Article Text

Statistics from Altmetric.com
Introduction
The benefit of mechanical thrombectomy for stroke associated with anterior circulation large vessel occlusion (LVO) is well established and among the most effective treatments in medicine.1 Stroke associated with basilar artery occlusion (BAO) was not included in the seminal thrombectomy randomised clinical trials (RCTs). BAO accounts for 1% of the ischaemic strokes and 5%–10% of the LVO, but 70%–80% of BAO victims evolve to death or full dependence.2 3 The terminal nature of the brainstem and thalamic circulations may predispose to such dismal outcomes.
Only two RCT designed to assess the efficacy of early (<6–8 hours since symptoms onset) thrombectomy for BAO treatment, the BEST and BASICS trials.2 4 Given the prior evidence for thrombectomy benefit for anterior circulation stroke is well settled; BAO stroke shares a similar physiopathology with very poor prognosis; the two available BAO trials had limited sample sizes but large absolute differences on the functional outcomes; we propose that an aggregated analysis of the BEST and BASICS trials should be performed under a Bayesian approach.
Methods
Thrombectomy RCTs designed for the enrollment of BAO-associated stroke patients were eligible for inclusion. The only exclusion criterion was the endovascular intervention time window: only early (6–8 hours) thrombectomy was considered. The MEDLINE and EMBASE databases were searched for articles in any language inception to October 2020. The descriptors ((basilar) OR (vertebrobasilar)) AND (stroke) AND (thrombectomy) were used within the filter ‘RCT’. The ClinicalTrials.gov database was also searched.
A Bayesian random-effects meta-analysis was modelled with a prior choice of µ effect parameter based on the results of the HERMES collaboration, in which thrombectomy was associated with a higher odd of modified Rankin Score (mRS) 0–3 at 90 days (OR 2.25, 95% CI 1.80 to 2.82).1 Thus, a Gaussian prior with mean 0.811 (2.25 in the logarithmic OR scale) and SD 0.414 (percentile 2.5 corresponding to the null effect, since a prior hypothesis of a thrombectomy deleterious effect was highly unlikely) was appropriate (online supplemental figure 1). A conservative prior distribution was chosen for the heterogeneity parameter τ (half-Normal, scale 0.5).5 The code (R language, bayesmeta 2.5) and data are available on request to the authors. The PRISMA guidelines was followed.
Supplemental material
Results
The initial search strategy yielded 43 studies (plus the BASICS trial preliminary results retrieved from the European Stroke Organisation/World Stroke Organisation conference report). Five studies were duplicates and another 35 were excluded because they were not an RCT or did not include basilar artery stroke. There are no other related ongoing RCT, except for the Basilar Artery Occlusion Chinese Endovascular Trial (NCT02737189), assessing the extended time window (6–24 hours). The literature database search confirmed only the BEST (Endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion) and BASilar artery International Cooperation Study (BASICS) trials investigated thrombectomy for the treatment of BAO acute stroke. These trials had similar inclusion criteria (except for a small difference in the stroke window tolerance for the performance of thrombectomy: 6 hours for the BASICS trial and 8 hours for the BEST trial). The samples included were reasonably homogeneous, but the BASICS patients received intravenous thrombolysis more often compared with BEST patients (~80% vs ~30%) (online supplemental table 1).
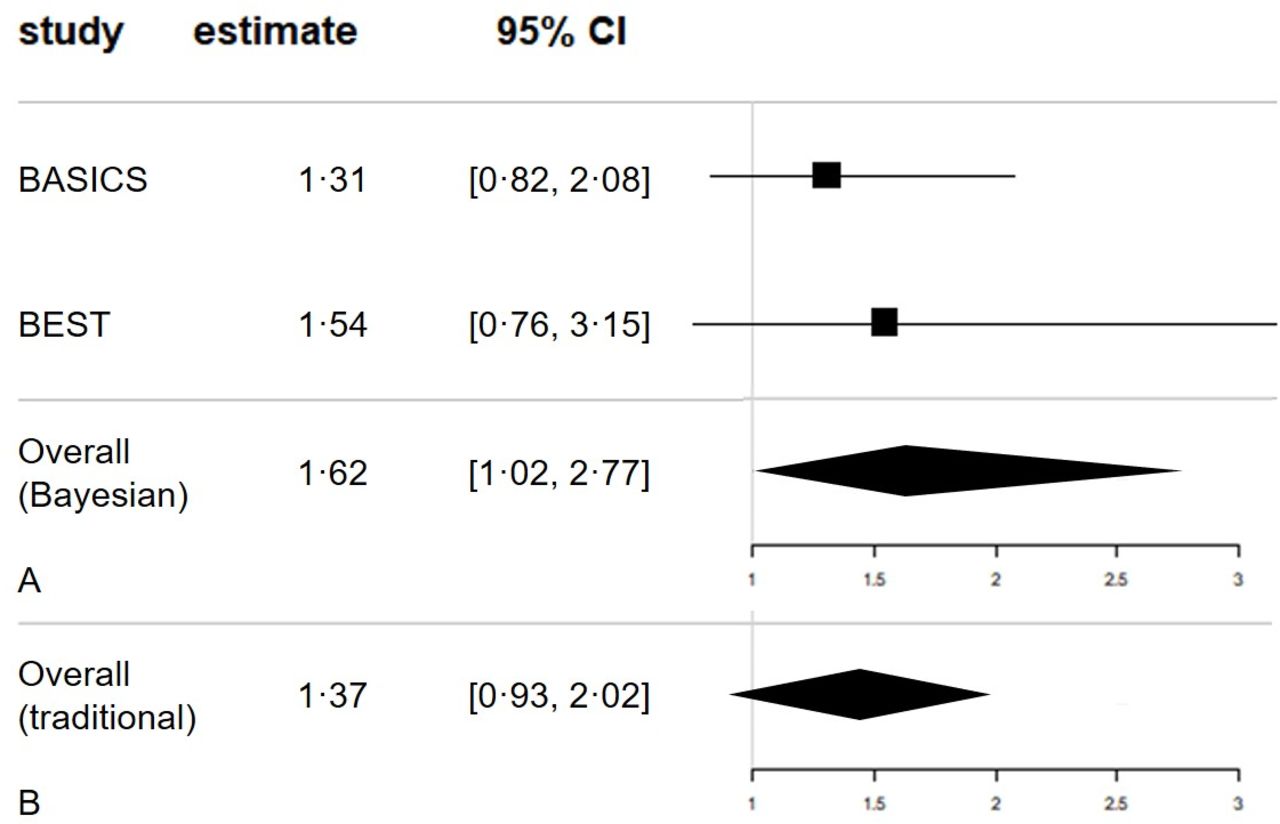
In the BEST trial intention-to-treat (ITT) analysis, there was no difference between treatment groups in the 90-day primary outcome, mRS 0–3 (intervention, 28/66, 42% and control, 21/65, 32%; OR 1.54, 95% CI 0.76 to 3.15). Similarly, no difference was found in the BASICS trial primary outcome ITT analysis (intervention, 68/154, 44% and control, 55/146, 38%; OR 1.31, 95% CI 0.82 to 2.08). In both trials, the secondary efficacy and safety outcomes were similar between groups.
Mechanical thrombectomy was associated with favourable functional outcomes in BAO stroke, with an OR 1.62% and 95% credible interval (high density interval) 1.01–2.77 (figure 1A and online supplemental figure 2). The observed absolute risk reduction would translate to a number need to treat of 13. Using classical (‘frequentist’) estimates, meta-analysis would result inconclusive, with an OR 1.37 (95% CI 0.93 to 2.02) (figure 1B).

{kind=link}
Meta-analysis for 90-day favourable functional outcome (MRS 0–3). (A) Bayesian approach. (B) Traditional approach.
Discussion
Although the individual trials resulted inconclusive, the Bayesian meta-analysis with an enhanced sample size and power suggested a functional outcome benefit for thrombectomy in BAO stroke patients. In view of the potential signal of benefit, we would advocate for the initiation of long-term clinically-led registries, especially in low-income and middle-income countries, where the greatest burden of the disease lies. Although our result is promising, we acknowledge that the BEST and BASICS trials authors, with the full individual-level database, will be able to perform a more comprehensive analysis, including subgroup stratification and/or meta-regression. A Bayesian approach may not be the ‘BASICS’, straightforward method, but it is probably the ‘BEST’ one for this scenario.
Acknowledgments
DJFS, AGK and KPB report grants and non-financial support from National Institute for Health Research (NIHR). AGK reports grants and non-financial support from University of Cambridge, grants and non-financial support from Royal College of Surgeons of England.
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @davisolla
Contributors Study conception: DJFS. Study design, data collection, data analysis and writing: DJFS and FCA. Data interpretation: all authors. Critical revision: KPB, AGK, JGMPC and JO-F.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.