Article Text

Abstract
Background and purpose The role of depression in the development and outcome of cardiometabolic diseases remains to be clarified. We aimed to examine the extent to which depressive symptoms affect the transitions from healthy to diabetes, stroke, heart disease and subsequent all-cause mortality in a middle-aged and elderly European population.
Methods A total of 78 212 individuals aged ≥50 years from the Survey of Health Ageing and Retirement in Europe were included. Participants with any baseline cardiometabolic diseases including diabetes, stroke and heart disease were excluded. Depressive symptoms were measured by the Euro-Depression scale at baseline. Participants were followed up to determine the occurrence of cardiometabolic diseases and all-cause mortality. We used multistate models to estimate the transition-specific HRs and 95% CIs after adjustment of confounders.
Results During 500 711 person-years of follow-up, 4742 participants developed diabetes, 2173 had stroke, 5487 developed heart disease and 7182 died. Depressive symptoms were significantly associated with transitions from healthy to diabetes (HR: 1.12, 95% CI: 1.05 to 1.20), stroke (HR: 1.31, 95% CI: 1.18 to 1.44), heart disease (HR: 1.26, 95% CI: 1.18 to 1.34) and all-cause mortality (HR: 1.41, 95% CI: 1.34 to 1.49). After cardiometabolic diseases, depressive symptoms were associated with the increased risk of all-cause mortality in patients with diabetes (HR: 1.54, 95% CI: 1.25 to 1.89), patients who had stroke (HR: 1.29, 95% CI: 1.03 to 1.61) and patients with heart disease (HR: 1.21, 95% CI: 1.02 to 1.44).
Conclusions Depressive symptoms increase the risk of diabetes, stroke and heart disease, and affect the risk of mortality after the onset of these cardiometabolic conditions. Screening and treatment of depressive symptoms may have profound implications for the prevention and prognosis of cardiometabolic diseases.
- stroke
Data availability statement
Data are available in a public, open access repository. The data that support the findings of this study are openly available in the SHARE at http://www.share-project.org/.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
With the rapid population ageing, non-communicable diseases (NCDs) pose a major public health challenge throughout the world.1 According to the WHO, the number of global NCD deaths per year has increased from 31 million in 2000 to 40 million in 2016, and it is estimated to further reach 52 million by 2030.2 3 Among all types of NCDs, cardiometabolic diseases, including diabetes, stroke and heart disease, are the most common kinds and leading causes of NCD deaths, which accounted for over 50% of NCD mortality during 2012.4 Traditional risk factors of cardiometabolic diseases, including age, gender, overweight/obesity, smoking, physical inactivity and unhealthy diet, have been investigated extensively in previous studies.5 6 However, these factors only partly explain the rising incidence and mortality of cardiometabolic diseases. To develop multiple preventive strategies, identifying novel modifiable risk factors for cardiometabolic diseases is in urgent need.
Depression is a common and recurrent psychological disorder that is linked to a wide variety of adverse consequences.7 In 2008, WHO listed depression as the third cause of global disease burden and projected that it would rank the first by 2030.8 The prevalence of major depression in patients with cardiovascular disease has been estimated to be over two to three times higher than that in the general population.9 Depression has also been shown to be an important independent risk factor for single cardiometabolic disease.10–12 However, several investigations also found inconsistent results.13–15
Furthermore, epidemiological studies in this domain are piecemeal, in that studies generally focus on the association between depression and single cardiometabolic disease (eg, diabetes,10 stroke,11 12 15 coronary heart disease (CHD)11 12 14) and single outcome (disability16 or mortality17 18). These studies neglect that cardiometabolic diseases are affected by several common risk factors and may interact with each other. Moreover, few studies have investigated the extent to which depression shapes the transitions from a healthy state to cardiometabolic diseases and subsequently to all-cause mortality. Considering the inherent links and competing risks among diabetes, stroke, heart disease and all-cause mortality, a holistic understanding of how depression affects the disease trajectory has the potential to develop comprehensive medical strategies for the prevention and prognosis of cardiometabolic diseases. Thus, this study used multistate models to simultaneously investigate the effect of depressive symptoms on the risk of diabetes, stroke, heart disease and subsequent all-cause mortality in a large-scale, cross-national and longitudinal survey.
Methods
Study population
We used longitudinal data on 78 212 individuals from the Survey of Health Ageing and Retirement in Europe (SHARE) during the period 2004–2018. SHARE is a nationally representative study of individuals aged ≥50 years across 29 European continental countries.19 It collected information about sociodemographic background, somatic and mental health, health-related behaviours, economic status and social networks using structured questionnaires. The first survey of SHARE (wave 1), which was conducted between 2004 and 2006, included 30 424 participants among 12 European countries. The six follow-up surveys (waves 2–7) have been conducted approximately every 2 years, with 108 588 refreshment samples included. To date, SHARE has surveyed a total of about 140 000 individuals. Informed consent was signed by each participant, and the protocol of the SHARE study was approved by the Ethics Committee of the University of Mannheim and Ethics Council of the Max Planck Society.
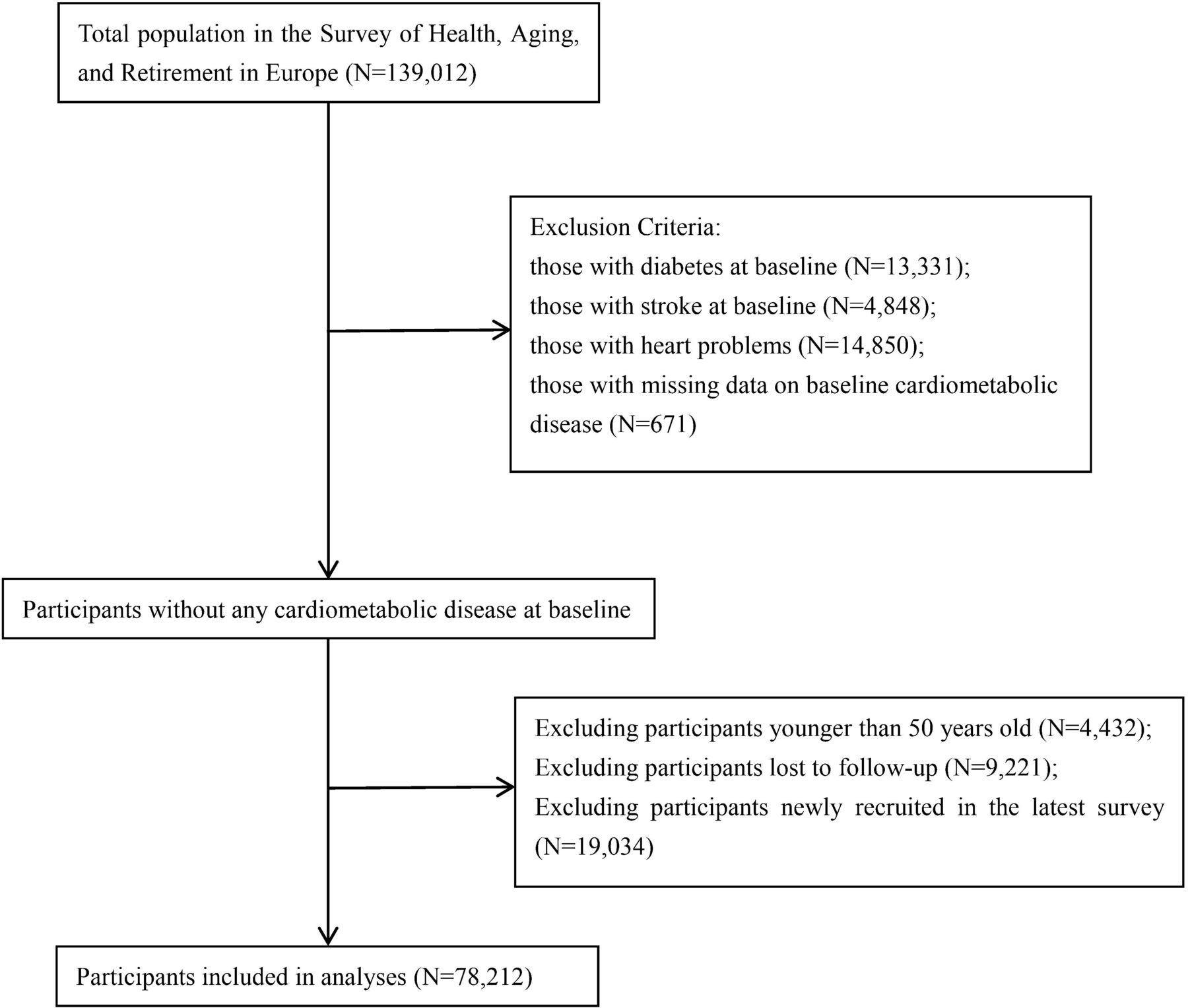
In this study, we selected participants who were initially investigated between wave 1 and wave 6 to ensure at least one follow-up visit for each participant. Besides, we excluded participants who were younger than 50 years at baseline, those with any cardiometabolic disease (diabetes, stroke and heart disease) at their initial survey and those without any follow-up information. In total, 78 212 respondents out of almost 140 000 participants were included for this analysis. The detailed flowchart of participant selection is presented in figure 1.

Flowchart of study participant selection.
Assessment of depressive symptoms
The Euro-Depression scale (EURO-D) was used to assess participants with depressive symptoms.20 It consisted of 12 items, namely, sad or depressed, pessimism, suicidal feeling, guilty, sleeping problems, interest, irritability, fatigue, appetite, concentration, enjoyment and crying. Participants were asked to answer the above questions by trained interviewers, with 1 point if answering ‘yes’ and 0 point if ‘no’. The total score is the sum of the scores for 12 items, ranging from 0 to 12, with a higher score indicating a higher degree of depressive symptoms. A cut-off value of ≥4 was used to define clinically relevant depressive symptoms, with an appropriate sensitivity (63%–83%) and specificity (49%–95%) validated in 14 European countries.20
Assessment of cardiometabolic diseases
The diagnosis of cardiometabolic diseases was determined by participants’ self-reported information in follow-up surveys. In each visit, respondents were asked whether a doctor has told he/she had or currently has diabetes or high blood sugar, heart diseases (including myocardial infarction, coronary thrombosis and any other heart problems), stroke or cerebrovascular disease (online supplemental text 1). Individuals were defined as having the corresponding cardiometabolic disease if an affirmative answer was given.
Supplemental material
All-cause mortality
Another outcome in our study was all-cause mortality. During follow-up, interview status (alive and dead) and interview time (year and month) were collected for each participant. Participants were followed up until the wave with death records or 31 December 2018. If respondents had complete information on death time, the survival time was calculated as the interval between the interview date of the enrolled wave and the exact death date. For participants whose death dates were not available, the survival time was defined as the median time from the initial interview to the wave with death record. For those who had survived during the follow-up period, the follow-up time was the interval between the first interview wave and the last interview wave.
Other covariates
The following covariates, extracted from the baseline waves, were adjusted in the multivariable models: age (50–59 years, 60–69 years, ≥70 years); gender (male, female); obesity (body mass index, BMI ≥30 kg/m2); marital status (married or partnered, others); drinking status (drinking and non-drinking); smoking status (never smoker, ever smoker, current smoker); physical activity (hardly ever or never, 1–3 times per month, ≥1 time per week); education (less than secondary school, upper secondary education, tertiary education); and taking medication for depression or anxiety (yes or no). Besides, other nine chronic conditions were also investigated at baseline by asking, ‘Have you been diagnosed with the following diseases by a doctor (namely, hypertension, cancer (excluding minor skin cancers), chronic lung disease, arthritis, high blood cholesterol, Parkinson’s disease, cataracts, hip fracture, stomach or duodenal ulcer)’. The total number of chronic diseases at baseline was categorised into three groups: 0–1, 2–3 and ≥4.
Statistical analysis
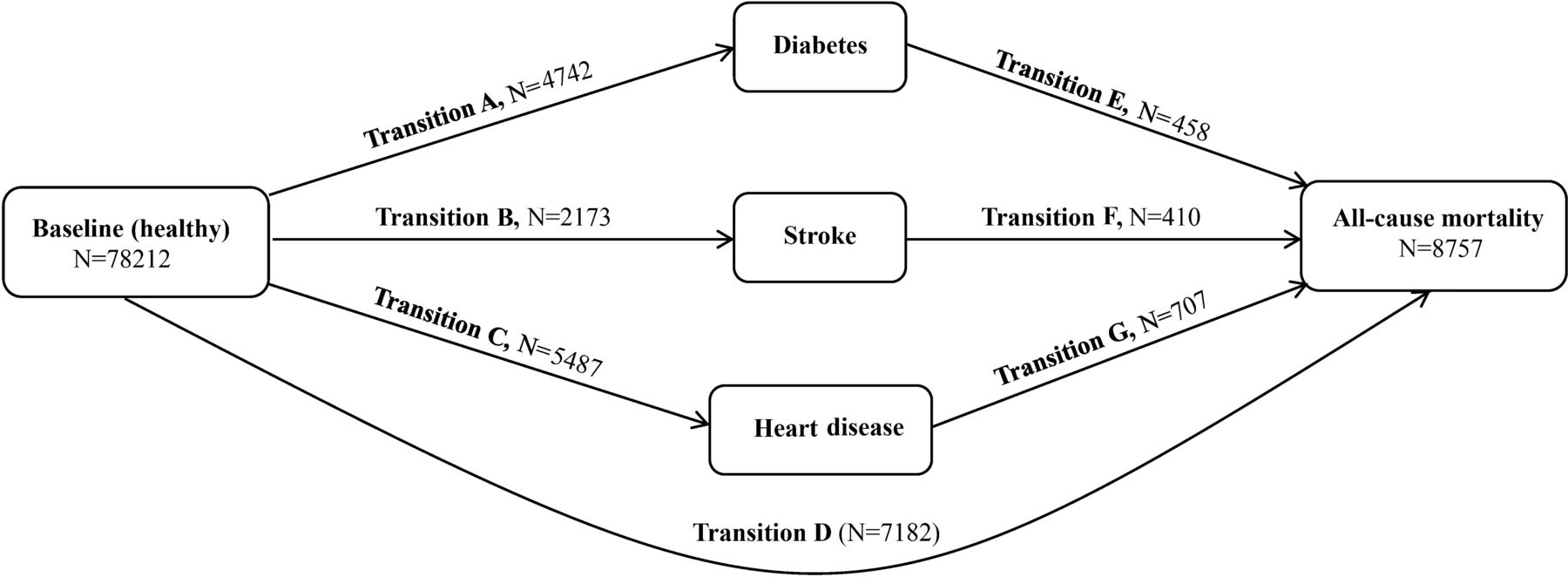
The baseline characteristics according to depressive symptoms are presented as frequency (percentage) and compared by the χ2 test. As shown in figure 2, we preplanned seven transitions from a healthy state to cardiometabolic diseases and subsequent all-cause mortality. We applied multistate models to evaluate the effect of depressive symptoms on the risk of all transitions from (A) healthy to diabetes, (B) healthy to stroke, (C) healthy to heart disease, (D) healthy to all-cause mortality, (E) diabetes to all-cause mortality, (F) stroke to all-cause mortality and (G) heart disease to all-cause mortality. Multistate models,21 22 an extension of competing risk survival analysis, could simultaneously estimate the risks of different transitions from an initial state to intermediate events and subsequently to final states in the same framework. Such an analytical approach could clearly delineate the time sequence and deal with competing risks in disease progress. These models are Markov processes, and the estimated probability of going to a future state only depends on the current state and not on history. Results are presented as transition-specific HRs and 95% CIs for cardiometabolic disease onset and subsequent all-cause mortality. The cumulative incidence functions of each transition were estimated according to depressive symptoms. Missing values of covariates (N=2454) were imputed using random forest models.23 Moreover, we performed several sensitivity analyses with the exclusion of subjects who had missing values of covariates and those with cancer or Parkinson’s disease at baseline.

Transitions from baseline (healthy) to diabetes, stroke, heart disease and all-cause mortality.
All statistical analyses were performed with SAS V.9.4 statistical software (SAS Institute) and the ‘mstate’ R package. P values less than 0.05 (two-sided) were considered as statistically significant.
Results
Of the 78 212 participants included in this study, the median (range) age was 61 (55–69) years and the proportion of women was 56.38%. The prevalence of depressive symptoms (scores of EURO-D ≥4) at baseline was 24.17%, with 16.09% in men and 30.42% in women. The baseline characteristics of participants by depressive symptoms are shown in table 1. Compared with participants free of depressive symptoms, individuals with depressive symptoms were older, more likely to be women, obese, illiterate and had more chronic diseases at baseline, but were less likely to be drinkers, smokers, physically active and married.
Baseline characteristics of study participants according to depressive symptoms
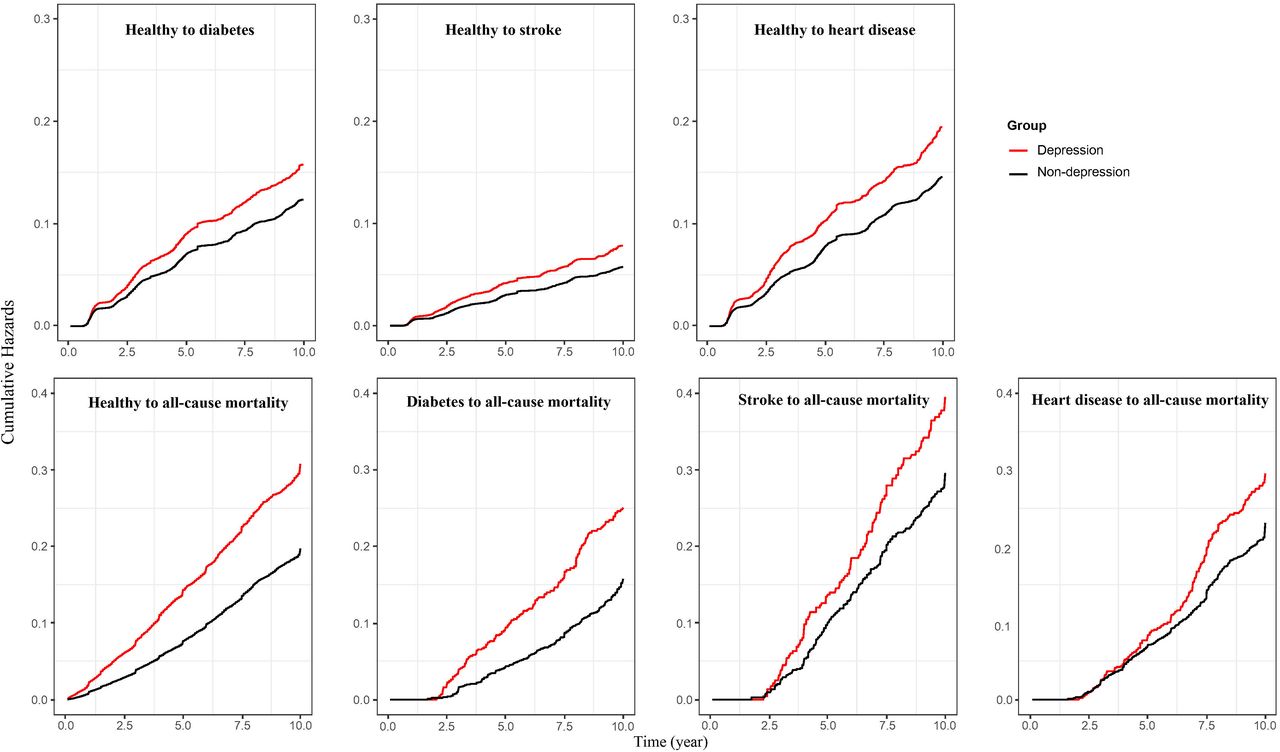
During 500 711 person-years of follow-up, the number of those experiencing cardiometabolic diseases and all-cause mortality were 4742 for diabetes, 2173 for stroke, 5487 for heart disease and 7182 for death events. The cumulative risks of diabetes, stroke and heart disease during the 10-year follow-up were 15.82%, 7.83% and 19.52% among depressed subjects, in contrast to 12.43%, 5.82% and 14.63% among non-depressed subjects (figure 3). After cardiometabolic disease, the 10-year cumulative risks of all-cause mortality were 25.05%, 39.51% and 29.51% for depressed participants with diabetes, stroke or heart disease, respectively. By contrast, the risks for non-depressed participants were 15.76%, 29.57% and 23.06%, respectively (figure 3).

{kind=link}
{kind=link}
{kind=link}
Cumulative hazards of different transitions by depressive symptoms.
Results from multistate models revealed that depressive symptoms were significantly associated with the risk of developing cardiometabolic diseases and subsequent transitions to all-cause mortality (table 2). After adjusting for age, gender, obesity, smoking, drinking, physical activity, marital status, education, country, taking medication for depression or anxiety, and the number of diseases at baseline, the HR (95% CI) values of different transitions were 1.12 (1.05 to 1.20) for transition A, 1.31 (1.18 to 1.44) for transition B, 1.26 (1.18 to 1.34) for transition C and 1.41 (1.34 to 1.49) for transition D. After the onset of these cardiometabolic diseases, depressive symptoms also increased the risk of all-cause death, with adjusted HR (95% CI) being 1.54 (1.25 to 1.89) in patients with diabetes, 1.29 (1.03 to 1.61) in patients who had stroke and 1.21 (1.02 to 1.44) in patients with heart disease.
Association between depressive symptoms and risk of diabetes, stroke, heart disease and subsequent all-cause mortality
Similarly, the subgroup analyses by gender indicated that depressive symptoms were also associated with increased risk of disease onset and subsequent all-cause death in both men and women (table 3). The positive associations were most pronounced for the transition from diabetes to death in men (HR: 1.56, 95% CI: 1.15 to 2.13) and women (HR: 1.56, 95% CI: 1.17 to 2.08). What’s more, the results were not changed a lot in the sensitivity analyses after excluding participants with missing values of covariates and those with baseline cancer or Parkinson’s diseases (table 3).
Subgroup and sensitivity analyses of the association of depressive symptoms with cardiometabolic diseases and all-cause mortality
Discussion
Based on a large prospective study with over 78 000 middle-aged and elderly participants, we evaluated the role of depressive symptoms in the temporal progression from healthy to cardiometabolic diseases and subsequently to all-cause mortality. Our results suggested that baseline depressive symptoms affected the risk of developing cardiometabolic diseases among the European middle-aged and elderly population. In addition, depressive symptoms also increased the risk of all-cause mortality among participants with diabetes, stroke or heart disease.
Despite the differences in tools used to measure depressive symptoms from previous studies, our findings were consistent with most of the findings that baseline depressive symptoms were positively associated with cardiometabolic disease onset.10–12 For example, a large cohort study consisting of approximately 0.5 million Chinese adults indicated that compared with participants free of major depression, individuals with major depressive episode had a 31% increased risk of developing type 2 diabetes.10 Péquignot et al reported that cumulative exposure to a high level of depression symptoms (HLDS) increased the risk of CHD and stroke.12 Among participants with the presence of HLDS, the risks were 1.64 times higher for stroke and 1.56 times higher for CHD at four study visits. However, several exceptions existed with inconsistent results. Nabi and his colleagues found that participants with mild to severe depressive symptoms or prescriptions of antidepressant medications had an increased risk of CHD but not cerebrovascular disease.14 We speculate that the small number of cerebrovascular events (N=129) might result in insufficient power for the association. Besides, a prospective cohort study involving 20 627 stroke-free individuals reported that 12-month major depressive disorder (MDD) was not associated with incident stroke.15 It is worth noting that in contrast to a 1-month retrospective recall period for EURO-D in SHARE, the 12-month period of recall for MDD in this study was more likely to result in recall bias.
What’s more, we further found a positive association between baseline depressive symptoms and transitions from cardiometabolic diseases to all-cause mortality. By contrast, studies investigating the association between depression and mortality in patients with cardiometabolic disease have been sparse and limited. Results from the First National Health and Nutrition Examination Survey (NHANES I) Epidemiologic Follow-up Study showed that compared with individuals with only diabetes, people with both diabetes and depression had a 33% elevated risk of all-cause death.17 Similarly, another study demonstrated that people with both depression and stroke had a higher risk of death than those with only stroke.18 A study among 337 patients with acute myocardial infarction showed that major depression was related to 2.54 times higher risk of all-cause mortality.24 In our study, heart diseases included any types of heart problems, such as myocardial infarction, coronary thrombosis and any other heart problem including congestive heart failure. The association between depressive symptoms and a specific type of heart disease needs further investigation in future studies.
The relationship between depression and cardiometabolic disease progression may be explained from both behavioural and biological perspectives. First, depressed people are more likely to fall into unhealthy behaviours, such as physical inactivity, smoking, obesity and non-adherence to medications.25 Besides, these poor health behaviours tend to appear together in the same depressed patient26 and have been acknowledged as important risk factors of cardiometabolic diseases. In our study, adjustment of unhealthy behaviours somewhat attenuated the associations of depressive symptoms with cardiometabolic diseases and subsequent all-cause mortality, suggesting that these lifestyles may confound or mediate the association between depressive symptoms and cardiometabolic morbidity. On the contrary, many biological mechanisms have been proposed for the adverse impact of depression on the course of cardiometabolic diseases. For example, depression is associated with enhanced activity of the sympathetic system and hypothalamic–pituitary–adrenal axis, resulting in elevated catecholamine or cortisol levels that are predictive of cardiovascular diseases and diabetes outcomes.27–30 Moreover, inflammatory biomarkers, such as C reactive protein and interleukin 6, are other potential mediation factors that link depression and cardiometabolic diseases.31–34 Furthermore, the reverse causality that persons with cardiometabolic conditions have an increased risk of depressive symptoms is also plausible. This notion has been supported by two previous meta-analyses. The prevalence of poststroke depression has been estimated to be approximately 30% among stroke survivors.35 Nouwen and his colleagues reported that compared with individuals without diabetes, individuals with type 2 diabetes have a 24% increased risk of depression.36
The primary strength of this study is our analytical strategy that involved all three cardiometabolic diseases and assessed both aetiological and prognostic factors in the same analytical framework. This strategy fully addressed the competing risks among these conditions and avoided false discoveries. Moreover, we excluded individuals with any cardiometabolic conditions at baseline, which enables us to map the causal pathway from depressive symptoms to cardiometabolic disease and subsequent mortality. Another strength of our study is the large sample size (N=78 212), which ensures the reliability of our results. However, there are also several limitations. First, depressive symptoms were only measured once at the baseline survey, while the potential changes during follow-up, particularly after the diagnosis of cardiometabolic diseases, and the duration of depressive symptoms were not available. The unrecognised depressive symptoms after disease diagnosis might underestimate the adverse impact of depressive symptoms on mortality. Second, although multivariate models adjusted for some important risk factors for cardiovascular diseases and diabetes, we cannot exclude the possibility of residual confounders due to data availability. Third, there may exist various biases in such a large-scale epidemiological survey. But in SHARE, elaborate preparations (including rigorous interviewers training, multidisciplinary conference and a pilot survey) have been completed before the formal interviews to minimise these biases. Moreover, results from sensitivity and subgroup studies were consistent with the primary analyses, indicating the robustness of our results. Fourth, depressive symptoms were measured only by EURO-D scale, but not a clinical diagnosis, which may introduce a measurement error and result in the underestimation of relationships. Finally, because the EURO-D scale was mostly used to detect late-life depressive symptoms in European populations, our results need further validation in other non-European countries.
Conclusion
In conclusion, we found that the presence of depressive symptoms was an independent risk factor for cardiometabolic diseases and contributed to increased all-cause mortality risk in people with cardiometabolic diseases. Screening and treatment of depressive symptoms in middle-aged and elderly adults may have profound implications for decreasing the incidence and mortality of cardiometabolic diseases.
Data availability statement
Data are available in a public, open access repository. The data that support the findings of this study are openly available in the SHARE at http://www.share-project.org/.
Ethics statements
Patient consent for publication
Ethics approval
Informed consent was signed by each participant. and the protocol of the SHARE study was approved by the Ethics Committee of the University of Mannheim and Ethics Council of the Max Planck Society.
Acknowledgments
This analysis uses data or information from the Harmonized SHARE dataset and Codebook, Version E.2 as of November 2019 developed by the Gateway to Global Aging Data. The development of the Harmonized SHARE was funded by the National Institute on Aging (R01 AG030153, RC2 AG036619, R03 AG043052). For more information, please refer to 'https://g2aging.org/ https://g2aging.org/'.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CK and YD conceived and designed the research; YQ, SL and GL performed the data analysis; YQ, SL and YL wrote the manuscript; YQ and YW interpreted the results of statistical analysis; and CK and YD revised it critically for important intellectual content. All authors contributed to the interpretations of the findings. All authors reviewed the manuscript.
Funding This work was supported by National Natural Science Foundation of China (81703316), Natural Science Foundation of Jiangsu Province (BK20170350), a project Funded by Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD) and Natural Science Research Projects of Colleges and Universities in Jiangsu Province (20KJB330004).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.