
Abstract
Aim
To evaluate the profile of strabismus that occurs in stroke survivors and determine the relationship between site of stroke and symptom of diplopia.
Methods
Prospective multi-centre cohort trial involving 16 recruiting centres (Vision In Stroke (VIS) Group). Standardised referral and investigation protocol used by local investigators. Each patient underwent assessment of ocular alignment, motility, and binocular vision. Results were evaluated with non-parametric statistical tests.
Results
In all, 512 patients were recruited with a mean age of 69 years: SD 15 over a 2-year period (59% male patients, 41% female patients). Median duration from onset to vision assessment was 19 days (range 0–1140 days). About 19% of the patients had strabismus detected on orthoptic investigation after the onset of stroke. Of these strabismic patients 12.5% had strabismus that pre-existed the onset of stroke (that could be determined from case history). A total of 70% had strabismus associated with ocular motility abnormalities and 30% were in isolation. About 24% were associated with brain stem, cerebellar, thalamus or basal ganglia strokes, and 73% with cortical strokes. Around 36% complained of diplopia and the remainder had no symptoms related to their strabismus.
Conclusions
Strabismus was found to occur in 16.5% of patients after their stroke. Strabismus with diplopia was always associated with other ocular motility abnormalities, whereas strabismus without associated ocular motility abnormalities did not result in the symptom of diplopia.
Similar content being viewed by others

Introduction
The ocular motility consequences of stroke are wide ranging. Recent research has documented a prevalence of 68% of stroke survivors, referred with suspected visual difficulty, as having an ocular motility or ocular alignment impairment.1 Symptoms included diplopia, oscillopsia, reading difficulty, or blurred vision in these patients. Previously Fowler et al2 addressed the prevalence of strabismus and diplopia after brain injury, of which 54% were strokes. They found 26% of their stroke survivors to have a squint. However, they noted that a large proportion of these patients failed to complain of diplopia.
As part of the multi-centre Vision In Stroke (VIS) Study, the results were evaluated to determine the profile of strabismus occurring in our stroke survivors. The purpose was to consider the symptom of diplopia (or lack of) and the relationship between the site of stroke, the occurrence of strabismus, and the presence of symptoms.
Materials and methods
The VIS Study has been described in detail elsewhere.1 The study is a prospective multi-centre observational case cohort study, which conforms to the Tenets of Helsinki with multi-centre ethical approval in the United Kingdom. The VIS Group consists of local investigators responsible for assessing stroke patients and collecting patient data. The data is collated centrally at the University of Liverpool.
The target population is stroke patients suspected of having a visual difficulty. A standardised screening and investigation forms are used in each recruiting centre, which identifies known pre-existent ocular pathology, symptoms and signs, investigation of visual field, ocular motility and perceptual aspects, and stroke demographics.
For this study we addressed the ocular motility and ocular alignment findings. The assessments consisted of cover test at near and distant fixation, qualitative evaluation of saccades, smooth pursuits and vergence eye movements, retinal correspondence (Bagolini glasses), fusional vergence (20 prism diopter (PD) or prism fusion range at near fixation), stereoacuity (Frisby near test), prism cover test, and lid and pupil function.
Statistical analysis was undertaken using the SPSS version 15 software package (SPSS Inc, Chicago, IL, USA) using non-parametric tests.
Results
In all, 512 patients were recruited over a 2-year period. The mean age at stroke onset was 69 years: SD 15 with 59% male patients and 41% female patients. Median duration from onset to vision assessment was 19 days (range 0–1140 days).
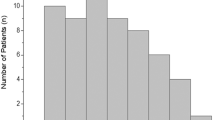
Almost 19% had strabismus detected by cover test (Figure 1). About 73% of these were cortical strokes and 24% included subcortical areas (cerebellar, brainstem, thalamus, or basal ganglia). Around 2.5% were diagnosed as having pre-existent strabismus from their case history. In all 16.5% of the total patients recruited to the study thus, had strabismus due to the stroke. Of these patients 69% included cortical lesion and 31% were subcortical lesions. About 42% were purely cortical (frontal, occipital, parietal or temporal lobes, internal or external capsule, periventricular or intraventricular), 18% were purely subcortical and 40% were multiple areas. Forty-eight percent of patients with strabismus had right-sided stroke, 42% had left-sided stroke and 10% were bilateral.

Types of manifest strabismus.
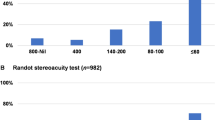
Almost 70% had strabismus associated with ocular motility abnormalities (Figure 2). Around 56.5% had just one ocular motility abnormality, for example internuclear opthalmoplegia (INO); the remainder had a combination of ocular motility abnormalities, for example, vertical gaze palsy with III nerve palsy. Seventy-seven percent had a near point of convergence of less than 8 cms (of which 72% were associated with exotropia) and 24% had nystagmus (gaze evoked, upbeat, congenital, end point, abducting, multivector, convergence retraction, horizontal jerk, latent and pendular).

Ocular motility abnormalities.
In all, 36% complained of diplopia as a primary symptom. A further 16% complained of diplopia in association with other symptoms, including reading difficulty, visual field loss, poor vision, and oscillopsia. All patients complaining of diplopia had associated ocular motility abnormalities. Of these patients, 56% included a cortical lesion and 44% involved sub cortical lesions. Thirty-three percent were purely cortical (occipital, temporal or parietal lobes or internal capsule), 19% were purely sub cortical, and 48% were multiple areas. Forty-two percent had right-sided lesions, 41% had left-sided lesions, and 17% had bilateral lesions.
Low vision of <0.5 best-corrected vision (logMAR) was documented in 24% of patients with strabismus and low vision of 1.0 or worse was documented in 15% of patients. Visual field impairment was documented in 34% of strabismic patients, including 67% with homonymous hemianopia and the remainder relating to quadrantanopia, peripheral loss, altitudinal, and scotomatous loss.
Treatment for strabismic patients was provided in 64%, including the use of prisms, occlusion, spectacle correction, and orthoptic exercises.
Discussion
The reported incidence of ocular motility abnormalities ranges up to 68%1, 3, 4, 5 and for strabismus, ranges up to 26% in stroke survivors.1, 2, 3 In all, 19% of patients in this study had manifest strabismus detected on cover test at their first orthoptic assessment after the onset of stroke. About 2.5% had a history of prior strabismus and thus, the total percentage of patients with strabismus acquired after onset of stroke was 16.5%. The predominant strabismus type noted in our patients was that of exotropia.
Fowler et al2 reported a number of interesting findings. They noted that in some of their cases the deviation was slight or intermittent and might not have been noticed. This was particularly true of divergent strabismus for near targets, which commonly resulted in disabling loss of convergence and stereo-acuity. They reported that left-sided and right-sided hemispheric strokes were equally as likely to cause strabismus, left-sided strokes were more associated with the presence of diplopia, and there was a surprising lack of diplopia with strabismus of recent onset with 36% of patients being asymptomatic.
The most common type of manifest strabismus encountered in this study was exotropia. Almost 77% of our patients had impaired convergence and 72% of these patients had exotropia. We also found that our strabismic patients had similar occurrences of right- or left-sided strokes, and 10% had bilateral lesions. However, we did not find that diplopic patients were more likely to have left-sided strokes. Our diplopic patients were equally as likely to have right- or left-sided strokes, and 17% had bilateral lesions. We confirmed the lack of diplopia with manifest strabismus of recent onset. Around 48% of our patients did not complain of diplopia. About 11% were entirely asymptomatic and other symptoms predominantly related to poor vision, reading difficulty, and visual field loss.
It has been postulated that left-sided neglect may partially explain the lack of diplopia in right hemisphere strokes.2 However, this cannot explain the lack of diplopia for patients without neglect or with left-sided stroke. Poor vision may explain a lack of diplopia in some cases although it is acknowledged that even in very poor acuity, some patients may still complain of diplopia.6 Considerable loss of visual field, such as homonymous hemianopia may also contribute to the non perception of diplopia. It was not possible to predict from the area of brain injury, those patients that complained of diplopia. The only factor that we found to be different between patients with or without the symptom of diplopia was the additional association of an ocular motility abnormality (excluding poor convergence or nystagmus).
Jones and Shinton7 stated that patients may find that their symptoms improve over time with little or no intervention. For those patients that require treatment to alleviate the symptom of diplopia, a number of interventions have been shown to be beneficial, including the use of Fresnel prisms, occlusion, orthoptic exercises, typoscopes, or compensatory head postures.1, 4, 8 In this study, 64% of patients had intervention to aid alleviation of their diplopia. The remaining 36% had targeted advice on how to cope with their symptoms. Intervention included Fresnel prisms to join diplopia, orthoptic exercises, spectacle correction, and occlusion (total or sector as required). Around 29.5% had multiple treatment interventions.
A recommendation has been made previously for the involvement of orthoptists in the stroke team because of the poor understanding of strabismus by many physicians,7 and the orthoptists ability to diagnose and treat patients with diplopia, gaze problems, and nystagmus.4 This recommendation has been further endorsed by recent research on the status of ocular motility and alignment after stroke.1, 9 The results of this study add to the recommendation to include orthoptists in the evaluation of stroke survivors in both acute and neuro rehabilitation services. One-fifth of patients with visual disability after stroke show a manifest strabismus and many of these have associated ocular motility disturbance. However, of those patients with a recent onset strabismus, nearly half do not complain of diplopia and therefore, may be less likely to be detected by clinicians unfamiliar with the assessment of ocular alignment or motility. Orthoptists can accurately detect and diagnose the many types of strabismus that may occur post stroke, and quickly instigate an intervention for those patients who do complain of diplopia.
References
Rowe FJ, VIS group. Visual impairment following stroke. Do stroke patients require vision assessment? Age Ageing 2009; 38: 188–193.
Fowler MS, Wade DT, Richardson AJ, Stein JE . Squints and diplopia seen after brain damage. J Neurol 1996; 243: 86–90.
Clisby C . Visual assessment of patients with cerebrovascular accident on the elderly care wards. Br Orthopt J 1995; 52: 38–40.
MacIntosh C . Stroke re-visited: visual problems following stroke and their effect on rehabilitation. Br Orthopt J 2003; 60: 10–14.
DeLuca M, Spinelli D, Zoccolotti P . Eye movement patterns in reading as a function of visual field defects and contrast sensitivity loss. Cortex 1996; 32: 491–502.
Lam FC, Weir CR, Cleary M . Binocularity and severe uniocular trauma. Strabismus 2008; 16: 71–75.
Jones SA, Shinton RA . Improving outcome in stroke patients with visual problems. Age Ageing 2006; 35: 560–565.
Freeman CF, Rudge NB . Cerebrovascular accident and the Orthoptist. Br Orthopt J 1988; 45: 8–18.
Rowe FJ, VIS group. Visual impairment in stroke survivors: a prospective multi-centre trial. Trans. 31st European Strabismological Association: Mykonos, Greece, 2007; 185–188.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Declaration: This article is based on a study first reported in the Transactions of the 32nd European Strabismological Association, Munich, Germany. 2008, in press
Appendix
Rights and permissions
About this article
Cite this article
Rowe, F., VIS group UK. The profile of strabismus in stroke survivors. Eye 24, 682–685 (2010). https://doi.org/10.1038/eye.2009.138
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2009.138
Keywords
This article is cited by
-
Clinical Practice Guidelines for Occupational Therapists in the Evaluation and Treatment of Oculomotor Impairment Following Traumatic Brain Injury
Current Physical Medicine and Rehabilitation Reports (2021)
-
Update on the Clinical Approach to Spatial Neglect
Current Neurology and Neuroscience Reports (2019)
-
Neurological signs in 23 dogs with suspected rostral cerebellar ischaemic stroke
Acta Veterinaria Scandinavica (2015)
-
Prevalence of ocular motor cranial nerve palsy and associations following stroke
Eye (2011)
