
Abstract
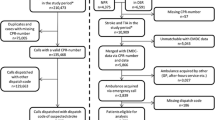
Early identification of stroke should begin in the prehospital phase because the benefits of thrombolysis and clot extraction are time dependent. This study aims to identify patient characteristics that affect prehospital identification of stroke by Long Island college hospital (LICH) emergency medical services (EMS). All suspected strokes brought to LICH by LICH ambulances from January 1, 2010 to December 31, 2011 were included in the study. We compared prehospital care report-based diagnosis against the get with the guidelines (GWTG) database. Age-adjusted logistic regression models were used to study that the effect of individual patient characteristics have on EMS providers’ diagnosis. Included in the study were 10,384 patients with mean age 43.9 years. Of whom, 75 had a GWTG cerebrovascular diagnosis: 53 were ischemic strokes, 7 transient ischemic attacks, 3 subarachnoid hemorrhage, and 12 intercerebral bleeds. LICH EMS correctly identified 44 of 75 GWTG strokes. Fifty-one patients were overcalled as stroke by the EMS. Overall EMS sensitivity was 58.7 % and specificity was 99.5 %. Dispatcher call type of altered mental status, stroke, unconsciousness, and increasing prehospital blood pressure quartile were found to be significantly predictive of a true stroke diagnosis. Patients with a past medical history and EMS providers’ impression of seizures were more likely to be overcalled as a stroke in the field. More than a third of actual stroke patients were missed in the field in our study. Our results show that the patients’ past medical history, dispatcher collected information and prehospital vital sign measurements are associated with a true diagnosis of stroke.


Similar content being viewed by others


References
Strong K, Mathers C, Bonita R (2007) Preventing stroke: saving lives around the world. Lancet Neurol 6:182–187
Global disease burden estimates 2000–2012. World health organisation website. http://www.who.int/healthinfo/global_burden_disease/estimates/en/index2.html. Accessed 23 Sept 2015
Rajajee V, Saver J (2005) Prehospital care of the acute stroke patient. Tech Vasc Interv Radiol 8(2):74–80
Bae HJ, Kim DH, Yoo NT et al (2010) Prehospital notification from the emergency medical service reduces the transfer and intra-hospital processing times for acute stroke patients. J Clin Neurol 6:138–142
McKinney JS, Mylavarapu K, Lane J, Roberts V, Ohman-Strickland P, Merlin MA (2013) Hospital prenotification of stroke patients by emergency medical services improves stroke time targets. J Stroke Cerebrovasc Dis 22(2):113–118
Patel MD, Rose KM, O’Brien EC, Rosamond WD (2011) Prehospital notification by emergency medical services reduces delays in stroke evaluation: findings from the North Carolina stroke care collaborative. Stroke 42:2263–2268
Abdullah AR, Smith EE, Biddinger PD, Kalenderian D, Schwamm LH (2008) Advance hospital notification by EMS in acute stroke is associated with shorter door-to-computed tomography time and increased likelihood of administration of tissue-plasminogen activator. Prehosp Emerg Care 12:426–431
Eissa A, Krass I, Bajorek BV (2012) Barriers to the utilization of thrombolysis for acute ischaemic stroke. J Clin Pharm Ther 37(4):399–409
Ramanujam P, Guluma KZ, Castillo EM, Chacon M, Jensen MB, Patel E et al (2008) Accuracy of stroke recognition by emergency medical dispatchers and paramedics—San Diego experience. Prehosp Emerg Care 12(3):307–313
Fothergill RT, Williams J, Edwards MJ, Russell IT, Gompertz P (2013) Does use of the recognition of stroke in the emergency room stroke assessment tool enhance stroke recognition by ambulance clinicians? Stroke 44:3007–3012
State and county quick facts: Kings County. U.S. Department of Commerce website. http://quickfacts.census.gov/qfd/states/36/36047.html. Accessed 23 Sept 2015
American Heart Association/American Stroke Association (2015) Get with the guidelines stroke registryfact sheet. http://www.heart.org/idc/groups/heart-public/@wcm/@gwtg/documents/downloadable/ucm_310976.pdf. Accessed 23 Sept 2015
Xian Y, Fonarow GC, Reeves MJ, Webb LE, Blevins J, Demyanenko VS, Zhao X, Olson DM, Hernandez AF, Peterson ED, Schwamm LH, Smith EE (2012) Data quality in the American heart association get with the guidelines stroke program: results from a national data validation audit. Am Heart J 163:392–398
Brandler ES, Sharma M, McCullough F et al (2015) Prehospital stroke identification: factors associated with diagnostic accuracy. J Stroke Cerebrovasc Dis 24(9):2161–2166
Brandler ES, Sharma M, Sinert RH, Levine SR (2014) Prehospital stroke scales in urban environments. A systematic review. Neurology 82:2241–2249
Frendl DM, Strauss DG, Underhill BK, Goldstein LB (2009) Lack of impact of paramedic training and use of the Cincinnati prehospital stroke scale on stroke patient identification and on-scene time. Stroke 40:754–756
Bray JE, Martin J, Cooper G, Barger B, Bernard S, Bladin C (2005) Paramedic identification of stroke: community validation of the melbourne ambulance stroke screen. Cerebrovasc Dis 20(1):28–33
Bray JE, Coughlan K, Barger B, Bladin C (2010) Paramedic diagnosis of stroke: examining long-term use of the Melbourne ambulance stroke screen (MASS) in the field. Stroke 41:1363–1366
Bergs J, Sabbe M, Moons P (2010) Prehospital stroke scales in a Belgian prehospital setting: a pilot study. Eur J Emerg Med 17(1):2–6
Qureshi AI, Ezzeddine MA, Nasar A, Suri MF, Kirmani JF, Hussein HM et al (2007) Prevalence of elevated blood pressure in 563,704 adult patients with stroke presenting to the ED in the United States. Am J Emerg Med 25(1):32–38
Irisawa T, Iwami T, Kitamura T, Nishiyama C, Sakai T, Tanigawa-Sugihara K, Hayashida S et al (2013) An association between systolic blood pressure and stroke among patients with impaired consciousness in out-of-hospital emergency settings. BMC Emerg Med 13(1):24
Kidwell CS, Starkman S, Eckstein M, Weems K, Saver JL (2000) Identifying stroke in the field. Prospective validation of the Los Angeles prehospital stroke screen (LAPSS). Stroke 31:71–76
Brandler ES, Sharma M, McCullough F, Khandelwal P, Kinraich D, Ben-Eli D et al (2013) EMS accuracy for stroke identification: seizures lead to overdiagnosis. Acad Emerg Med 20:S99 (abstract 236)
Govindarajan P, Desouza NT, Pierog J, Ghilarducci D, Johnston SC (2012) Feasibility study to assess the use of the Cincinnati stroke scale by emergency medical dispatchers: a pilot study. Emerg Med J 29(10):848–850
Gropen TI, Gokaldas R, Poleshuck R et al (2014) Factors related to the sensitivity of emergency medical service impression of stroke. Prehosp Emerg Care 18(3):387–392
Brandler ES, Sharma M, Khandelwal P et al (2013) Identification of common confounders in the prehospital identification of stroke in Urban, underserved minorities. Stroke 44:AWP243 (abstract)
Acknowledgments
This study was supported in part by NIH grants 1U01NS044364, R01 HL096944, 1U10NS077378, and 1U10NS080377.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of human and animal rights
This article does not contain any studies with animals performed by any of the authors.
Informed consent
For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Sharma, M., Helzner, E., Sinert, R. et al. Patient characteristics affecting stroke identification by emergency medical service providers in Brooklyn, New York. Intern Emerg Med 11, 229–236 (2016). https://doi.org/10.1007/s11739-015-1347-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-015-1347-9