
Abstract
Background
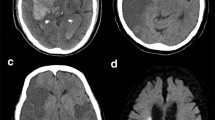
Patients with stroke symptoms but negative diffusion-weighted imaging (DWI) might have transient ischemic attacks (TIA) or stroke mimics. Brain DWI is important for the diagnosis of cerebral infarction but it is not available before thrombolysis for most patients to avoid treatment delay. This study aimed to evaluate the safety of IV thrombolysis in patients with a negative post-treatment DWI for cerebral infarction.
Methods
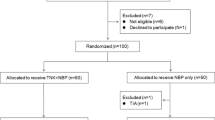
We conducted a retrospective study of 89 patients treated with IV recombinant tissue plasminogen activator (rt-PA) within 4.5 h after stroke symptom onset. The patients were identified in our acute stroke registry from January 2009 to September 2010. Information on patients’ demographics, clinical characteristics, neuroimaging, treatment complications, and outcomes was obtained and analyzed.
Results
Out of 89 patients, 23 patients (26%) had a negative DWI on follow-up stroke imaging. Fourteen patients had a TIA and nine patients had a stroke mimic, including Todd’s paralysis, complicated migraine, and somatoform disorder. We found significant differences between patients with a positive and a negative DWI in mean age (62 years vs. 52 years; P < 0.01) and median admission NIH stroke scale score (11 points versus 6 points; P < 0.001). Among patients with a positive DWI, four patients had a symptomatic intracerebral hemorrhage (ICH). No patients with a negative DWI had symptomatic or asymptomatic ICH.
Conclusions
Our results suggest that the administration of IV rt-PA within the first 4.5 h of symptom onset in patients with suspected ischemic stroke is safe even when post-treatment DWI does not demonstrate cerebral infarction.

Similar content being viewed by others

References
Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375:1695–703.
Schellinger PD, Bryan RN, Caplan LR, et al. Evidence-based guideline: the role of diffusion and perfusion MRI for the diagnosis of acute ischemic stroke: report of the therapeutics and technology assessment subcommittee of the American Academy of Neurology. Neurology. 2010;75:177–85.
Oppenheim C, Stanescu R, Dormont D, et al. False-negative diffusion-weighted MR findings in acute ischemic stroke. Am J Neuroradiol. 2000;21:1434–40.
Huff JS. Stroke mimics and chameleons. Emerg Med Clin North Am. 2002;20:583–95.
Yew KS, Cheng E. Acute stroke diagnosis. Am Fam Physician. 2009;80:33–40.
Chernyshev OY, Martin-Schild S, Albright KC, et al. Safety of tPA in stroke mimics and neuroimaging-negative cerebral ischemia. Neurology. 2010;74:1340–5.
Winkler DT, Fluri F, Fuhr P, et al. Thrombolysis in stroke mimics: frequency, clinical characteristics, and outcome. Stroke. 2009;40:1522–5.
Uchino K, Massaro L, Hammer MD. Transient ischemic attack after tissue plasminogen activator: aborted stroke or unnecessary stroke therapy? Cerebrovasc Dis. 2010;29:57–61.
Caplan L, Mohr J, Kistler J, Koroshetz W. Should thrombolytic therapy be the first-line treatment for acute ischemic stroke? Thrombolysis—not a panacea for ischemic stroke. N Engl J Med. 1997;337:1309–10.
Scott PA, Silbergleit R. Misdiagnosis of stroke in tissue plasminogen activator-treated patients: characteristics and outcomes. Ann Emerg Med. 2003;42:611–8.
Vroomen P, Buddingh M, Luijckx G, et al. The incidence of stroke mimics among stroke department admissions in relation to age group. J Stroke Cerebrovasc Dis. 2008;17:418–22.
Hand P, Kwan J, Lindley R, Dennis M, Wardlaw J. Distinguishing between stroke and mimic at the bedside: the brain attack study. Stroke. 2006;37:769–75.
Hemmen TM, Meyer BC, McClean TL, Lyden PD. Identification of nonischemic stroke mimics among 411 code strokes at the University of California, San Diego, Stroke Center. J Stroke Cerebrovasc Dis. 2008;17:23–5.
Acknowledgment
The authors wish to express their gratitude to James Roberts, B.S., R.N. for data collection assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Giraldo, E.A., Khalid, A. & Zand, R. Safety of Intravenous Thrombolysis within 4.5 h of Symptom Onset in Patients with Negative Post-Treatment Stroke Imaging for Cerebral Infarction. Neurocrit Care 15, 76–79 (2011). https://doi.org/10.1007/s12028-011-9523-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-011-9523-x