Article Text

Abstract
Background Somatic mutation contributes to clonal haematopoiesis of indeterminate potential (CHIP) is related to age and associated with a higher risk of stroke and atherosclerotic cardiovascular disease. Here, we investigated the prognostic significance of CHIP in a large first-ever acute ischaemic stroke (AIS) cohort and explored the underlying mechanisms.
Methods We studied a prospective cohort of 6016 patients who had a first-ever AIS in China. Whole-genome sequencing was performed to identify CHIP. High-sensitivity C reactive protein (hs-CRP) levels above 3 mg/L at baseline were defined as hyperinflammation. Recurrent stroke during the 3-month follow-up was the primary outcome.
Results Among the 6016 patients who had a first-ever AIS, with a median age was 62 years (IQR, 54.0‒70.0), 3.70% were identified as CHIP carriers. The most common mutations occurred in the DNMT3A (30.0%) and TET2 (11.4%) genes. During a follow-up of 3 months, the presence of CHIP was associated with recurrent stroke (HR 1.62, 95% CI 1.04 to 2.51, p=0.03), recurrent ischaemic stroke (HR 1.64, 95% CI 1.04 to 2.58, p=0.03) and combined vascular events (HR 1.58, 95% CI 1.02 to 2.44, p=0.04) after adjusting for hsCRP levels at baseline in patients who had a first-ever AIS. Subgroup analysis demonstrated that CHIP was only associated with recurrent stroke when patients under hyperinflammation (OR 3.10, 95% CI 1.92 to 5.00, p<0.001) but not in those without hyperinflammation (OR 0.18, 95% CI 0.03 to 1.04, p=0.06, Pinteraction=0.002).
Conclusion Our results suggest that somatic mutations contributing to CHIP increase the risk of short-term recurrent stroke in patients who had a first-ever AIS. Hyperinflammation may be important in the relationship between CHIP and recurrent stroke.
- Stroke
- Genetics
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Clonal haematopoiesis of indeterminate potential (CHIP) describes individuals with somatic mutations related to haematopoietic clones but without haematologic abnormalities. Results from large-scale genetic studies demonstrate that CHIP is associated with stroke and atherosclerotic cardiovascular disease. Additionally, experimental evidence shows that CHIP accelerates atherosclerosis via specific inflammatory pathways. However, the association between CHIP and the prognosis of first-ever acute ischaemic stroke (AIS) remains unknown.
WHAT THIS STUDY ADDS
While previous CHIP-related studies have mainly focused on the white population, our study supplemented the Asian population data. In contrast to previous studies, we described the prognostic significance of CHIP in patients who had a first-ever AIS and explored potential mechanisms. Our study included 6016 patients who had a first-ever AIS, and we found that CHIP was associated with short-term recurrent stroke, recurrent ischaemic stroke and combined vascular events, especially when patients under hyperinflammation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
CHIP is a new risk factor affecting recurrent stroke in patients who had a first-ever AIS, and some inflammatory pathways might be potential mechanisms between CHIP and the prognosis of AIS. Future studies should validate the underlying mechanisms and discuss the impact of inflammation-targeted therapies to improve poor outcomes in patients who had a first-ever AIS.
Introduction
Clonal haematopoiesis of indeterminate potential (CHIP) describes individuals with gene mutations related to haematologic malignancies but without haematologic malignancy or other clonal disorders.1 CHIP is a common consequence of ageing, and evidence shows that it is a new risk factor of atherosclerotic cardiovascular diseases. Mechanistically, CHIP mutations affect immune effector cells and target specific inflammatory mediators, which may efficiently increase the risk of cardiovascular disease.2 3
As a major cause of disability globally, stroke is a chronic disease that is related to age.4 5 In China, the incidence of stroke (first-ever strokes that occurred within 1 year before the record time) is approximately 246.8/100 000 person-years after age standardisation.6 Moreover, patients have a residual risk of recurrence within days or weeks of symptom onset, even after guideline-based prevention and quality care.7 Therefore, more effective intervention methods that target the unconventional risk factors for stroke are needed. Recently, a large-scale genetic study suggested that CHIP increased the risk of stroke.8 However, the potential prognostic significance of CHIP in patients who had a first-ever acute ischaemic stroke (AIS) remains unknown. Hence, we assessed the characteristics of CHIP by whole-genome sequencing (WGS) in a large cohort of patients who had a first-ever AIS and investigated the prognostic significance of CHIP in first-ever AIS.
Methods
Study participants
Our study was based on a nationwide, prospective cohort (The Third China National Stroke Registry (CNSR-III)) that contained 15 166 patients who presented to hospitals with AIS (n=14 146, 93.3%) or transient ischaemic attack (TIA) (n=1020, 6.7%).9 Patients enrolled in this study were selected from 10 914 patients who participated in the genetic substudy of CNSR-III.10 We defined patients without a history of ischaemic stroke or TIA as first-ever AIS. We included 6016 patients who had a first-ever AIS without history of malignancies and whose qualified genomic data and complete clinical information during the 3-month follow-up were available. A flowchart of patients’ selection is shown in online supplemental figure 1. All patients or legally authorised representatives had signed informed consents before they were recruited in CNSR-III.
Supplemental material
The participants’ laboratory data and clinical information were prospectively collected. The primary outcome in this study was recurrent stroke at 3 months, which was defined as a new ischaemic or haemorrhagic stroke occurred during 3-month follow-up after symptom onset. The secondary outcomes in this study included recurrent ischaemic stroke, combined vascular events and all-cause mortality at 3 months. The definitions of these clinical outcomes were published previously.9 Follow-up data collection at 3 months after admission were conducted by trained research coordinators face to face.
The diagnosis of AIS in all participants was confirmed by brain imaging, and aetiology classifications of all participants in our cohort were performed with reference to the Trial of Org 10 172 in Acute Stroke Treatment (TOAST) criteria.11 12 We used high-sensitivity C reactive protein (hs-CRP) levels to evaluate the inflammation status of patients, which were measured centrally in Beijing Tiantan Hospital using blood samples collected within 24 hours of admission. We divided our patients into different groups according to the relative risk stratification of hs-CRP levels (0–3 mg/L and >3 mg/L), as recommended by the Centers for Disease Control and Prevention and the American Heart Association for cardiovascular disease risk assessment.13 Hs-CRP levels above 3 mg/L at baseline were defined as hyperinflammation.
Image data collection and vascular assessments
The assessment of intracranial artery stenosis or occlusion in all patients was based on the results of at least one vascular imaging assessment for intracranial. The intracranial arterial segments included the posterior cerebral, middle cerebral, anterior cerebral, basilar and internal carotid artery (intracranial segments). The Warfarin-Aspirin Symptomatic Intracranial Disease Study criteria14 were used to evaluate the intracranial atherosclerotic stenosis (ICAS). Furthermore, assessment of atherosclerosis burden was evaluated by the degree of ICAS and categorised into three groups in this study: no stenosis or <50% stenosis, 50%–99% stenosis and occlusion.
Whole-genome sequencing (WGS)
Total DNA obtained from the CNSR- III cohort was isolated from peripheral white blood cells. WGS was performed using the BGISEQ-500 platform (BGI Genomics, Shenzhen, China), and we stored the sequence data in the form of FASTQ for subsequent processes. The average sequencing depth was greater than 30 times. Raw data were cleaned using the following steps: both paired reads were removed if any one of the reads (1) contained a sequencing adapter, (2) the ratio of low-quality base (base quality≤12) >50% or (3) the ratio of unknown base (‘N’ base)>10%. Low-quality reads and bases were filtered out using fastp (V.0.20.0), and these qualified data were analysed by downstream bioinformatics. More details of gene mapping and variant calling were reported previously.10
Somatic mutation detection
GATK MuTect2 software (https://software.broadinstitute.org/gatk) was used to detect the putative somatic variants. We used a coverage of 10, variant allele frequency (VAF) of 0.05 and minimum variant read counts of 3 for MuTect2 to call somatic variants. A public panel of healthy controls (gs://gatk-best-practices/somatic-hg38/1000g_pon.hg38.vcf.gz) was used. Mutations in these regions previously reported in the literature and the Catalogue of Somatic Mutations in Cancer (http://cancer.sanger.ac.uk/cancer genome/projects/cosmic/) were used in the following analysis. An exact binomial test was performed to remove likely germline variations according to a previously reported method.2 15 For heterozygous germline variations, alternate allele frequencies were assumed to be approximately 0.5. Therefore, we performed an exact binomial test to determine whether a significant difference between the VAF and expected distribution of a germline allele existed. We used the read count of the reference allele plus the alternate allele as the number of trials and the read count of the alternate allele as the number of successes. Variants with a p value less than 0.001 were considered somatic mutations. Pathogenic variants in the exon regions of 74 genes related to human myeloid cancer were defined as CHIP.2
Statistical analysis
Means with SD or medians (IQR) were reported for continuous variables, and numbers (percentages) were reported for categorical variables. The Wilcoxon rank-sum test was used for continuous variables, whereas the χ2 test was used to compare the differences of response rate. Multivariate logistic regression model including age and sex was used to calculate the association between CHIP and blood traits. Kaplan-Meier analyses were displayed as cumulative event (recurrent stroke, combined vascular event and all-cause mortality) rate curves. The correlation between outcomes and CHIP was evaluated using HRs and calculated using the Cox proportional hazards model. To balance the characteristics between CHIP carriers and non-CHIP carriers, and reduce the influence of very small estimated probabilities from the propensity score (PS) model, we conducted the stabilised inverse probability of treatment weighting (IPTW) based on the PS.16 Three models were used for calculating PS when using stabilised IPTW: model 1, PS were calculated from patient characteristics at baseline, including age, sex, hypertension, diabetes, lipid metabolism disorders, heart disease, body mass index, drinking, smoking, admitting National Institutes of Health Stroke Scale and aetiology classification (TOAST); model 2, additionally included baseline hs-CRP based on model 1; model 3, additionally included the severity of ICAS at baseline based on model 1. We also tested the interaction among CHIP, inflammatory status and atherosclerosis burden on the primary outcome. The results were considered as statistical significance at a two-sided p value<0.05. SAS V.9.4 was used for all statistical analyses that performed in this study.
Result
Characteristics of study population and detection of mutations
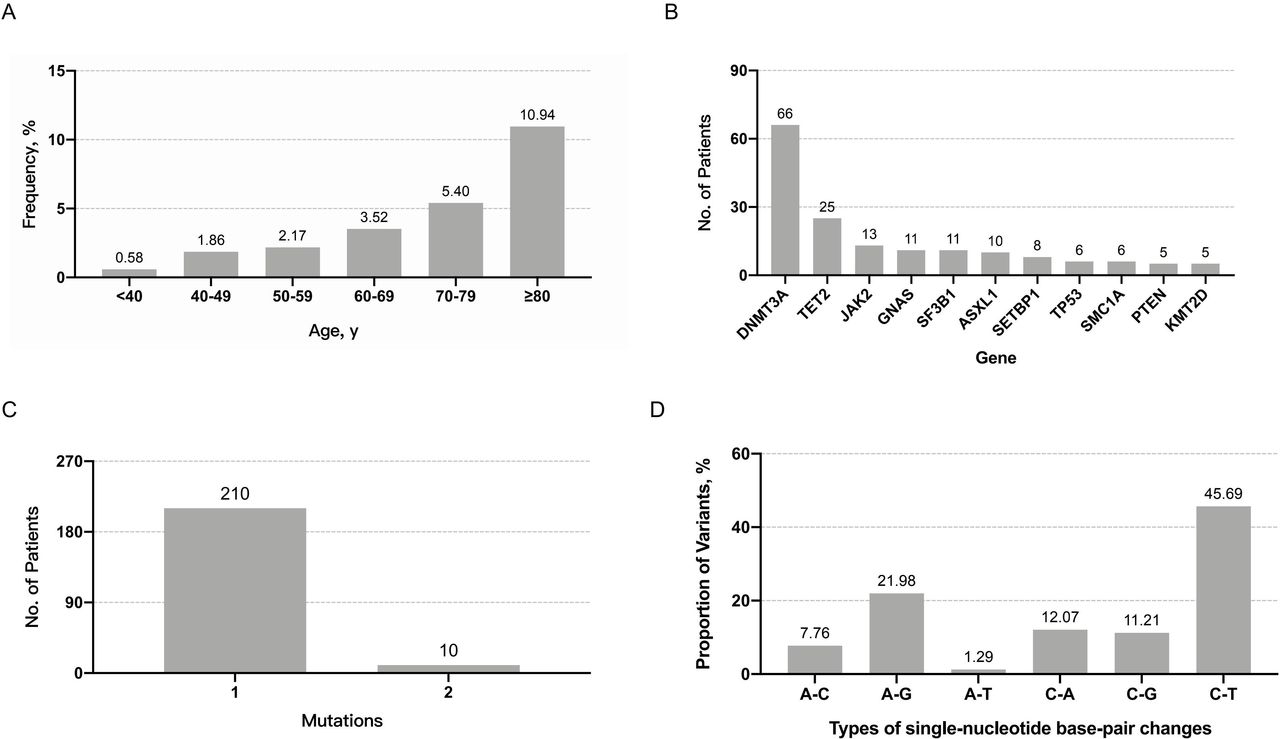
Among the 6016 patients who had a first-ever AIS, the median age was 62 years (IQR, 54.0–70.0), and 31.0% (1863/6016) were women. In total, 220 patients (3.70%) were identified as CHIP carriers, and the prevalence of CHIP in our cohort, especially DNMT3A and TET2 mutation carriers, significantly increased with age (figure 1A and online supplemental figure 2). The frequency of mutations in the >80 years age group was the highest among all groups, up to 10.94% (36 of 329 patients). DNMT3A (30.0%), TET2 (11.4%), JAK2 (5.9%), GNAS (5.0%) and SF3B1 (5.0%) were the most frequently mutated genes (figure 1B), accounting for over half of all the CHIP carriers. A total of 210 (95.5%) CHIP carriers had a single-driver gene mutation (figure 1C), indicating that clones in most CHIP carriers were only present at the initial stage. The cytosine-to-thymine transition was the most common single-nucleotide variant type (figure 1D), accounting for 45.69%, which was thought to be an age-related somatic mutation.17

Characteristics of clonal haematopoiesis of indeterminate potential (CHIP). (A) Distribution of CHIP carriers according to age. (B) Ten most common mutated genes leading to CHIP in this cohort. (C) The number of persons with one or two candidate variants. (D) Number of the types of changes in variant single-nucleotide base pair.
Baseline characteristics of study population
Baseline characteristics of the total 6016 patients who had a first-ever AIS according to the CHIP status are summarised in table 1. As illustrated, CHIP carriers were 6 years older than non-CHIP carriers (p<0.0001), but the differences between CHIP and non-CHIP carriers in risk factors of vascular disease were not significant. Drinking and smoking habits were associated with a reduced probability of CHIP in unadjusted analysis, but these differences were not significant after adjusting for sex and age (OR=1.43, 95% CI 0.92 to 2.22, p=0.12 and OR=1.11, 95% CI 0.79 to 1.57, p=0.54, respectively). Furthermore, CHIP was not associated with the distribution of the TOAST classification.
Baseline characteristics of the study population
Associations of CHIP and blood traits
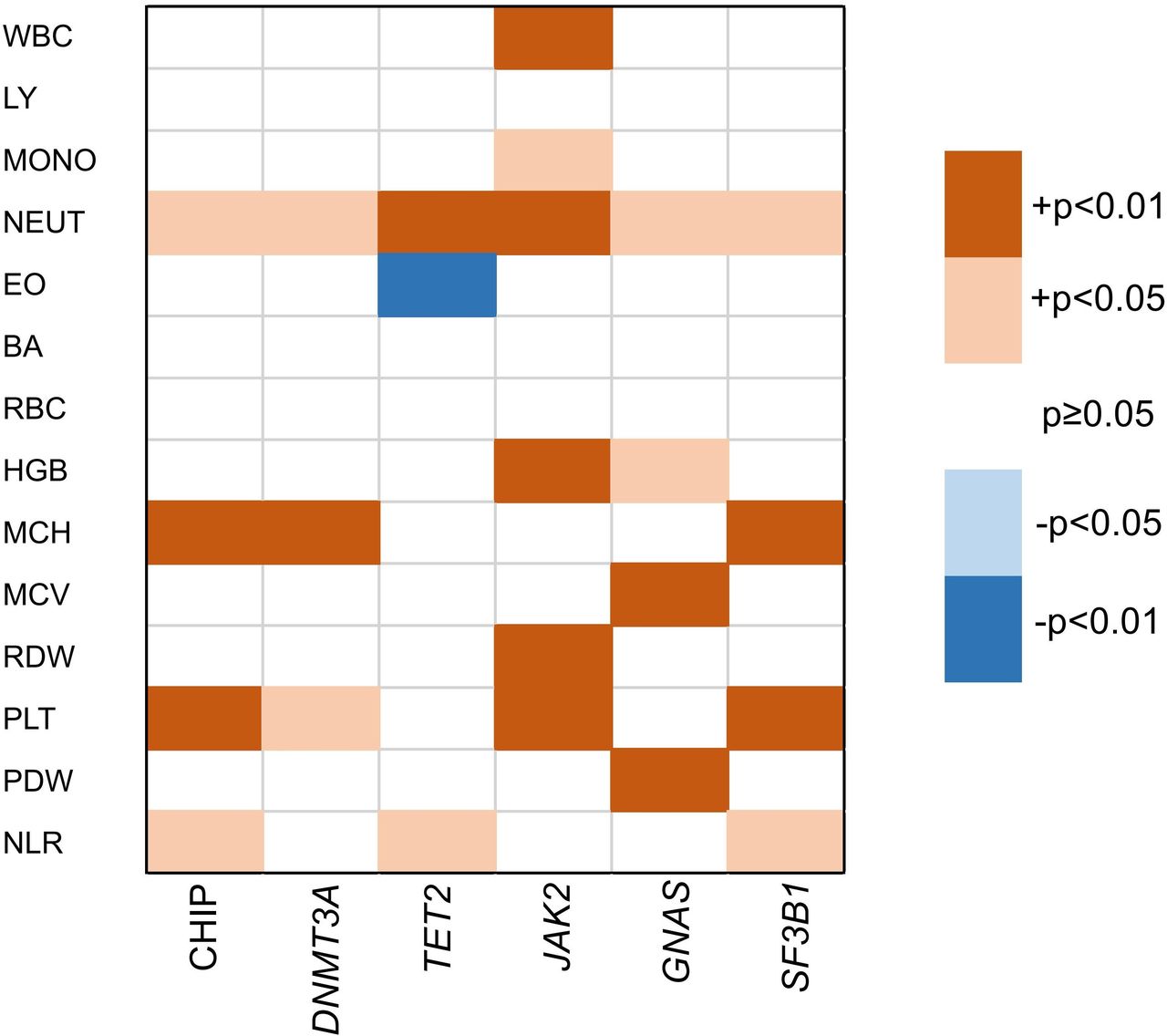
As CHIP may affect haematopoiesis in patients, we next investigated the blood profile of CHIP carriers in our cohort. We found that different CHIP genes had different effects on blood characteristics. Overall, CHIP was associated with an increased neutrophil (NEUT) count, neutrophil-to-lymphocyte ratio (NLR), mean corpuscular haemoglobin and platelet count. Notably, NLR in CHIP carriers was significantly higher than that in non-CHIP carriers (3.9 vs 3.2, p<0.001). Furthermore, the five most common genes (DNMT3A, TET2, JAK2, GNAS and SF3B1) were associated with elevated NEUT levels (figure 2; Online supplemental table 1). In addition, JAK2 mutations were significantly increased the levels of red cell distribution width (p<0.001), a parameter that predicts poor outcomes in the elderly regardless of age-associated diseases.18
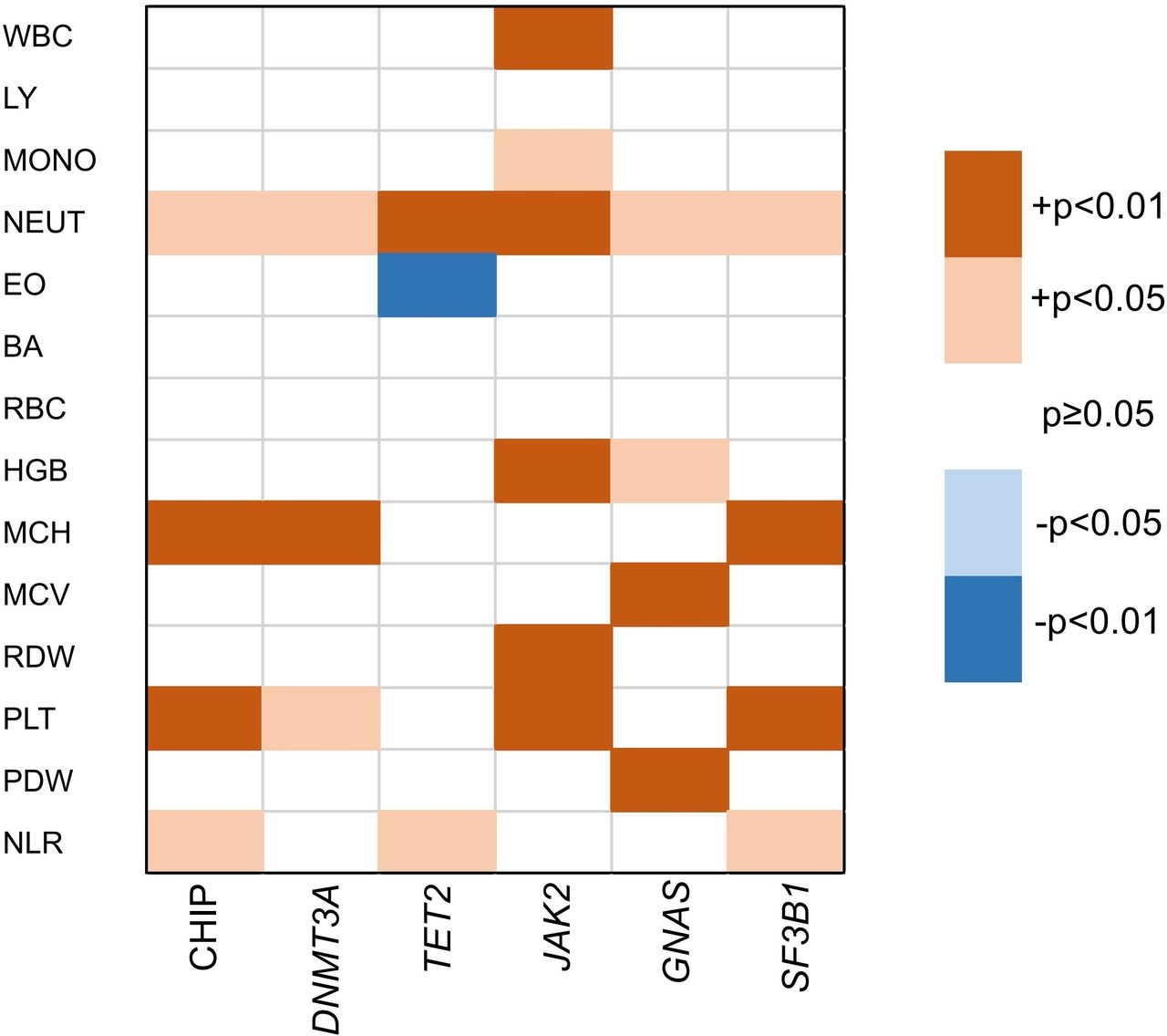
Association of CHIP and blood traits. The positive correlation was represented in orange; and negative correlation was represented in blue. BA, basophil count; EO, eosinophil count; HGB, haemoglobin; LY, lymphocyte count; MCH, mean corpuscular haemoglobin; MCV, mean corpuscular volume; MONO, monocyte count; NEUT, neutrophil count; NLR, neutrophil-to-lymphocyte ratio; PLT count, platelet; PDW, platelet distribution width; RBC, red blood cell count; RDW, red blood cell distribution width; WBC, white blood cell count.
Prognostic significance of CHIP in patients who had a first-ever AIS
At the 3-month follow-up, 357 (5.93%) patients had a recurrent stroke, 333 (5.54%) had a recurrent ischaemic stroke, 367 (6.10%) patients had combined vascular events and 72 (1.20%) patients died. Higher rates of recurrent stroke (6.36% vs 5.92%), recurrent ischaemic stroke (5.91% vs 5.52%), combined vascular events (6.36% vs 6.09%) and all-cause mortality (1.36% vs 1.19%) were observed in the CHIP carriers than in non-CHIP carriers. Results of Kaplan-Meier event-free survival analysis showed that the cumulative risk of clinical outcomes between CHIP carriers and non-CHIP carriers was not different (online supplemental figure 3). We next assessed the association of CHIP with different outcomes using Cox proportional regression analysis with three adjustment models. CHIP was significantly associated with recurrent stroke (HR 1.62, 95% CI 1.04 to 2.51, p=0.03), recurrent ischaemic stroke (HR 1.64, 95% CI 1.04 to 2.58, p=0.03) and combined vascular events (HR 1.58, 95% CI 1.02‒2.44, p=0.04) after adjusting for hs-CRP levels at baseline (table 2), which is a biomarker associated with both recurrent stroke19 and CHIP.20 In addition, CHIP was significantly associated with recurrent ischaemic stroke (HR 1.59, 95% CI 1.00‒2.51, p=0.048) without adjusting for hs-CRP levels (table 2).
Associations between CHIP and different outcomes in patients who had a first-ever AIS
Association of CHIP and recurrent stroke in selected subgroups
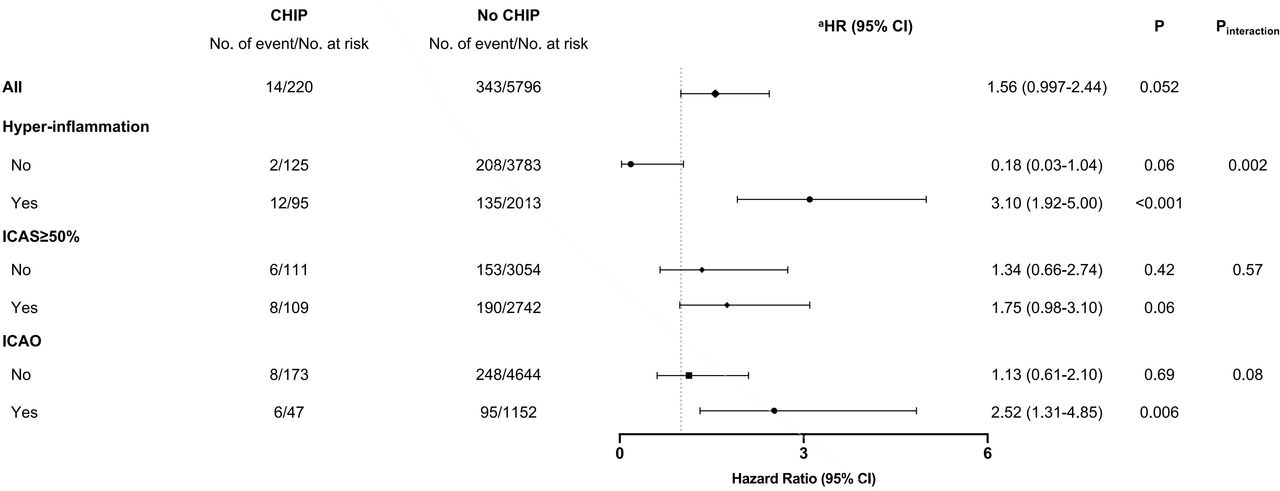
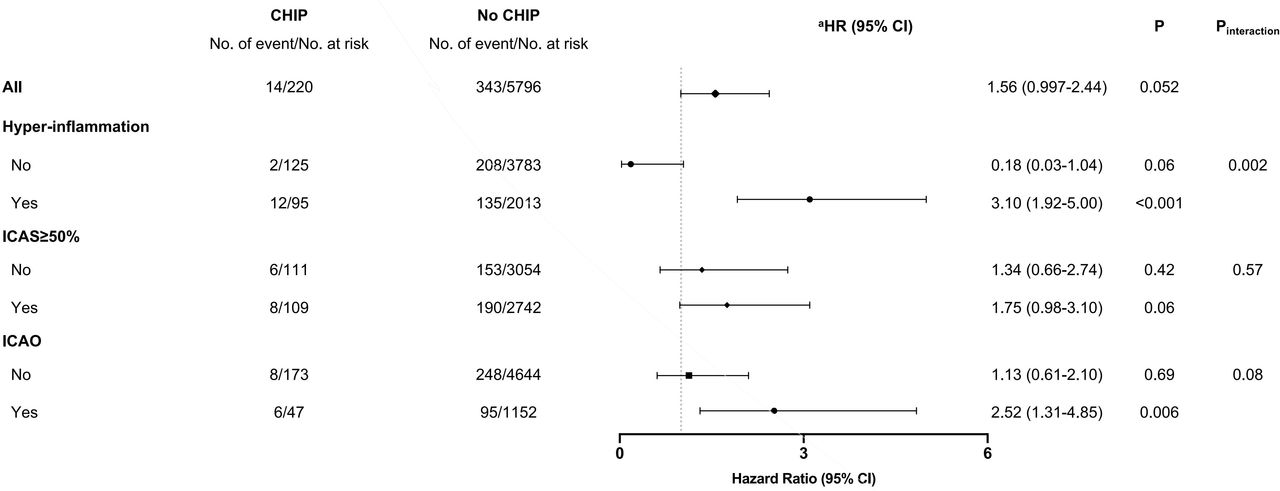
The results of subgroup analysis to explore factors that influence the relationship between CHIP and the primary outcome, including inflammation status and severity of ICAS, are shown in figure 3 and online supplemental table 2. Among patients with hyperinflammation, the rate of recurrent stroke in CHIP carriers (12.63%) was 1.9-fold higher than that in non-CHIP carriers (6.71%), and CHIP significantly increased the risk of recurrent stroke when patients under hyperinflammation (HR 3.10, 95% CI 1.92 to 5.00, p<0.001); in contrast, the presence of CHIP had no significant effect on recurrent stroke in patients without hyperinflammation (HR 0.18, 95% CI 0.03 to 1.04, p=0.06). The apparent difference in ORs was statistically significant (Pinteraction=0.002).
{kind=link}
{kind=link}
{kind=link}
Associations between CHIP and recurrent stroke in selected subgroups. aCox proportional hazards model was adjusted by stable inverse probability of treatment weighting based on the propensity score (PS). Variables used for calculating PS included age, sex, body mass index, smoking, drinking, history of the disease (ie, hyperlipidaemia, diabetes mellitus and hypertension), Trial of Org 10 172 in Acute Stroke Treatment classification and National Institutes of Health Stroke Scale. CHIP, clonal haematopoiesis of indeterminate potential; ICAO, intracranial cerebral artery occlusion; ICAS, intracranial atherosclerotic stenosis.
Next, we analysed the subgroups stratified by ICAS severity. We observed that CHIP increased the risk of recurrent stroke in patients with ICAS≥50% (HR 1.75, 95% CI 0.98 to 3.10, p=0.06), which was slightly higher than that in patients with ICAS<50% (HR 1.34, 95% CI 0.66 to 2.74, p=0.42); however, there were no statistical significance in both groups. In the intracranial cerebral artery occlusion (ICAO) subgroup analysis, which was the most severe ICAS, CHIP was significantly associated with recurrent stroke in patients with ICAO (HR 2.52, 95% CI 1.31 to 4.85, p=0.006) but not in those patients without ICAO (HR 1.13, 95% CI 0.61 to 2.10, p=0.69). However, the interaction between CHIP and ICAO for the risk of recurrent stroke was not significant (Pinteraction=0.08).
Discussion
Our study demonstrated that CHIP was frequent in elderly patients who had a first-ever AIS, and associated with recurrent stroke, recurrent ischaemic stroke and combined vascular events of patients who had a first-ever AIS, especially when patients under hyperinflammation.
In this study, the prevalence of CHIP was approximately 3.70%, based on a variant allele frequency (VAF) of mutation>0.05, which was slightly lower than the previously reported 6.5% in a coronary heart disease cohort with a median age of 60 years2 and 4.3% in the general population.17 This is likely owing to the ethnic differences and the characteristics of the study population. Consistent with the previous studies,21 CHIP frequently occurred in patients who had an AIS of advanced age, especially when patients were over 80 years of age. Also, the genes involved in epigenetic regulation were the most frequently mutated in CHIP carriers, such as DNMT3A and TET2, which are also ageing signatures. The association of CHIP with blood characteristics revealed that the NLR value of CHIP carriers, which is a predictive marker of short-term adverse outcomes of first-ever stroke,22 was significantly higher than that of non-CHIP carriers. Moreover, NLR is considered a measurement index of inflammation levels,23 suggesting a relationship among CHIP, inflammation and poor outcomes of first-ever AIS.
Our results revealed that CHIP was significantly associated with recurrent stroke, recurrent ischaemic stroke, and combined vascular events in patients who had a first-ever AIS. We used three different IPTW models to weight the Cox regression model, and each of the models gave the similar results. However, only the model with hs-CRP was statistically significant, suggesting that hs-CRP levels at baseline might play a key role between CHIP and outcomes of first-ever AIS. Fuster et al 24 have shown that CHIP contributes to the development of cardiovascular disease by targeting specific inflammatory pathways. They reported that, in a mice model with low-density lipoprotein receptor-deficient (Ldlr–/–), TET2-driven CHIP leads to a noticeable increase in atherosclerotic plaque size by generating a pool of macrophages with elevated transcript levels of inflammatory markers, including IL-6 and IL-1β. Another study demonstrated that monocytes from patients with cardiovascular disease and DNMT3A/TET2 -driven CHIP might cause excessive inflammatory responses.25 Inflammation is also a considerable risk factor independent of traditional vascular risk factors for recurrent ischaemic stroke and contributes to the rupture of atherosclerotic plaque.26 27 Hs-CRP is a widely used inflammatory biomarker that can reflect hyperinflammation after AIS, and the relationship between hs-CRP and stroke has been extensively investigated.19 Our subgroup analysis illustrated that the risk of recurrent stroke increased by CHIP was only significant in patients with hyperinflammation, which indicates that hyperinflammation appeared to play a critical role between CHIP and recurrent stroke. Accordingly, our results suggest that CHIP is of great significance for recurrent stroke, which may be due to the exaggerated poststroke inflammatory response that results in the rupture of unstable plaque. However, further experimental evidence is needed for a definitive causal relationship among CHIP, inflammation and recurrent stroke.
Previous investigations have revealed that a higher atherosclerosis burden, such as intracranial artery occlusion, was another independent predictor for recurrent stroke in addition to inflammation status.28–30 We found that CHIP carriers had a significantly higher risk of recurrent stroke only when they had ICAO, but a significant interaction of CHIP and the severity of ICAS was not observed. Therefore, we hypothesise that, unlike cardiovascular disease, the adverse effect of CHIP on the recurrent stroke in patients who had a first-ever AIS is not mainly caused by an increased atherosclerosis burden. In contrast, inflammation may play a more important role between CHIP and recurrent stroke.
Limitations
We had several limitations in this study. Although it is the largest to date to focusing on CHIP and stroke prognosis, the number of CHIP carriers is limited, which might have prevented the assessment of the association between CHIP driver mutations and clinical outcomes. When calculating Cox regression, we used stabilised IPTW models to balance the confounding and sample size so that the p value was close to 0.05. However, the results still require further verification in other cohorts to make the evidence more conclusive. Moreover, we only explored CHIP as a whole and did not evaluate the specific effect for each of them. Further study to investigate this issue in a larger scale cohort will be conducted in future work. In addition, all of our participants were enrolled only from the Chinese population; therefore, our results require further validation in worldwide cohorts. Nevertheless, we firmly believe that our exploratory research results are strongly suggestive.
Conclusion
We found that CHIP was frequent in elderly patients and it was associated with recurrent stroke, recurrent ischaemic stroke, and combined vascular events 3 months after symptom onset in first-ever AIS, especially when patients under hyperinflammation. We propose that the hyperinflammation status might play a critical role in the association between CHIP and recurrent stroke. Future studies should conduct external clinical cohort verification and experimental validation of the underlying mechanisms.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The protocol of this study was reviewed and approved by ethics committee of Beijing Tiantan Hospital (KY2015-001-01). Participants gave informed consent to participate in the study before taking part.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
YW and ZL contributed equally.
Contributors ZL and YoW designed the study. YoJ, XM, YiW and XZ acquired the data. XQ, HQ-G, YiJ, XH, ZX and HL analysed and interpreted the data. XQ, YD and SC analysed the genomic data. XQ wrote the manuscript. ZL and YoW revised the manuscript. All of other authors discussed the results and approved the manuscript. ZL is responsible for the overall content as guarantor.
Funding This study was supported by grants from National Natural Science Foundation of China (grant number 82171270, 81870905, U20A20358), Natural Science Foundation of Beijing (Z200016) and Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2019-I2M-5-029).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.