Article Text

Abstract
Introduction Current guidelines recommend blood pressure (BP) lowering in patients after acute intracerebral haemorrhage (ICH) without guidance on initial choice of antihypertensive class. This study sought to determine if initial antihypertensive class differentially effects acute BP lowering in a large multiethnic ICH cohort.
Methods Subjects enrolled in the Ethnic/Racial Variations in ICH study between August 2010 and August 2017 with elevated admission BP and who received labetalol, nicardipine or hydralazine monotherapy as initial antihypertensive were analysed. Primary outcomes were systolic and diastolic BP changes from baseline to first BP measurement after initial antihypertensive treatment. Secondary outcomes included haematoma expansion (HE), hospital length of stay (LOS) and modified Rankin Score (mRS) up to 12 months after ICH. Exploratory outcomes assessed effects of race/ethnicity. Linear and logistic regression analyses, adjusted for relevant covariates, were performed to determine associations of antihypertensive class with outcomes.
Results In total, 1156 cases were used in analyses. Antihypertensive class was associated with diastolic BP change (p=0.003), but not systolic BP change (p=0.419). Initial dosing with nicardipine lowered acute diastolic BP than labetalol (least square mean difference (labetalol-nicardipine)=5.47 (2.37, 8.57), p<0.001). Initial antihypertensive class was also found to be associated with LOS (p=0.028), but not with HE (p=0.406), mortality (p=0.118), discharge disposition (p=0.083) or mRS score at discharge, 3, 6 and 12 months follow-up (p=0.262, 0.276, 0.152 and 0.36, respectively). Race/ethnicity variably affected multivariable models.
Conclusion In this large acute ICH cohort, initial antihypertensive class was associated with acute diastolic, but not systolic, BP-lowering suggesting differential effects of antihypertensive agents.
Trial registration number NCT01202864.
- Blood Pressure
- Hemorrhage
- Intervention
Data availability statement
Data are available in a public, open access repository. All de-identified subject data are available in a publicly accessible database maintained at Wake Forest University available through data access approval by the University of Cincinnati.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key message
What is already known on this topic
For patients suffering from acute intracerebral haemorrhage (ICH) with initial systolic blood pressure greater than 150 mm Hg, the American Heart Association/American Stroke Association recommends reduction to below 140 mm Hg. However, no available data indicate which antihypertensive class might be most efficacious.
What this study adds
Initial choice of antihypertensive agent differentially effects immediate diastolic, but not systolic, blood pressure reduction in patients presenting with acute ICH, with nicardipine appearing to be more efficacious than labetalol.
How this study might affect research, practice or policy
While this study cannot advise on longer-term effects of initial antihypertensive choice after ICH, these results suggest that optimisation of patient-specific blood pressure therapy may be warranted through future real-world evidence or prospective clinical trials.
Introduction
Spontaneous, non-traumatic intracerebral haemorrhage (ICH) is a devastating neurological disease with no proven treatment, accounting only for 10%–15% of all strokes, but 50% of stroke-related mortality.1 2 ICH prognosis remains poor with high mortality at 30 days3 and 16-year cumulative survival of around 3% for men and 10% for women.4 An effective treatment of ICH continues to be an important area of active research with promise for future successful therapeutic interventions.
For ICH patients with an initial systolic blood pressure (SBP) of 150–220 mm Hg, and without other contraindications to SBP lowering, the American Heart Association/American Stroke Association (AHA/ASA) guideline recommends that acute reduction of SBP to below 140 mm Hg.5 High SBP is associated with early neurological deterioration, greater haematoma expansion (HE), worse clinical outcome, acute kidney injury6 and death.7–9 The degree and speed of BP reduction may depend on antihypertensive class. However, no available data indicate which antihypertensive class might be most efficacious in treating acute ICH patients.
This study seeks to address this question using a large, multiethnic cohort of ICH patients. Our hypothesis was that class of antihypertensive agent differentially affects immediate BP reduction after acute ICH in a large, multiethnic cohort. The primary aim was to identify associations between antihypertensive medication class and differential immediate BP response after acute ICH. Secondary aims were to determine associations of antihypertensive class with clinical outcomes, including HE, survival and neurological recovery. Exploratory aims examined associations of antihypertensive class with outcomes in different race/ethnicity groups.
Materials and methods
Study population
Subjects were previously enrolled as part of the ERICH Study,10 11 a multicentre, prospectively recruited ICH case–control study that enrolled 3000 ICH cases between August 2010 and August 2017. For this study, inclusion criteria included diagnosis of spontaneous, primary ICH and aged 18 years or older. Warfarin-associated ICH and peripartum ICH were included, but secondary aetiologies such as trauma, transformation of cerebral infarction, tumour-associated, dural venous sinus thrombosis, aneurysm, vascular malformation and malignancies leading to coagulopathy were excluded. Due to frequent use of labetalol, nicardipine and hydralazine as first-line intravenous agents in the ERICH study, individuals treated with other antihypertensive agents, treated with multiple antihypertensive agents, or with missing dose documentation were excluded. Only patients admitted through the enrolling hospital’s emergency departments were included, thereby avoiding variability instilled by outside hospital transfers. Finally, all patients undergoing surgical procedure for haematoma evacuation or hemicraniectomy were excluded. Finally, the study did not proscribe an intervention strategy, so each site practised according to contemporary medical practice, following AHA guidelines at the time. Of the 3000 participants recruited into the original ERICH study, 1156 participants (figure 1) were identified who were administered an antihypertensive agent of interest in the emergency department with available premedication and post medication administration BP readings.

CONSORT diagram. CONSORT, Consolidated Standards of Reporting Trials; ICH, intracerebral haemorrhage.
Collected variables
Demographic and baseline data from each subject were obtained via chart abstraction, including age, body mass index (BMI) at admission, sex, race/ethnicity, medical history and substance abuse (table 1). Heavy alcohol use was defined as consumption of more than 2 servings of alcohol per day. Information on previous cocaine use was obtained from subject/family interview. Clinical data related to the ICH event, namely, haematoma location, name and dose of first antihypertensive agent administered, BP immediately prior to and within an hour of antihypertensive administration, and time between antihypertensive administration and BP measurement. Following contemporary ICH guidelines and best practice, BP measurements were taken approximately 15 min after antihypertensive administration with automated entry into the electronic medical record.
Subject demographics and baseline characteristics compared among three antihypertensive groups
Antihypertensive exposure
Labetalol, nicardipine and hydralazine were selected for analyses as the three the most common used intravenous agents in our sample population. The focus was on intravenous monotherapy because clinicians must choose a single intravenous agent to initiate BP reduction in the acute ICH setting; analyses of monotherapy provided clearly interpretable results; and cohorts of patients exposed to other antihypertensives or overlapping therapies became quite small. Antihypertensive agents were administered via intravenous bolus immediately after measurement of baseline BP. Cumulative dose of antihypertensive administered was calculated until the first subsequent BP reading after initial dosing.
Outcomes
The primary aim was to identify associations between antihypertensive medication class and differential immediate BP response after acute ICH. The primary outcomes were change in SBP and diastolic BP (DBP) between initial BP measurement on hospital admission and first subsequent BP reading after initial administration of one of the three selected antihypertensive medication. Secondary outcomes included HE and 6 month mortality. Secondary aims were to determine associations of antihypertensive class with clinical outcomes, including HE, survival and neurological recovery. Secondary outcomes included hospital length of stay (LOS), modified Rankin Scale (mRS) at hospital discharge, 3, 6 and 12 months post-ICH and discharge disposition. Discharge disposition and mRS at discharge were obtained from discharge summaries. Surviving subjects were contacted at follow-up intervals by study personnel certified for administering outcome scales.12 mRS was dichotomised for analyses, with mRS ≤3 representing favourable outcome and mRS >3 representing unfavourable outcome. Subject disposition was classified as discharge home (ie, to own home, care of relative or friend, or rehabilitation centre) or discharge to facility (ie, to skilled nursing home, assisted living, hospital or acute setting). Exploratory aims examined associations of antihypertensive class with primary and secondary outcomes in different race/ethnicity groups.
Imaging
The initial CT images for each subject was reviewed to confirm diagnosis of spontaneous ICH by site investigator and central imaging core neuroradiologist. Planimetric analysis using Alice software (Parexel, Waltham, Massachusetts, USA) was employed to measure haematoma volumes, previously reported to have exceptional inter-rater reliability.13 HE was defined as >33% increase in haematoma volume from diagnostic CT to next subsequent CT imaging within 72 hours after ICH onset. Haematoma location was dichotomised into lobar and non-lobar.
Statistical analyses
Subjects were divided into three groups according to the initial antihypertensive agent administered on presentation to the emergency department. For comparisons of cohorts grouped by antihypertensive class without adjustment for covariates, Kruskal-Wallis test was used to compare continuous variables and χ2 test for the categorical variables. To estimate association of antihypertensives with outcomes, multivariable linear regression was performed for continuous outcomes (SBP, DBP, HE and LOS), while multiple logistic regression was performed for binary outcomes (mortality, mRS at specific time points, and disposition). Covariates adjusted in the above multiple linear/logistic regression models include race/ethnicity, age, BMI, dose of the first antihypertensive agent given, time difference between antihypertensive agent administration and measurement of BP, sex, prior history of stroke, hypertension, diabetes mellitus, cigarette use, heavy alcohol use or cocaine use, premorbid mRS, history of antihypertensive use and volume and location of ICH. To examine associations of outcomes and antihypertensive class depending on race/ethnicity, multiple linear/logistic regression models stratified by race/ethnicity was conducted in order to examine the associations of the outcomes and the antihypertensive class separately in each race/ethnicity group. For sensitivity analysis, we also fit the multiple linear/logistic regression models adjusted for the above set of covariates plus interaction term of antihypertensive class and race/ethnicity. Analyses for this study were performed using the SAS software V.9.4.
Results
The antihypertensive agent administered acutely after ICH was hydralazine in 71 subjects (6.14%), labetalol in 415 subjects (35.90%), and nicardipine in 670 subjects (57.96%). Demographic characteristics of the study subjects are summarised in table 1, and crude outcomes, categorised by antihypertensive agent, are summarised in table 2. Time from ICH onset to administration of first antihypertensive agent was less than 6 hours in 72.75% of the cohort with 81.46% in total receiving initial antihypertensive therapy within 12 hours. The mean time difference between antihypertensive agent administration and BP measurement was 17.4±14.5 min across all three antihypertensive groups. The baseline characteristics of subjects in all three groups of antihypertensive agents were similar. SBP change was not different among three antihypertensive groups (p=0.730), but DBP change was significantly different (p=0.002). Secondary and exploratory outcomes were also not different among three antihypertensive groups except for LOS (p=0.004).
Outcomes compared across three antihypertensive groups
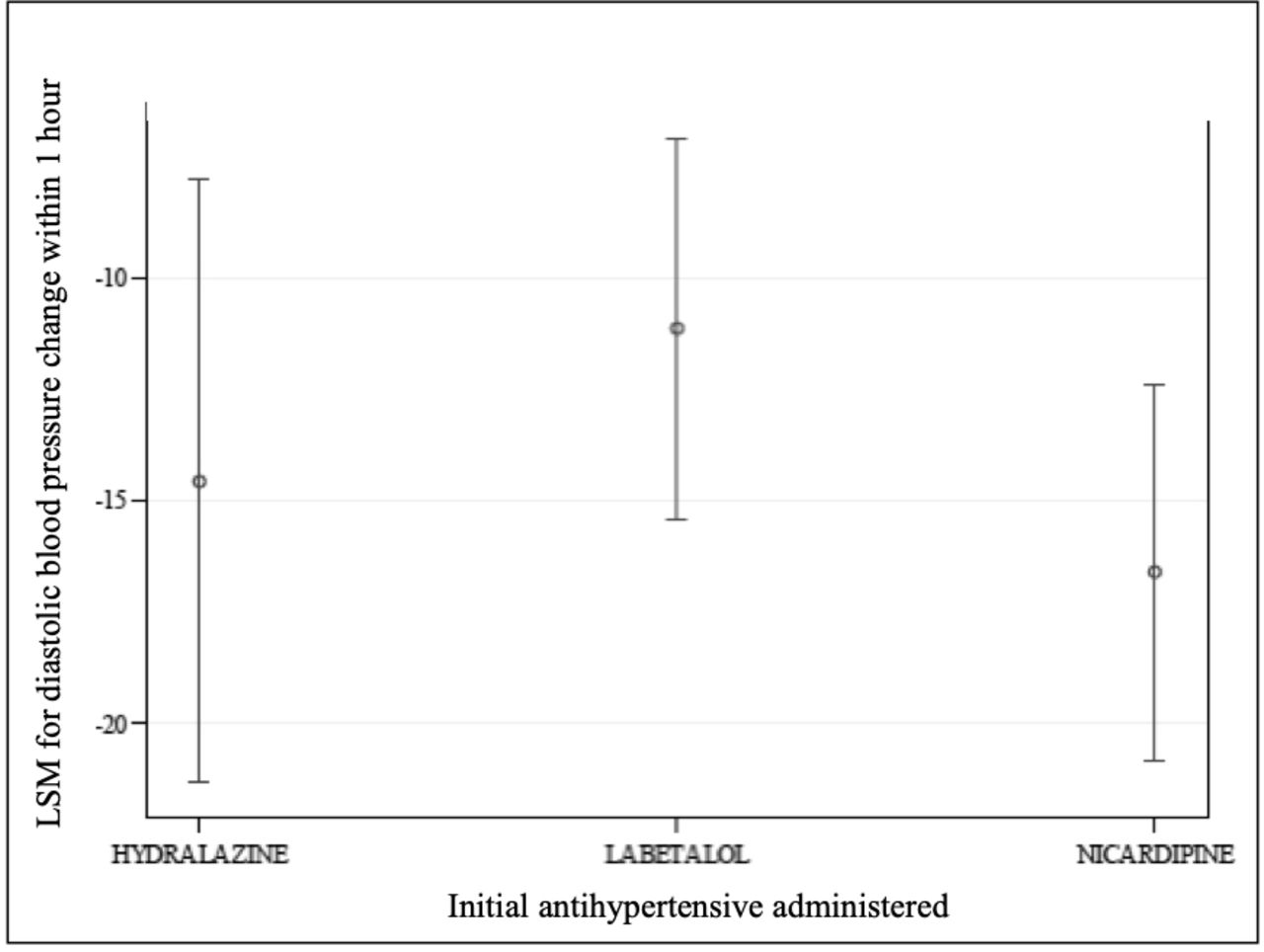
Linear regression models adjusted for covariates found no significant difference in antihypertensive medication class for the primary outcome of change in SBP. However, significant difference in DBP change (table 3) among antihypertensive medication classes was found, particularly between labetalol and nicardipine, where nicardipine could lower initial DBP to a greater extent than labetalol (figure 2). A sensitivity analysis for SBP and DBP using a cohort that excluded infratentorial haemorrhage cases was performed and did not alter the findings. Antihypertensive class was also found to be differentially associated with LOS (p=0.028; online supplemental table 1), particularly between labetalol and nicardipine (p=0.008; least square mean difference (labetalol-nicardipine)=−3.39 (–5.87, –0.90)), with nicardipine associated with shorter LOS. No association was found between antihypertensive class and other secondary outcomes including HE (p=0.406), mortality (p=0.118), mRS at time of discharge, 3, 6 and 12 months follow ups (p=0.262, 0.276, 0.152 and 0.36, respectively), or discharge disposition (p=0.083; online supplemental table 1).
Supplemental material
Multiple linear regression models of primary outcomes of mean change in systolic or diastolic blood pressure (SBP/DBP) from antihypertensive administration to first subsequent blood pressure measurement, adjusted

{kind=link}
{kind=link}
Least square means (LSM) diastolic blood pressure change within 1 hour of antihypertensive use, adjusted for covariates.
The ERICH study was specifically designed to study racial/ethnic differences in ICH. In regression models for primary and secondary outcomes race/ethnicity was included as a covariate. Race/ethnicity had a statistically significant effect on SBP (p<0.001) and DBP (p=0.036) changes (table 4) but no associations with secondary outcomes. In exploratory analyses, regression models were stratified by race/ethnicity. In stratified models, antihypertensive class was associated with DBP change in blacks (p=0.046), but not Hispanics (p=0.134) or whites (p=0.550), particularly between labetalol and nicardipine (p=0.013; least square mean difference (labetalol-nicardipine)=7.54 (1.58, 13.50)), where nicardipine lowered DBP more than labetalol. Associations were also found between antihypertensive class and LOS, disposition, 6-month mortality and mRS when stratified by race/ethnicity (online supplemental table 2). However, sensitivity analyses, using regression models with interaction term of antihypertensive class and race/ethnicity, found no association between the interaction term and any outcome.
Multiple linear regression models of different race/ethnicities for primary outcomes of mean change in systolic or diastolic blood pressure (SBP/DBP) from antihypertensive administration to first subsequent blood pressure measurement, adjusted for covariates
Discussion
In this large, multiethnic cohort, initial antihypertensive agent class is not associated with differences in initial SBP reduction after acute ICH or with subsequent clinical outcomes, but it is associated with initial DBP reduction. Physiologically, lowering BP may ameliorate acute ICH pathophysiology such as HE and perihaematomal oedema formation. AHA/ASA guidelines currently recommend SBP lowering to below 140 mm Hg.5 Lack of association with antihypertensive class and SBP reduction in acute ICH is consistent with these guidelines in which no specific antihypertensive agent is recommended. At present, antihypertensive medication after acute ICH should be selected by considering pharmacological profile, potential side effects, cost and practicability.
Clinical ICH trials have targeted SBP for treatment based on the evidence in the literature suggesting an association between SBP and HE.14 15 However, our results demonstrated that the choice of initial antihypertensive agent was associated with a significant difference in DBP, not SBP. Effects on clinical outcome post-ICH for BP parameters other than SBP, such as DBP, pulse pressure and heart rate, remain mostly unstudied. Elevated DBP has been related to end-organ damage16 and implicated as a strong predictor of cardiovascular disease in people under 50 years of age.17 Recent research by Chang et al 18 found that widened pulse pressure, that is, the difference between SBP and DBP, was an independent predictor of increased mortality in ICH. Small vessels in the brain may be damaged by the elevated pressure pulse-wave, leading to cerebrovascular morbidity and mortality.19 20 Failure of acute BP lowering to improve clinical outcome in ICH may be related to oversimplification of SBP as the primary variable of interest. As such, given the present investigation and related findings as discussed above, studies regarding the implication of DBP control after ICH might be considered.
The ERICH study was specifically designed to address racial/ethnic disparities and differences in ICH. Racial/ethnic differences in hypertension and the chronic effects of antihypertensive medications are well known.21 However, differential antihypertensive effects after acute ICH have not been described. Thus, this study sought to explore possible associations between common antihypertensive agents, race/ethnicity and early effects after acute ICH. In this study, race/ethnicity affected associations between antihypertensive agents with SBP and DBP change but lacked associations with secondary clinical outcomes. To evaluate possible effects of race/ethnicity on antihypertensive therapy after acute ICH, not only was race-ethnicity included in multiple regression models, but also examined interaction effects of race-ethnicity and antihypertensive agent were examined, multiple regression models stratified by race-ethnicity were explored. Notably, associations of antihypertensive class and DBP was found in blacks, especially for labetalol versus nicardipine. Several other potentially significant associations were discovered, but these findings were highly exploratory and true relationships remain unclear, especially given the lack of significant interaction effect of race/ethnicity and antihypertensive agent for primary and secondary outcomes. Overall, race/ethnicity may be an important covariate for antihypertensive effects after acute ICH, but further research is required to evaluate these associations more fully.
As one of the largest acute ICH samples (N=1156), this study has adequate power to detect differences in HE among the antihypertensive agents, especially for nicardipine (N=670) and labetalol (N=415). Few missing data for secondary and exploratory outcomes and low lost to follow-up for mRS and survival-mortality provide further reassurance of validity of findings and avoidance of bias. However, the study cannot address effects of subsequent antihypertensive taken during and after hospitalisation22 or changes in potentially relevant variables, such as creatinine or other serological profiles over time. Patient recruitment was similar across each race/ethnicity for the three antihypertensive agents allowing for exploratory analyses. However, route and dosing regimen of administration of antihypertensive medications across all subjects could not be standardised, which affects pharmacokinetics.23 Thus, comparison of doses across subjects cannot be considered 1:1 equivalent.24 Initial antihypertensive agents were analysed without including subsequent other antihypertensive agents, and despite the large sample, testing interactions beyond the three classes of agents was not possible. In particular, the sample size of subjects on hydralazine was relatively small, and clevidipine use was not in widespread use when this cohort was assembled. Further, initial National Institutes of Health Stroke Scale scores were not captured in the parent ERICH study and not available for inclusion in models. Thus, parsing out which specific antihypertensive class is most efficacious in each race/ethnicity or other patient-specific factors25 is beyond the limits of this study, and would require a much larger sample from a prospectively collected cohort or specific clinical trial. Treatment of patients in this cohort with other antihypertensives in the prehospital setting remains a possible confounder. The baseline CT and initial dose of antihypertensive treatment was more than 3 hours after symptoms onset for some patients, but maximal HE may occur as early as the first 3 hours after ICH onset.26 Also, HE was identified using imaging within the following 72 hours after ICH onset, though substantive clot retraction is unlikely during that time period. Finally, the present analyses may be confounded by BP changes that would naturally occur in the acute ICH setting.
Conclusion
Initial choice of antihypertensive agent differentially effects immediate DBP reduction, but not SBP reduction, in patients presenting with acute ICH, with nicardipine appearing to be more efficacious than labetalol. While this study cannot advise on longer-term effects of initial antihypertensive choice after ICH, future prospective, real-word evidence trials would be required, if warranted, to optimise patient-specific initial BP therapy.
Data availability statement
Data are available in a public, open access repository. All de-identified subject data are available in a publicly accessible database maintained at Wake Forest University available through data access approval by the University of Cincinnati.
Ethics statements
Patient consent for publication
Ethics approval
The Ethnic/Racial Variations of Intracerebral Haemorrhage (principal investigator: DW, MD, Grant: U01-NS069763-05) data and analyses presented in this manuscript are based on the research files downloaded from the Archived Clinical Research web site.11 Prior to commencement of study enrolment, Institutional Review Board approval at the contributing centres to the Ethnic/Racial Variations of Intracerebral Haemorrhage and informed consent from the patient or legal authorised representative were obtained.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Shree_Stroke, @mlukej
Contributors YN, substantial contributions to conception and design of the work, acquisition and interpretation of data, drafting the work and revising it critically for important intellectual content; WQ - substantial contributions to conception and design of the work, analysis and interpretation of data, drafting the work and revising it critically for important intellectual content; NKKK - substantial contributions to conception and design of the work, interpretation of data, drafting the work and revising it critically for important intellectual content; TC - substantial contributions to conception and design of the work, interpretation of data, drafting the work and revising it critically for important intellectual content; VK - substantial contributions to conception and design of the work, interpretation of data, drafting the work and revising it critically for important intellectual content; SS - substantial contributions to conception and design of the work, interpretation of data, drafting the work and revising it critically for important intellectual content; AD - substantial contributions to interpretation of data, drafting the work and revising it critically for important intellectual content; MB - substantial contributions to interpretation of data, drafting the work and revising it critically for important intellectual content; ERC - substantial contributions to interpretation of data, drafting the work and revising it critically for important intellectual content; MLF - substantial contributions to interpretation of data, drafting the work and revising it critically for important intellectual content; KBW - substantial contributions to acquisition and interpretation of data, drafting the work and revising it critically for important intellectual content; FDT - substantial contributions to acquisition and interpretation of data, drafting the work and revising it critically for important intellectual content; JLM - substantial contributions to acquisition and interpretation of data, drafting the work and revising it critically for important intellectual content; LAG - substantial contributions to conception and design of the work, acquisition and interpretation of data, drafting the work and revising it critically for important intellectual content; CDL - substantial contributions to conception and design of the work, acquisition, analysis and interpretation of data, drafting the work and revising it critically for important intellectual content; TPB - substantial contributions to conception and design of the work, acquisition and interpretation of data, drafting the work and revising it critically for important intellectual content; DW - substantial contributions to conception and design of the work, acquisition and interpretation of data, drafting the work and revising it critically for important intellectual content; MLJ - substantial contributions to conception and design of the work, acquisition and interpretation of data, drafting the work and revising it critically for important intellectual content, and acts as guarantor of the work. All the listed authors have offered final approval of the version published. Further all authors have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was funded by the NIH/NINDS U01-NS069763-05 (D.W.).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.