez L, Hamilton OKL, Clancy U, Backhouse EV, Stewart CR, Stringer MS, Doubal FN and Wardlaw JM (2021) Sex Differences in Cerebral Small Vessel Disease: A Systematic Review and Meta-Analysis. Front. Neurol. 12:756887. doi: 10.3389/fneur.2021.756887
Received: 11 August 2021; Accepted: 04 October 2021;
Published: 28 October 2021.
Edited by:
Christine Kremer, Lund University, SwedenReviewed by:
Francesca Romana Pezzella, San Camillo-Forlanini Hospital, ItalyCheryl Carcel, University of New South Wales, Australia
Copyright © 2021 Jiménez-Sánchez, Hamilton, Clancy, Backhouse, Stewart, Stringer, Doubal and Wardlaw. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joanna M. Wardlaw, joanna.wardlaw@ed.ac.uk