Article Text

Abstract
Background Stroke after acute coronary syndrome (ACS) can be devastating. It is uncertain whether the risks of ischaemic stroke or intracranial haemorrhage (ICH) are associated with different choices of P2Y12 inhibitors (potent P2Y12 inhibitors such as ticagrelor and prasugrel vs clopidogrel). Even though East Asians are known to have different thrombotic and haemorrhagic profiles from Caucasians, data on Chinese patients are sparse.
Method This was a retrospective cohort study conducting in Chinese patients with ACS who underwent first-ever percutaneous coronary intervention from 14 hospitals in Hong Kong between 2010 and 2017. The primary efficacy endpoint was ischaemic stroke. The secondary efficacy endpoint was a composite outcome of thrombotic events including all-cause mortality, non-fatal myocardial infarction and ischaemic stroke. The primary safety endpoint was ICH. The secondary safety endpoint was a composite of major bleeding events.
Results After adjustment of baseline characteristics by 1:1 propensity score matching, a total of 6220 patients (3110 on each group) were analysed. Compared with clopidogrel, potent P2Y12 inhibitors were associated with a lower risk of ischaemic stroke (HR 0.57; 95% CI 0.37 to 0.87; p=0.008) and a lower risk of thrombotic events (HR 0.77; 95% CI 0.66 to 0.90; p=0.001). Potent P2Y12 inhibitor was associated with similar risk of ICH (HR 0.65; 95% CI 0.34 to 1.25, p=0.20) and major bleeding (HR 0.83; 95% CI 0.68 to 1.01, p=0.069).
Conclusions Potent P2Y12 inhibitors were associated with a lower adjusted risk of ischaemic stroke and thrombotic events, compared with clopidogrel. The risks of ICH and major bleeding were similar.
- stroke
- cerebral infarction
- cerebrovascular disorders
- hemorrhage
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
WHAT IS ALREADY KNOWN ON THIS TOPIC?
Potent P2Y12 inhibitors may reduce ischaemic stroke but at a cost of intracranial haemorrhage. Data in Asians including Chinese were sparse.
WHAT THIS STUDY ADDS?
Compared with clopidogrel, potent P2Y12 inhibitors were associated with a lower risk of ischaemic stroke and thrombotic events, without excess risks of intracranial haemorrhage or major bleeding.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY?
Chinese patients may benefit from potent P2Y12 inhibitors with regard to ischaemic stroke prevention and without excess bleeding risk.
Background
Stroke occurs in 1%–4% patients within the first year after acute coronary syndrome (ACS).1 2 Patients with stroke after ACS have a high mortality rate up to 36%, and nearly 60% of the remaining survivors had poor functional outcomes.3 4 It is important to identify effective secondary prevention to reduce the occurrence of stroke after ACS.
Dual‐antiplatelet therapy involving aspirin and a P2Y12 inhibitor is the standard antithrombotic therapy in patients with ACS.5 Potent P2Y12 inhibitors, ticagrelor and prasugrel, can achieve more pronounced platelet inhibition and reduce major adverse cardiac events (MACE) compared with clopidogrel in patients with ACS.1 6 They became the preferred choice over clopidogrel in most patients with ACS according to American and European guidelines.7 8 However, their protective effects on stroke prevention is less obvious. For example, the PLATelet inhibition and patient Outcomes trial showed that ticagrelor reduced individual endpoint of vascular death and myocardial infarction (MI), but not stroke or ischaemic stroke alone when compared with clopidogrel.1 The Trial to Assess Improvement in Therapeutic Outcomes by Optimising Platelet Inhibition with Prasugrel–Thrombolysis in Myocardial Infarction 38 showed that prasugrel reduced MI and stent thrombosis but not stroke when compared with clopidogrel.6 In contrast, a retrospective analysis found a reduction in subsequent ischaemic stroke with ticagrelor compared with clopidogrel in Swedish patients with ACS and a history of ischaemic stroke.9
East Asians have different thrombotic and bleeding profiles from White patients. Known as the East Asian Paradox, it describes the vulnerability to bleeding and resistance to ischaemic events of East Asian populations.10–12 Asians are observed to have a higher risks of intracranial haemorrhage (ICH) and cerebral microbleed,13–15 but a lower risk of MACE after percutaneous coronary intervention (PCI).16 This would argue in favour of clopidogrel use, since both ticagrelor and prasugrel have been linked to increase fatal ICH in certain subgroups.1 6 However, approximately 65% of East Asians carry a CYP2C19 loss-of-function allele and may result in impaired metabolic activation of clopidogrel,17 which is supportive of more liberal use of potent P2Y12 inhibitors. Even though East Asians are the largest ethnic group with a population more than 1.5 billion, they was represented in less than 4% in the landmark randomised controlled trials (RCTs).1 6 18 In the few East Asian RCTs and registries with smaller sample sizes, inconsistent results were shown.19–24 Their interpretation can also be confusing since some of these studies condensed ischaemic and haemorrhagic stroke as separate endpoints.
Currently, there are no data to compare the effect of different P2Y12 inhibitors with regard to ischaemic and haemorrhagic stroke in East Asians. Therefore, our aim is to determine the comparative risks of ischaemic and thrombotic stroke in Chinese patients with ACS treated with potent P2Y12 inhibitors or clopidogrel after PCI.
Methods
Study population and design
Data from all patients who underwent first-ever PCI between 1 January 2004 and 31 December 2017 from all 14 public hospitals that performed PCI and recorded in a territory-wide PCI registry were reviewed. Patients baseline characteristics, exposures and outcomes were retrieved from the PCI Registry and Clinical Data and Analysis Reporting System.
We included all adult patients (18 years of age or older) of Chinese ethnicity, who underwent first-ever PCI performed for ACS and survived beyond hospital discharge. Patients were excluded if they are not prescribed on any P2Y12 inhibitor on discharge or received concomitant anticoagulant on discharge.
Definitions of exposure and outcome variables
Patients were stratified according to the P2Y12 inhibitor (potent P2Y12 inhibitor, ie, ticagrelor or prasugrel, vs clopidogrel) prescribed on hospital discharge. No further cross-over was allowed after group assignment. Of note, intravenous form of P2Y12 inhibitor was not available in this locality. The primary efficacy endpoint was ischaemic stroke. The secondary efficacy endpoint was thrombotic events, defined as a composite outcome of all-cause mortality, non-fatal MI and ischaemic stroke. The primary safety endpoint was ICH. The secondary safety endpoint was a composite of major bleeding (MB) events. Major bleeding was defined as a composite of fatal bleeding event, bleeding that occurred in the critical sites (intracranial, intra-articular or intramuscular with compartment syndrome, intraocular, pericardial, retroperitoneal), bleeding necessitating transfusion, or bleeding that caused a drop in haemoglobin of ≥20 g/L, in accordance to the International Society on Thrombosis and Haemostasis.25 The diagnosis of clinical events were made by managing clinicians with verification on blood transfusion records and laboratory test findings.
Statistical analyses
All analyses were performed with prespecified endpoints and statistical methods. We constructed a propensity score that predicted the likelihood of potent P2Y12 inhibitors versus clopidogrel with variables selected a priori based on data in the published literature and biological plausibility: gender, age, tobacco use, diabetes mellitus, hypertension, dyslipidaemia, cerebrovascular disease, chronic obstructive pulmonary disease, peripheral vascular disease, previous MI, previous coronary arterial bypass grafting, previous heart failure, decompensated heart failure on presentation (New York Heart Association Class III or IV), atrial fibrillation, anaemia, PCI indication (ST elevation MI, non-ST elevation MI, unstable angina) and other medications on discharge (aspirin, beta blocker, angiotensin antagonist, statin).
The study cohort consisted of two comparison groups—‘potent P2Y12 inhibitor group’ and ‘clopidogrel group’—generated by 1:1 propensity-score-matching using a calliper of 0.2 times the SD of the logit of the propensity score. Unadjusted analyses were made using χ2 tests for categorical variables and Student’s t-test or Wilcoxon rank-sum tests for continuous variables. Kaplan-Meier survival curves were constructed for study groups.26 Cox proportional hazards regression was performed to evaluate the relationship between P2Y12 inhibitors and clinical outcomes as a time-to-first-event analysis until 365 days after index PCI.
Sensitivity analyses
First, we repeated the primary analysis using the same model except that outcomes were included from PCI until 30 days after cessation of P2Y12 inhibitors. Next, to assess any residual confounding by treatment selection, we performed falsification testing for the primary outcomes with landmark analysis at 30 days after cessation of P2Y12 inhibitors until 5 years after PCI, such that any residual difference would likely results from reflect residual confounding because patients were no longer exposed to the effect of P2Y12 inhibitor. Next, we included all patients before propensity score matching and repeated the primary analysis using Cox regression model, adjusting for the same set of covariates used to construct the propensity score. Next, we used multiple imputation with chained equations to address missing data and repeated the primary analysis on the entire cohort using the same Cox regression model.
Exploratory analyses
We studied the effect modification on the relationship between P2Y12 inhibitor and primary outcomes by predefined clinical variables, and introduced interaction terms to the Cox regression model. We also performed landmark analysis to explore the association between P2Y12 inhibitors and primary outcomes for the period 0–30 days and 30–365 days after PCI separately.
Data management and statistical analyses were performed in Stata software, V.16 (StataCorp). A two-tailed p<0.05 was considered statistically significant.
Results
Patients and characteristics
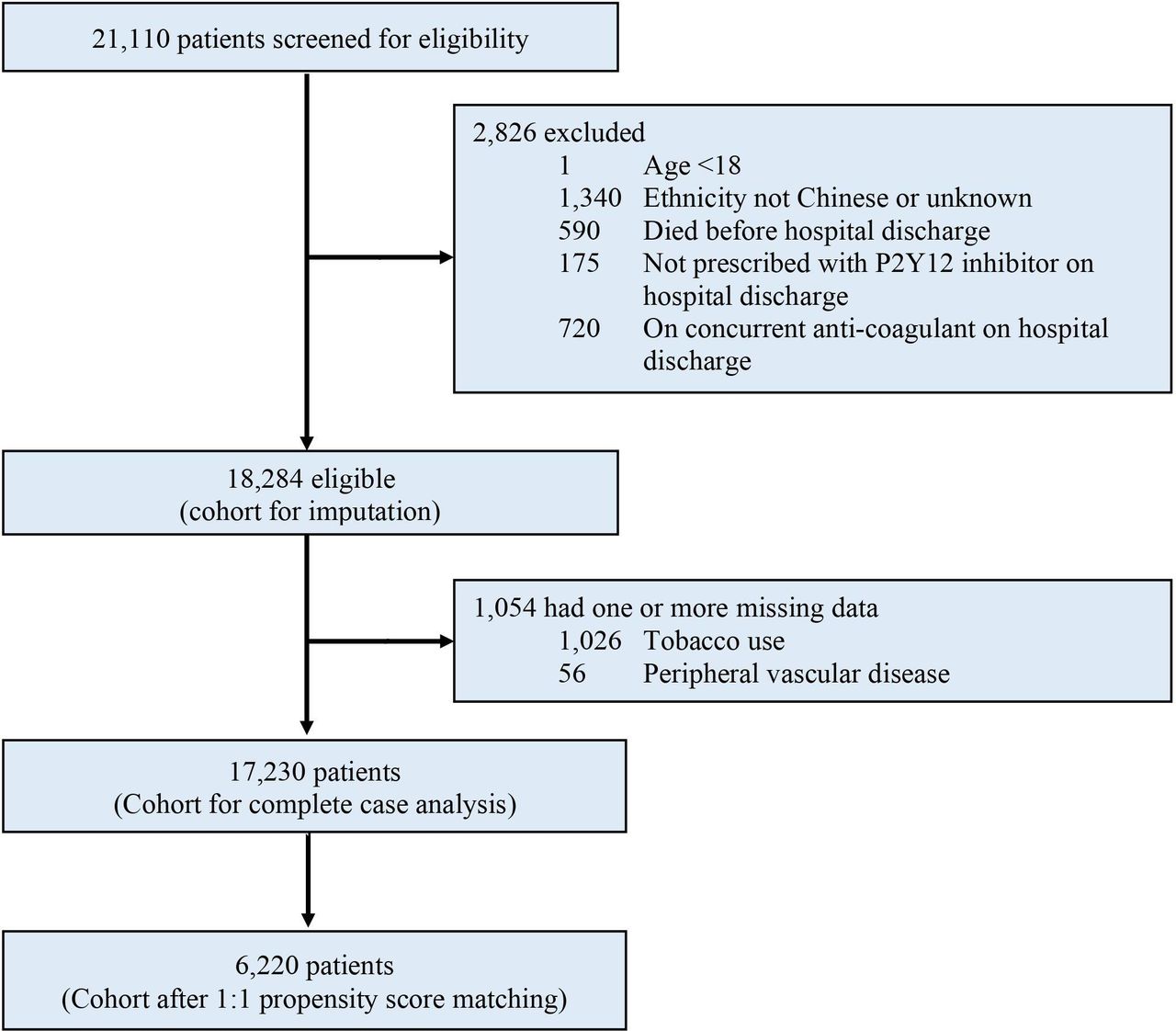
Between January 2010 and December 2017, a total of 21 110 patients were considered for inclusion: 2826 (13.4%) were excluded due to any of the following exclusion criteria—age younger than 18 years, ethnicity not Chinese or unknown, died before hospital discharge, not prescribed with P2Y12 inhibitor on hospital discharge, on concurrent anti-coagulant on hospital discharge. Of the remaining 18 284 patients analysed, a total of 1054 (5.8%) were excluded from the complete case analysis due to missing values in any of the variables used in the propensity score model (figure 1). Baseline characteristics of all patients before propensity score matching is shown in online supplemental appendix table S1). A total of 3110 pairs of patients prescribed on either potent P2Y12 inhibitor or clopidogrel at hospital discharge were generated by propensity score matching. The mean age was 61.5±11.7, in which 940 (15.1%) were women. The two groups were well balanced in the bassline characteristics with standardised differences <0.1 for all variables except for age >75, as shown in table 1. The two groups had similar duration of P2Y12 inhibitor use, but more patients in the potent P2Y12 inhibitor group transitioned to clopidogrel than vice versa. Details of P2Y12 inhibitor use were shown in online supplemental appendix table S2.
Supplemental material
Baseline characteristics of patient

Study profile.
Primary and secondary efficacy outcomes
In the propensity match cohort, the primary outcome of ischaemic stroke developed in 35 (1.13%) patients on potent P2Y12 inhibitors and in 61 (1.96%) patients on clopidogrel, corresponding to an annualised risk of 1.15% and 2.02%, respectively (HR 0.57; 95% CI 0.37 to 0.87; p=0.008) (table 2 and figure 2). The annualised risk of composite thrombotic events were lower in the potent P2Y12 inhibitor group than the clopidogrel group (HR 0.77; 95% CI 0.66 to 0.90; p=0.001) and so was the risk of MI (HR 0.71; 95% CI 0.59 to 0.87, p=0.001). The risk of all-cause mortality was similar across groups (HR 1.17; 95% CI 0.87 to 1.56; p=0.30).

Estimated probabilities of ischaemic stroke stratified by P2Y12 inhibitor. Potent P2Y12 inhibitor had a lower risk of ischaemic stroke than clopidogrel in the propensity score matched cohort. PCI, percutaneous coronary intervention.
Annualised risks and HRs of primary and secondary outcomes
Primary and secondary safety outcomes
The annualised risk of ICH was similar across both groups (HR 0.65; 95% CI 0.34 to 1.25, p=0.20) (table 2 and figure 3). Other major bleeding outcomes were also similar (table 2).

Estimated probabilities of intracranial haemorrhage stratified by P2Y12 inhibitor. Potent P2Y12 inhibitor and clopidogrel had a similar risk of intracranial haemorrhage in the propensity score matched cohort. PCI, percutaneous coronary intervention.
Sensitivity analyses
When outcomes were observed until 30 days after cessation of P2Y12 inhibitor, the risk of ischaemic stroke was lower in the potent P2Y12 inhibitor group (HR 0.57; 95% CI 0.38 to 0.86; p=0.007) and the risk of ICH was similar across groups (HR 0.71; 95% CI 0.37 to 1.38; p=0.31), consistent with the primary analysis.
Falsification testing with landmark analysis at 30 days after cessation of P2Y12 inhibitor showed that the risk of ischaemic stroke was similar across groups (HR 1.11; 95% CI 0.77 to 1.60; p=0.56), and so was the risk of ICH (HR 1.09; 95% CI 0.63 to 1.89; p=0.75), suggestive of no residual confounding.
We analysed the outcomes of all 17 230 patients with complete information before propensity score matching. The risk of ischaemic stroke was lower in the potent P2Y12 inhibitor group (HR 0.69; 95% CI 0.47 to 0.99; p=0.046) and the risk of ICH was similar across groups (HR 1.00; 95% CI 0.57 to 1.79; p=0.98), consistent with the primary analysis. Next, we analysed the outcomes of all 18 284 patients using multiple imputation with chained equations to address missing data. Their baseline characteristics were shown in online supplemental appendix table S1. The risk of ischaemic stroke was lower in the potent P2Y12 inhibitor group (HR 0.69; 95% CI 0.48 to 0.98; p=0.041) and the risk of ICH was similar across groups (HR 0.91; 95% CI 0.51 to 1.61; p=0.74), also consistent with the primary analysis.
Exploratory analyses
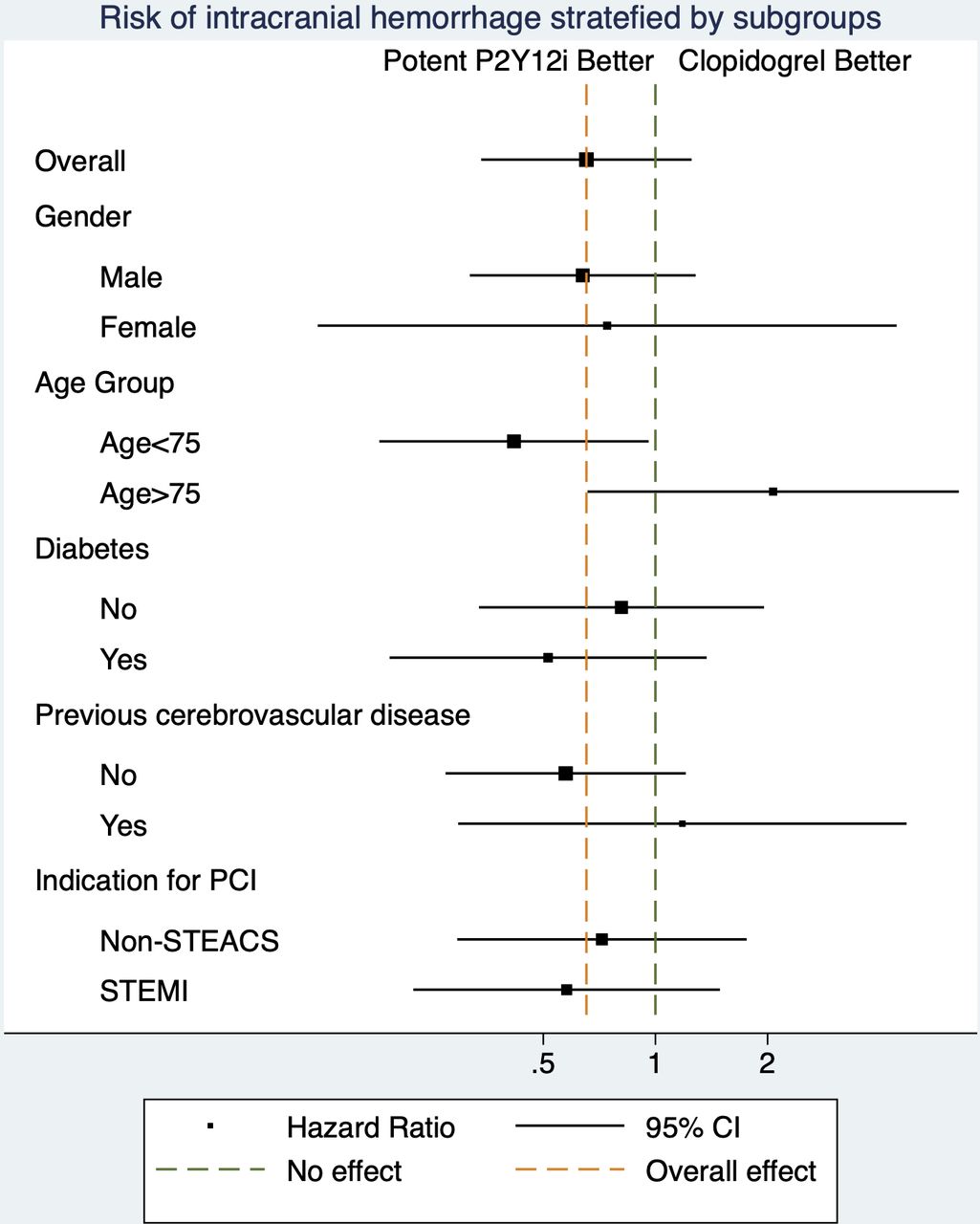
The association between P2Y12 inhibitors and ischaemic stroke was modified by gender, which female patients had less benefit with potent P2Y12 inhibitor (table 3 and figures 4–5). The association between P2Y12 inhibitors and ICH was modified by age group. In landmark analysis, potent P2Y12 inhibitors were associated with similar risk of ischaemic stroke between 0 and 30 days after PCI (HR 0.58, 95% CI 0.28 to 1.21, p=0.15) and a lower risk between 30 to 365 days after PCI (HR 0.57, 95% CI 0.34 to 0.94, p=0.028). Potent P2Y12 inhibitors were associated with similar risk of ICH between 0 and 30 days after (HR 0.12, 95% CI 0.02 to 1.00, p=0.05) and between 30 and 365 days after PCI (HR 0.93, 95% CI 0.45 to 1.94, p=0.86).
Subgroup analysis for primary efficacy and safety outcomes
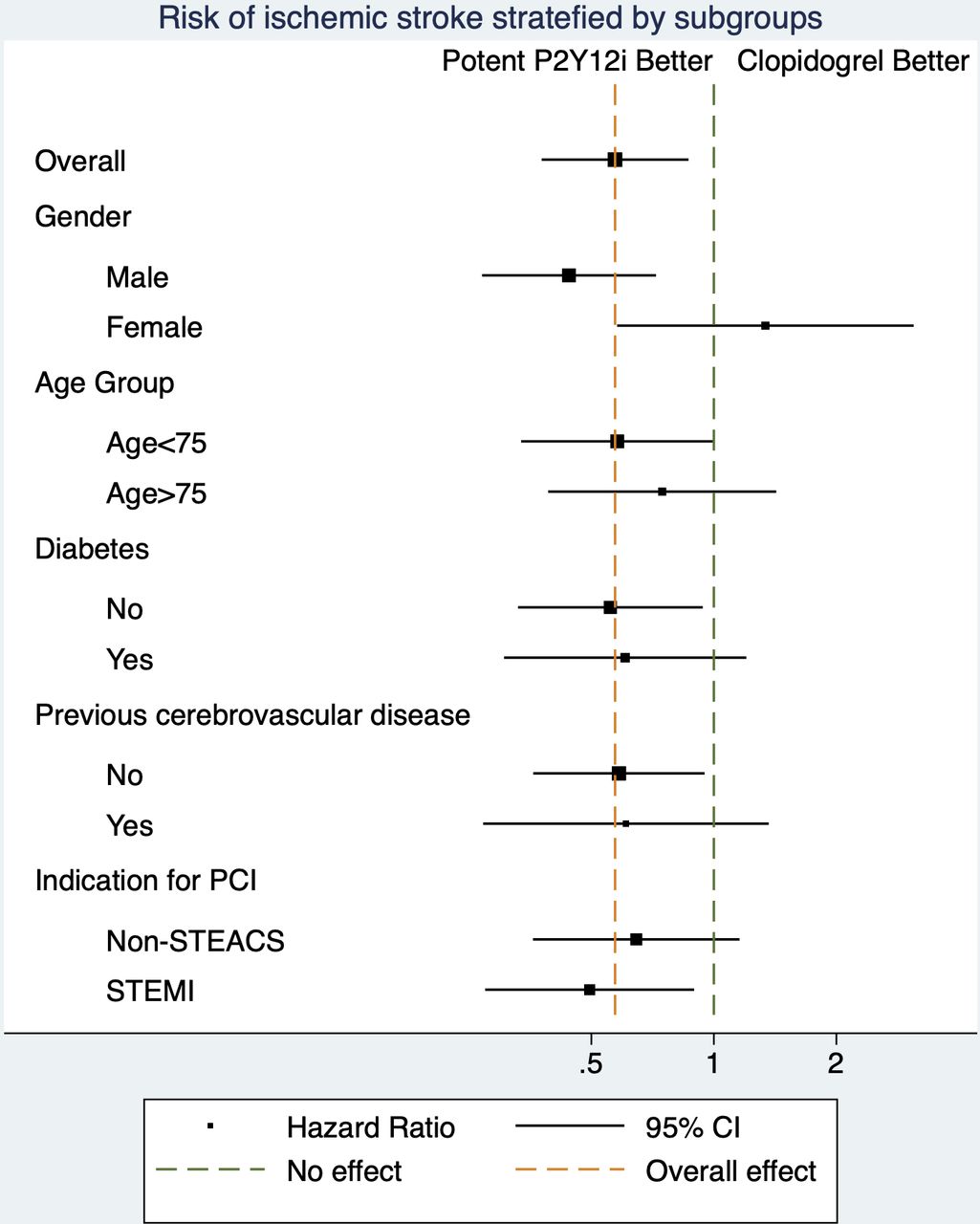
Forrest plot for subgroup analysis. HRs of ischaemic stroke stratified by P2Y12 inhibitors were modified by gender. P2Y12i denotes P2Y12 inhibitor. PCI, percutaneous coronary intervention.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forrest plot for subgroup analysis. HRs of intracranial haemorrhage (ICH) stratified by P2Y12 inhibitors were modified by age. P2Y12i denotes P2Y12 inhibitor. Non-STEACS, Non-ST elevation acute coronary syndrome; PCI, percutaneous coronary intervention; STEMI, ST elevation myocardial infarction.
Discussion
In this cohort of 6220 Chinese patients with ACS undergoing first-ever PCI, potent P2Y12 inhibitors were associated with lower risk of ischaemic stroke and similar risk of ICH, compared with clopidogrel. The risks of thrombotic events and MI were lower with potent P2Y12 inhibitors, while the risk of all-cause mortality was similar. The risks of major bleeding and fatal bleeding were also similar.
ACS can trigger systemic atherosclerotic inflammation and result in recurrent atherothrombotic events including stroke.27 Stroke after ACS can be devastating with a mortality rate up to one-third and poor functional outcomes in nearly two-thirds of the survivors.3 4 It is considered hierarchically as the second most important endpoint in the standardised composite endpoint definition of the Academic Research Consortium, after all-cause mortality.28 Although potent P2Y12 inhibitors were shown to reduce ischaemic events compared with clopidogrel after ACS, the individual endpoint of stroke was not reduced while the incidence of fatal or non-fatal ICH was increased in RCT and a large registry study.1 6 29 In a pooled meta-analysis of 82 784 patients from 12 RCT, there was no incremental benefit of potent P2Y12 inhibitors with regards to total stroke prevention.30 However, one would concern about the possibility that excess in haemorrhagic stroke with potent P2Y12 inhibitors might have offset the prevention of ischaemic stroke events. Furthermore, effects of potent P2Y12 inhibitors may vary across ethnic groups, as subgroup analysis indicated significantly less effect of ticagrelor in North America than in the rest of the world.1 31 This uncertainty is particularly problematic for East Asians, as they were well recognised to have a different thromboembolic and bleeding risks with regards to P2Y12 inhibitors compared with Caucasians.10–12 Unfortunately East Asians were vastly under-represented (<4%) in large scale RCT,1 6 even though they are currently the most populous ethnic group.
The current best evidence for East Asians came from smaller RCTs. However, due to the limited sample size, they are not sufficiently powered to detect any difference in ischaemic stroke and ICH. The PHILO study randomised 801 East Asians with ACS to ticagrelor or clopidogrel and found no significant differences in thrombotic or bleeding events.21 The PRASFIT-ACS study randomised 1363 Japanese patients with ACS to reduced dose prasugrel or clopidogrel, and found no significant differences in any composite or individual thrombotic and bleeding events.20 The TICA-KOREA study randomised 800 Koreans with ACS to ticagrelor or clopidogrel, and found in increase in major bleeding and fatal bleeding with ticagrelor, along with a numerically higher incidence of ischaemic events.19 Apart from RCT, several retrospective studies have compared MACE and bleeding events in Asians treated with different P2Y12 inhibitors. Yun et al examined 70 715 Asians with ACS and found a mortality benefit from ticagrelor over clopidogrel, but at a cost of increased minor bleeding with no differences in overall MACE. However risks of MI and stroke were not reduced with potent P2Y12 inhibitors. Importantly, ischaemic stroke were condensed together with haemorrhagic stroke in the effectiveness endpoint, therefore potentially masking any benefit in prevention of thrombotic events. Park et al examined 8010 Koreans with ACS and found that ticagrelor did not reduce ischaemic events but increased bleeding complications compared with clopidogrel.23 Similarly, ischaemic stroke were condensed together with haemorrhagic stroke in the efficacy endpoint. Lee et al examined 27 339 Taiwanese and found better anti-ischaemic effects from ticagrelor over clopidogrel without any difference in major bleeding.22 The driver for reduction in MACE was all-cause mortality and no differences in individual thrombotic endpoints were noted. Our study supplemented important data on the ischaemic stroke and ICH in relation to P2Y12 inhibitors in this population. Moreover, our findings were consistent with other observations that potent P2Y12 inhibitors were associated with reduced ischaemic events without excessive bleeding events in Chinese, a phenomenon differently observed in Koreas and Japanese studies which instead found no reduction in ischaemic events but rather excess in bleeding events.32
The choice of P2Y12 inhibitors for Asian patients with ACS is a real dilemma. An important advantage of potent P2Y12 inhibitors is their insusceptibility to CYP2C19 polymorphisms, which is more common in East Asian than Western patients.10 17 It is known that patients with any CYP2C19 allele associated with lower enzyme activity had lower levels of active clopidogrel metabolites, less platelet inhibition, lower risk of bleeding and higher risk of cardiovascular events.33 Therefore many East Asians may benefit from potent P2Y12 inhibitors. However, Asians are known to have a higher risk of ICH and cerebral microbleed with or without antithrombotic therapy.13–15 Asians also experience more bleeding events after ACS despite similar treatment,34 or when recruited in large scale clopidogrel RCT.35 This may have caused physicians to be more conservative in anti-platelet therapy for Asians. Our data supported that Chinese patients may benefit from potent P2Y12 inhibitors with regards to ischaemic stroke prevention and without excess bleeding risk, although this would require confirmation from RCT. Our findings can provide basis for the rationale and sample size calculation for RCTs dedicated for Asians.
Subgroup analysis showed that the protective effect of potent P2Y12 inhibitor on ischaemic stroke was more significant in male patients. This may be related to the lower proportion of women in our cohort and higher incidence of ischaemic stroke in men.36 37 We also identified a signal that potent P2Y12 inhibitors may not be as safe as clopidogrel with regards to ICH in patients ≥75 years old, although the interaction was mainly based on less ICH in patients <75 years old rather than excess ICH in those ≥75 years old. Nevertheless, prasugrel was previously noted to have a strong trend towards major bleeding including ICH in patients ≥75 years old and a related boxed warning was issued.6 Since age is generally known as an important risk factor for ICH in patients on anti-platelet therapy,38 future studies are needed to ensure the safety of intensification of antiplatelet therapy in elderly patients.
This study has some limitations. First, the observational nature of this retrospective cohort study conferred risks of unmeasured confounding and bias. We had adjusted extensively for potential confounders that may affect choice of P2Y12 inhibitor and outcomes, and the findings were consistent in multiple sensitivity analyses. Second, we only included patients who had first-ever PCI. Our findings may not be applicable to those who has ACS and recurrent coronary stenosis. Third, information on function outcomes of stroke were unknown to us. Forth, more patients transitioned from potent P2Y12 inhibitors to clopidogrel than vice versa. This could potentially create bias towards the null.
Further studies are needed to determine the best strategy of P2Y12 inhibitor use in Chinese or East Asian populations. The effects of CYP2C19 loss-of-function alleles or platelet reactivity, and extending to individualised genotypic or phenotypic guided anti-platelet therapy should be determined. It would be important to know to determine whether potent P2Y12 inhibitors prevented a certain subtypes of ischaemic stroke (ie, cardioembolic, small vessel related or large artery atherothrombotic stroke). Finally, it is important to identify any effect modification by age and cerebral microbleed burden in the association between ICH and choice of P2Y12 inhibitors.
Conclusion
Among Chinese patients with ACS undergoing first-ever PCI in Hong Kong, potent P2Y12 inhibitors were associated with a lower adjusted risk of ischaemic stroke and thrombotic events, compared with clopidogrel. The risks of ICH and major bleeding were similar.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW-20-176).
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drandrewkyng
Contributors AK-YN, KKL and C-WS was responsible for the conception and design of the study. AK-YN analysed the data collected by AI. AK-YN interpreted the data. AK-YN and PYN drafted the manuscript. AK-YN is responsible for the overall content as guarantor. All authors revised and approved the final manuscript, and are accountable for the accuracy and integrity of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.