Article Text

Abstract
Introduction The efficacy and safety of local intra-arterial (IA) thrombolytics during endovascular thrombectomy (EVT) for large-vessel occlusions is uncertain. We analysed how often IA thrombolytics were administered in the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) Registry, whether it was associated with improved functional outcome and assessed technical and safety outcomes compared with EVT without IA thrombolytics.
Methods In this observational study, we included patients undergoing EVT for an acute ischaemic stroke in the anterior circulation from the MR CLEAN Registry (March 2014–November 2017). The primary endpoint was favourable functional outcome, defined as an modified Rankin Scale score ≤2 at 90 days. Secondary endpoints were reperfusion status, early neurological recovery and symptomatic intracranial haemorrhage (sICH). Subgroup analyses for IA thrombolytics as primary versus adjuvant revascularisation attempt were performed.
Results Of the 2263 included patients, 95 (4.2%) received IA thrombolytics during EVT. The IA thrombolytics administered were urokinase (median dose, 250 000 IU (IQR, 1 93 750–2 50 000)) or alteplase (median dose, 20 mg (IQR, 12–20)). No association was found between IA thrombolytics and favourable functional outcome (adjusted OR (aOR), 1.16; 95% CI 0.71 to 1.90). Successful reperfusion was less often observed in those patients treated with IA thrombolytics (aOR, 0.57; 95% CI 0.36 to 0.90). The odds of sICH (aOR, 0.82; 95% CI 0.32 to 2.10) and early neurological recovery were comparable between patients treated with and without IA thrombolytics. For primary and adjuvant revascularisation attempts, IA thrombolytics were more often administered for proximal than for distal occlusions. Functional outcomes were comparable for patients receiving IA thrombolytics as a primary versus adjuvant revascularisation attempt.
Conclusion Local IA thrombolytics were rarely used in the MR CLEAN Registry. In the relatively small study sample, no statistical difference was observed between groups in the rate of favourable functional outcome or sICH. Patients whom required and underwent IA thrombolytics were patients less likely to achieve successful reperfusion, probably due to selection bias.
- Stroke
- Thrombectomy
- Thrombolytic Therapy
Data availability statement
No data are available.
Data availability statement
Data will not be made available to other researchers as no patient approval has been obtained for sharing data. Syntax files will be made available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
A recent trial demonstrated that local intra-arterial thrombolytics during endovascular thrombectomy improved patient outcomes. However, it is uncertain how often intra-arterial thrombolytics are used and whether this positive effect is also present in daily clinical practice.
WHAT THIS STUDY ADDS
In this non-randomised, observational study from the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands Registry, local intra-arterial thrombolytics were rarely used. In the relatively small study sample, no statistical difference was detected between groups in the rate of favourable functional outcome or symptomatic intracranial haemorrhage.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
As local intra-arterial thrombolytics were rarely used and were not associated with favourable outcome, larger studies are needed to confirm a potential beneficial effect.
Introduction
Treatment of acute ischaemic stroke has been the centre of attention in recent decades. Starting from 1990, intracranial thrombi were treated by administration of systemic intravenous thrombolysis or local intra-arterial (IA) thrombolytics.1–5 Intravenous thrombolysis became standard of care after publication of the National Institute of Neurological Disorders and Stroke and European Cooperative Acute Stroke Study trials.4 5 In the years that followed, the effectiveness and safety of mechanical endovascular thrombectomy (EVT) was proven for patients with a large-vessel occlusion as an adjunct to intravenous thrombolysis.6–11
Despite the success of EVT, approximately 55% of the patients are functionally dependent or deceased at 90 days after EVT.11 This may be partially explained by incomplete macrovascular recanalisation or incomplete microvascular reperfusion.12 Incomplete macrovascular recanalisation may be due to technical difficulties regarding clot removal, such as thrombus fragmentation to inaccessible distal territories,13 fibrin-rich thrombus composition14 and anatomical challenges, such as tortuous arteries.15 Incomplete microvascular reperfusion has been related to the presence of microthrombi or neutrophil extracellular traps.16 To improve macrovascular recanalisation rates, microvascular reperfusion and subsequently functional outcomes, local IA thrombolytics may be administered during EVT.
In the Prolyse in Acute Cerebral Thromboembolism1 2 and prematurely terminated Middle Cerebral Artery Embolism Local Fibrinolytic Intervention Trial3 trials conducted before the introduction of EVT with stent retrievers and aspiration catheters, better functional outcomes and reperfusion rates were observed in patients treated with local IA thrombolytics than in patients treated without. Recent observational studies reported improved outcomes after use of local IA thrombolytics as adjuvant revascularisation attempt during EVT.17–19 These latter results could, however, not be confirmed by a meta-analysis.20 Moreover, despite growing evidence on the safety of IA thrombolytics, there still is a fear of an increased risk of intracranial haemorrhage.17–23
In this study, we analysed how often local IA thrombolytics were used during EVT in the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) Registry and whether IA thrombolytics were associated with improved functional outcome. We further assessed technical and safety outcomes compared with EVT without IA thrombolytics.
Methods
Study design
This is a non-randomised, observational study of prospectively collected data from the MR CLEAN Registry between March 2014 and November 2017. The MR CLEAN Registry is a multicentre, observational study in which patients who were treated endovascularly (defined as arterial puncture in the angiography suite) for a large-vessel occlusion in the Netherlands were enrolled. The study design and patient eligibility criteria have been reported previously.24
The medical ethics committee of the Erasmus University Medical Centre Rotterdam in the Netherlands evaluated the study and granted permission to carry out the study as an observational registry (MEC-2014-235).
Data will not be made available to other researchers as no patient approval has been obtained for sharing data. Syntax files will be made available from the corresponding author on reasonable request.
Participants
Patients with an acute ischaemic stroke due to a proximal occlusion in the anterior circulation who underwent EVT (defined as an attempt to remove or dissolve the intracranial occlusion by thrombectomy or local IA thrombolytics) were included. Exclusion criteria were age under 18 years, EVT in a non-MR CLEAN trial centre, initiation of EVT more than 6.5 hours after onset of symptoms, a prestroke modified Rankin Scale (mRS) score >2 and missing data on administration of local IA thrombolytics. The choice of interventional technique, use of local IA urokinase or alteplase and dose was left to the discretion of the interventionist.
Outcome measurement
The primary endpoint was favourable functional outcome, defined as an mRS score of ≤2 at 90 days after EVT, reflecting independency for activities of daily living.25
The secondary endpoints were successful reperfusion, excellent reperfusion, early neurological recovery and occurrence of symptomatic intracranial haemorrhage (sICH). Successful reperfusion was defined as an extended Thrombolysis In Cerebral Infarction (eTICI) score of ≥2B immediately after EVT. Excellent reperfusion was defined as an eTICI score of ≥2C immediately after EVT.26 If the anteroposterior or lateral digital subtraction angiography (DSA) run immediately after EVT was unavailable, the assessment was based on only one DSA view with an eTICI score of 2A being the highest possible grading.24 Early neurological recovery was defined as a postprocedural National Institutes of Health Stroke Scale (NIHSS) score of 0 or 1 within 24 hours, or a decrease of 8 points relative to baseline.8 An intracranial haemorrhage was considered to be symptomatic if patients deteriorated neurologically (a decline of at least 4 points on the NIHSS) or died within 90 days after EVT and the haemorrhage was related to the clinical deterioration (according to the Heidelberg criteria).24 27
Data collection
A core lab, blinded to the clinical characteristics and outcome (except for symptom side), evaluated imaging data on location of the intracranial occlusion, collateral status, time from stroke onset to recanalisation or last contrast bolus, eTICI score before and after EVT and presence of sICH within 90 days after EVT.
For each patient, data on revascularisation attempts during EVT were registered. For the first three thrombectomy passes, it was recorded in the MR CLEAN Registry what the passes entailed (local IA thrombolytics, stent retriever or aspiration). Also, procedural reports were included in the database. From these variables, we could extract whether or not IA thrombolytics had been administered during EVT. Local IA thrombolytics were administered during a primary revascularisation attempt if no prior thrombectomy passes had been performed. Local IA thrombolytics were administered during an adjuvant revascularisation attempt if prior thrombectomy passes had been performed.
Additional reassessment of DSA images was performed by two neurointerventionists (MJ and RB) to acquire data on the most proximal location of the occlusion for which IA thrombolytics were administered. An occlusion was considered to be located proximally in case of an obstruction in the intracranial internal carotid artery, M1 or M2 segment, A1 or A2 segment or anterior communicating artery. An occlusion was considered to be located distally in case of an occlusion in the M3 of M4 segment, posterior communicating artery or posterior cerebral artery. Furthermore, additional data were collected on the procedural use of heparin. Procedural use of heparin was defined as administration of heparin either as a single bolus or continuously in saline flush during EVT.28
Statistical analysis
Baseline characteristics, procedural characteristics and outcomes were presented for patients treated with and without local IA thrombolytics.
Based on previous data,29 a sample size of 172 patients (86 patients per group) would have been required to detect an absolute difference in the rate of good functional outcome of 19%, assuming the rate of favourable functional outcome in the control group to be 63% (as was observed in the Chemical Optimization of Cerebral Embolectomy (CHOICE) trial),29 to achieve a significance level of 5% (two-sided) and a power of 80%.
To facilitate statistical comparisons despite the small number of observations in some of the categories, the mRS score was dichotomised into favourable and poor functional outcome, and the eTICI score into successful and unsuccessful reperfusion, and into excellent and non-excellent reperfusion. Univariable and multivariable logistic regression analyses were performed to analyse the association between local IA thrombolytics and primary and secondary endpoints.
For the primary endpoint, three stratified analyses were conducted to test for interaction between IA thrombolytics and intravenous thrombolysis, IA thrombolytics and procedural use of heparin and IA thrombolytics and EVT before versus after 1 January 2016. The significance of the interaction terms was tested in logistic regression models that consisted of the separate predictors and their joined effect. Furthermore, within the group of patients who were treated with local IA thrombolytics, three subgroup analyses were performed. We determined whether administration of local IA thrombolytics as primary revascularisation attempt was associated with favourable functional outcome or with successful reperfusion, and whether administration of local IA thrombolytics for a distal occlusion was associated with favourable functional outcome. An association between IA thrombolytics for a distal occlusion and successful reperfusion could not be analysed due to limited number of observations.
For the secondary endpoints successful reperfusion and excellent reperfusion, a sensitivity analysis was conducted in which patients with a missing final two-directional DSA run were excluded.
In the multivariable analyses, results were adjusted for age, a medical history of atrial fibrillation and previous stroke, use of anticoagulation, NIHSS score at baseline, collateral score, intravenous thrombolysis, procedural use of heparin and time from groin puncture to recanalisation or last contrast bolus. For the primary endpoint, an additional multivariable analysis was conducted in which we adjusted for the aforementioned covariables and the postprocedural reperfusion status (eTICI score on a categorical scale) in an attempt to further reduce the selection bias (we hypothesised that patients treated with IA thrombolytics who initially had a poor TICI score, were more likely to have a favourable outcome due to delayed reperfusion). In the subgroup analyses, we only adjusted for NIHSS score at baseline and time from groin puncture to recanalisation or last contrast bolus due to the limited sample size. The choice of the covariables was based on standard adjustments,24 and in addition on generally known associations related to stroke outcomes and significant differences that we found between the groups treated with and without local IA thrombolytics. Results of the logistic regression analyses were displayed as adjusted OR (aOR) with 95% CI.
Missing data were imputed using multiple imputations by chained equations. Statistical significance was set to p <0.05. Analyses were performed with SPSS Statistics V.23.0 software (IBM, Armonk, New York).
Results
In total, 3637 patients with acute ischaemic stroke were treated endovascularly in the Netherlands between March 2014 and November 2017. Of the 3180 patients who were included in the analysis of the MR CLEAN Registry, 2263 patients were eligible for inclusion in this study: 95 (4.2%) patients were treated with local IA thrombolytics and 2168 (96%) patients were treated without local IA thrombolytics (figure 1).

Flowchart of included patients. IA, intra-arterial; MR CLEAN, Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands; M3, middle cerebral artery, third segment; M4, middle cerebral artery, fourth segment; mRS, modified Rankin Scale; n, number. aEndovascularly was defined as arterial puncture in the angiography suite.
Baseline and procedural characteristics
Patients treated with local IA thrombolytics were younger, less likely to use anticoagulation, less often treated with a stent retriever or aspiration and had a longer duration from groin puncture to recanalisation or last contrast bolus. The number of revascularisation attempts, which included treatment with stent retrievers, aspiration or local IA thrombolytics, did not differ between patients treated with and without IA thrombolytics (table 1 and table 2).
Baseline characteristics
Procedural variables
The IA thrombolytics administered were urokinase (n=63/95 (66%)) or alteplase (n=32/95 (34%)), and the median doses were 250 000 IU (IQR, 1 93 750–2 50 000) and 20 mg (IQR, 12–20), respectively (table 2).
IA thrombolytics were administered more frequently as adjuvant than as primary revascularisation attempt (n=65/91 (71%) vs n=26/91 (29%)) and more frequently for proximal than for distal occlusions (n=67/88 (76%) vs n=21/88 (24%)). IA thrombolytics as primary revascularisation attempt were administered for both proximal (n=18/26, 69%) and distal (n=8/26, 31%) occlusions. For adjuvant revascularisation attempts, IA thrombolytics were also administered for both proximal (n=47/60, 78%) and distal (n=13/60, 22%) occlusions (online supplemental table S1).
Supplemental material
Outcome data
Primary endpoint
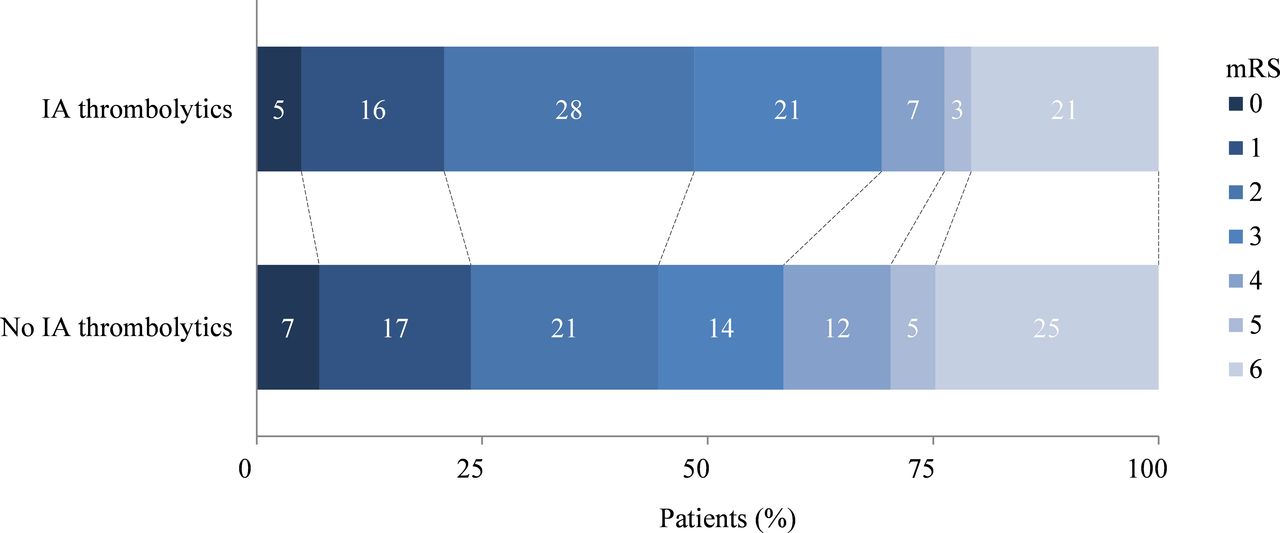
We observed comparable rates of favourable functional outcome between the groups treated with and without IA thrombolytics (49% vs 44%, respectively; OR, 1.18; 95% CI 0.78 to 1.80) (table 3, figure 2). After adjustments, no association was found between IA thrombolytics and favourable functional outcome (aOR, 1.16; 95% CI 0.71 to 1.90) (table 3). The direction of the results remained equal after additional adjustment for eTICI score (aOR, 1.31; 95% CI 0.79 to 2.19).
Secondary outcome variables
{kind=link}
{kind=link}
Distribution on the modified Rankin Scale. IA, intra-arterial; mRS, modified Rankin Scale.
There was no significant interaction between IA thrombolytics and intravenous thrombolysis related to favourable functional outcome (p=0.51) and between IA thrombolytics and procedural use of heparin related to favourable functional outcome (p=0.88) (online supplemental figure S1). IA thrombolytics were less often used in EVT procedures performed after January 2016 (n=53/1539 (3.4%] vs n=42/724 [5.8%]; p=<0.01). There was no significant interaction with IA thrombolytics related to favourable functional outcome (p=0.27) (online supplemental figure S1).
Secondary endpoints
Successful reperfusion was less often observed in patients treated with IA thrombolytics than in patients treated without (49% vs 67%, respectively; OR, 0.46; 95% CI 0.30 to 0.70; aOR, 0.57; 95% CI 0.36 to 0.90) (table 3). Compared with patients not treated with IA thrombolytics, the reperfusion status of patients treated with IA thrombolytics was numerically more often scored with a maximum eTICI score of 2A due to unavailability of a final anteroposterior or lateral DSA run (n=258/2135 (12%) vs n=17/92 (18%), respectively, p=0.07). Exclusion of those patients with a missing final two-directional DSA run did not change the direction of the results in both the unadjusted analysis (OR, 0.46; 95% CI 0.29 to 0.73) and adjusted analysis (aOR, 0.59; 95% CI 0.35 to 0.99).
Excellent reperfusion was also less often achieved in patients treated with IA thrombolytics than in patients treated without (32% vs 47%, respectively; OR, 0.54; 95% CI 0.35 to 0.85). In the adjusted analysis, the association between IA thrombolytics and excellent reperfusion did no longer exist (aOR, 0.68; 95% CI 0.43 to 1.09) (table 3). Exclusion of patients with a missing final two-directional DSA run did not change the directions of the results (OR, 0.58; 95% CI 0.36 to 0.93 and aOR, 0.74; 95% CI 0.45 to 1.21).
For patients treated with and without IA thrombolytics, the rates of early neurological recovery and sICH were comparable, and no associations were observed (table 3).
Subgroup analyses
Within the IA thrombolytics group, comparable proportions of favourable functional outcome (n=13/24 (54%) vs n=28/60 (47%), respectively; OR, 1.23; 95% CI 0.49 to 3.11) and successful reperfusion (n=10/26 (38%) vs n=35/63 (56%), respectively; OR, 0.51; 95% CI 0.20 to 1.29) were observed between patients who received IA thrombolytics as primary or adjuvant revascularisation attempt. Similarly for patients with a proximal or distal occlusion, the rate of favourable functional outcome was almost equal (n=30/63 (48%) and n=9/19 (47%), respectively; OR, 1.01; 95% CI 0.37 to 2.76).
In the adjusted analyses, no associations were found between IA thrombolytics as primary revascularisation attempt and favourable functional outcome (aOR, 0.83; 95% CI 0.30 to 2.33). Successful reperfusion was less often observed in patients treated with IA thrombolytics as primary revascularisation attempt than in those treated with IA thrombolytics as adjuvant revascularisation attempt (aOR, 0.34; 95% CI 0.12 to 0.95). Furthermore, there was no association between IA thrombolytics for distal occlusions and favourable functional outcome (aOR, 0.79; 95% CI 0.26 to 2.43) (online supplemental tables S2–S5).
Discussion
Local IA thrombolytics were rarely used in the MR CLEAN Registry. No statistical difference was detected between groups in the rate of favourable functional outcome or sICH. Patients whom required and underwent IA thrombolytics were patients less likely to achieve successful reperfusion.
Overall, IA thrombolytics were administered in 4.2% patients of the included patients, which was substantially lower compared with other observational studies (10%). This discrepancy could be the result of different preferences and experiences of the interventionists.
Based on the rationale behind administration of local IA thrombolytics, namely, improving recanalisation rates and microvascular reperfusion, one could have expected an association between IA thrombolytics and favourable functional outcome at 90 days after EVT. This hypothesis was neither confirmed by our primary analysis, nor in subgroup analyses on additional periprocedural treatment (use of intravenous thrombolysis and use of heparin), moment of treatment (EVT before or after January 2016), treatment approaches of local IA thrombolytics (primary or adjuvant revascularisation attempt) and indications for local IA thrombolytics (distal or proximal occlusion). Our results were consistent with a recently published meta-analysis, in which the use of local IA thrombolytics as adjuvant revascularisation attempt was not found to be associated with improved functional outcomes. Comparable to our study, the meta-analysis was only based on observational data, and, therefore, the results were considered to be inconclusive.20 In the CHOICE trial, the rate of favourable functional outcome (defined as mRS score of 0 or 1) was found to be higher in patients treated with than without IA alteplase (59.0% (n=36/61) vs 40.4% (n=21/52); adjusted risk difference, 18.4%; 95% CI 0.3% to 36.4%). The differences in functional outcome between our study and the CHOICE trial may be due to the location and size of the intracranial occlusions. In our study, for both primary and adjuvant revascularisation attempts, proximal occlusions more often constituted the target lesion. In the CHOICE trial, a positive treatment effect on functional outcome was particularly found in the subgroup of patients with an eTICI score of 2C or 3. Our study population may, therefore, have consisted of patients in whom clot removal was more difficult and treatment response to local IA thrombolytics was lower. Since the CHOICE trial only included patients with successful reperfusion and was terminated early due to implications of the COVID-19 pandemic, the results cannot be generalised to patients with incomplete reperfusion (eTICI scores of≤2B).29
Contrary to the supposed therapeutic effect of local IA thrombolytics on recanalisation, successful reperfusion (and excellent reperfusion in the unadjusted analysis) was less often achieved in patients treated with than in those treated without IA thrombolytics. This overall result could be due to the low rate of successful recanalisation among the subgroup of patients treated with IA thrombolytics as primary revascularisation attempt. Importantly, the inverse association between local IA thrombolytics and successful reperfusion did not translate into less favourable outcome. The discrepancy between the supposed effect of IA thrombolytics and our results suggests that the impaired recanalisation with local IA thrombolytics may be explained by other factors. First, we hypothesised that the reperfusion status of patients treated with IA thrombolytics might have been underestimated, as it was more often scored with a maximum eTICI score of 2A due to unavailability of a final two-directional DSA run. Our hypothesis was not confirmed, however, in the sensitivity analysis. Second, due to the non-randomised design, the local IA thrombolytics group may have consisted of patients with more ‘difficult’ procedures in whom successful reperfusion could not be achieved after intravenous thrombolysis or thrombectomy attempts. This latter argument may also hold for other observational studies, which predominantly showed comparable reperfusion rates between patients treated with and without IA thrombolytics as adjuvant revascularisation attempt.17 20–23
We did not find an association between IA thrombolytics and sICH, even though the majority of patients were previously treated with intravenous thrombolysis and procedure duration of EVT itself was longer. Previous studies focusing on IA thrombolytics as primary revascularisation attempt showed an increased risk of intracranial haemorrhages after administration of IA thrombolytics,2 30 while in most of the recent studies (focusing on IA thrombolytics as adjuvant revascularisation attempt), this association was no longer being observed.17 19–23 The comparable sICH rates that were found in recent studies, and also in our study, could be the result of the increased experience of interventionists and the more advanced devices in use today, reducing the risk of vessel wall injury. The influence of the type and dose of IA thrombolytics on sICH is unclear. In a meta-analysis of five randomised clinical trials, an increased risk of sICH was observed in patients treated with IA thrombolytics, whereas this was not found in any of the individual studies.30 The increased risk of sICH might be the result of the higher dose of IA thrombolytics used in some of the studies, however, its impact on the risk of sICH could not be reliably assessed due to the different eligibility criteria and protocols used.3 31 32
Our study has several limitations. First, results might have been affected by selection bias and confounding by indication as, due to the non-randomised, retrospective study design, no uniform protocol existed on the use of local IA thrombolytics, the type of thrombolytic agent and dose. The control group may therefore not have entirely matched the intervention group in terms of ‘difficulty’ of the EVT procedure and impossible or failed thrombectomy attempts (the latter was, however, not reflected in the number of revascularisation attempts). This could potentially have led to an underestimation of the rate of favourable functional outcome in patients treated with local IA thrombolytics. Second, for four patients, the exact revascularisation attempt of local IA thrombolytics was unknown. Moreover, for all patients, eTICI scores immediately before and after administration of IA thrombolytics were lacking. DSA images were, therefore, reassessed, but unfortunately, the exact timing of administration of IA thrombolytics, and consequently the eTICI scores before and after each attempt, could not be determined. Unavailability of the data hampered more accurate composition of the control group and determination of the precise effect of IA thrombolytics on reperfusion rates. Third, the effect of local IA thrombolytics on microvascular reperfusion status could not be assessed because the protocol of the MR CLEAN Registry did not include postprocedural perfusion imaging12 33 and/or transcranial Doppler.34 Fourth, although we did our best efforts to minimise missing data on the treatment with local IA thrombolytics, 124 patients had to be excluded, which may have biased the results in unpredictable ways and influenced the precision of the effect estimates. Final, some of the secondary endpoints could not be analysed separately for patients treated with IA thrombolytics as primary versus adjuvant recanalisation attempt and for a distal versus proximal occlusion due to small sample sizes. Also, the effect of the type and dose of thrombolytic agents could not be studied due to small sample sizes. Furthermore, as the underlying reasons to administer local IA thrombolytics were not reported in the MR CLEAN Registry, we could only hypothesise on the indications. These limited data may have hampered an in-depth understanding of the results.
Conclusion
Local IA thrombolytics were rarely used in the MR CLEAN Registry. In the relatively small study sample, no statistical difference was observed between groups in the rate of favourable functional outcome or sICH. Patients whom required and underwent IA thrombolytics were patients less likely to achieve successful reperfusion, probably due to selection bias.
Data availability statement
No data are available.
Data availability statement
Data will not be made available to other researchers as no patient approval has been obtained for sharing data. Syntax files will be made available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The medical ethics committee of the Erasmus University Medical Centre Rotterdam in the Netherlands evaluated the study and granted permission to carry out the study as an observational registry (MEC-2014-235). Participants gave informed consent to participate in the study before taking part.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators We would like to thank the MR CLEAN Registry Investigators —group authors (Supplemental Appendix).
Contributors SLC, RPHB, AM and MU contributed to the study conception and design. Data acquisition, analysis or interpretation were performed by all authors. The first draft of the manuscript was written by SLC, AM, RPHB and MU and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. Guarantor: SLC.
Funding The MR CLEAN Registry was partly funded by Toegepast Wetenschappelijk Instituut voor Neuromodulatie (TWIN) Foundation, Erasmus MC University Medical Centre, Maastricht University Medical Centre, and Amsterdam University Medical Centre.
Competing interests Amsterdam University Medical Centre received funds from Stryker® for consultations by Prof. Dr. Majoie, Prof. Dr. Roos, and Drs. Berkhemer. Maastricht University Medical Centre received funds from Stryker® and Codman® for consultations by Prof. Dr. Van Zwam. Prof. Dr. Majoie: Related: Grants TWIN Foundation; Unrelated: Grants from CVON/Dutch Heart Foundation, Stryker, European Commission, TWIN Foundation, Health Evaluation Netherlands (all paid to institution); shareholder of Nico-lab, a company that focuses on the use of artificial intelligence for medical image analysis (modest). The other authors report no conflicts.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.