Article Text

Abstract
Background To examine the relationship of serum albumin with poor functional outcome and mortality in patients with acute ischaemic stroke (AIS) or transient ischaemic attack (TIA), and perform a meta-analysis to summarise the association.
Methods We analysed data from the Third China National Stroke Registry (CNSR-Ⅲ). Patients were divided into four groups based on serum albumin levels at admission. The outcomes included poor functional outcome (modified Rankin Scale (mRS) score of 3 to 6) and mortality at 3 months and 1 year. Multiple logistic regression models and Cox regression models were used to evaluate the association, respectively. We used a fixed-effect model to calculate the risk ratio for poor functional outcome and a random-effect model for mortality in the meta-analysis.
Results A total of 13 618 patients were enrolled. During the 3-month follow-up period, compared with 40 to 44.9 g/L group, patients in <35 g/L group had an increased risk of poor functional outcome and mortality (adjusted OR 1.37 (95% CI 1.12 to 1.67); adjusted HR 2.13 (95% CI 1.41 to 3.23)). The relationship in per 10 g/L decreased serum albumin with prognosis was consistently inversed (adjusted OR 1.17 (95% CI 1.01 to 1.35); adjusted HR 1.86 (95% CI 1.30 to 2.64)). Also, low serum albumin levels were independently correlated with clinical outcomes at 1 year. In the meta-analysis, the OR for poor functional outcome pooled 3 studies per 1 g/L decrease was 1.03 (95% CI 1.02 to 1.05), and the HR for mortality pooled 5 studies was 1.07 (95% CI 1.03 to 1.11).
Conclusions Low serum albumin levels predict poor functional outcome and mortality in patients with AIS or TIA.
- stroke
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Albumin is the most abundant serum protein synthesised primarily in the liver and regulated by multiple physiological mechanisms.1 2 It has several physiological properties, including maintaining colloidal osmotic pressure, antiplatelet aggregation and anti-inflammatory effects.3
Recent pre-clinical research found that moderate-dose albumin therapy after vascular recanalisation remarkably reduced infarction volume and brain swelling, and improved neurological function, suggesting that serum albumin has a neuroprotective effect.4 5 However, the results of the Albumin in Acute Stroke (ALIAS) trials on intravenous albumin in patients with stroke were negative disappointedly.6 This apparent paradox between the strong basic evidence and the failure in translation to humans brings great confusion. In the past, several studies have discussed the relationship between serum albumin and stroke prognosis, while the sample size was limited and lack long-term follow-up.7–11
Our study aimed to assess the correlation between low serum albumin level and poor functional outcome and mortality in patients with acute ischaemic stroke (AIS) or transient ischaemic attack (TIA) in a large, long-term follow-up, prospective registry. Furthermore, we performed a meta-analysis to summarise the association.
Methods
Study design and participants
The Third China National Stroke Registry (CNSR-Ⅲ) was an ongoing, nationwide, prospective stroke registry enrolling patients with AIS or TIA (≥18 years old; within 7 days from the onset) between August 2015 and March 2018. A total of 201 hospitals from 22 provinces and 4 municipalities in China participated. We collected aetiology, imaging and biology data, and tried to clarify the pathogenesis and prognostic factors of ischaemic cerebrovascular disease. Details on the design of the CNSR-Ⅲ have been published previously.12 The study protocol was approved by the ethics committee of all participating study centres. Each participant signed informed consent before enrolment, and was followed up at 3 months and 1 year. An independent contract research organisation performed data monitoring throughout the study period.
Data collection
Baseline information was recorded on admission by trained research coordinators. Some information, like patient demographics, medical history, primary diagnosis, acute recanalisation therapy, inpatient medication and laboratory tests, were extracted from medical records. Other parts were obtained from face-to-face interviews, such as the pre-stroke modified Rankin Scale (mRS) and National Institutes of Health Stroke Scale (NIHSS) scores. The aetiological classification was conducted by the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria.13 All images were stored in DICOM format on disks and centrally interpreted by two neurologists. Disagreements were resolved by discussion with a third reviewer. The presence of intracranial arterial stenosis and extracranial arterial stenosis was defined as 50%–99% stenosis or occlusion of any intracranial and extracranial artery.14 15
Serum albumin and alanine aminotransferase (ALT) were tested in sub-centres within the first 24 hours after admission. Bromocresol purple assay or bromocresol green assay were used to measure the serum albumin levels, which depended on the test reagent of sub-centres. High-sensitivity C reactive protein (hs-CRP), total cholesterol (TC), high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglyceride (TG) and serum creatinine were tested in the central laboratory of Beijing Tiantan Hospital. The blood samples were collected at admission and frozen in the cryotube at −80℃ refrigerator, then transported through the cold chain to the central laboratory. The estimated glomerular filtration rate (eGFR) was calculated by Chronic Kidney Disease Epidemiology Collaboration equations.16
Outcomes
The clinical outcomes included functional outcome and mortality, which were obtained through face-to-face interviews at 3 months and 1 year. The poor functional outcome was defined as mRS score of 3 to 6 (disability/death), and the good functional outcome was defined as mRS score of 0 to 2 (independence).17 Mortality included death from all causes.
Statistical analysis
Continuous variables were presented as mean±SD or median with IQR, and categorical variables as percentages. The baseline characteristics of different groups were compared by Kruskal-Wallis test for continuous variables and χ2 test for categorical variables. We used ordinal logistic regression to compare the disparity in mRS scores between different groups at 3 months and 1 year. The proportional hazards assumption of mortality was eligible for Cox regression. The association of serum albumin with poor functional outcome and mortality was analysed in logistic regression models for ORs and Cox proportional hazards models for HRs, respectively. Moreover, the relationship was tested by two types of data, four groups as categorical variable and every 10 g/L as continuous variable. Adjusted ORs, adjusted HRs and their 95% CI were calculated on three models. In the first model, we adjusted age and sex, which are demographic characteristics. In the second model, we added body mass index (BMI), medical history, index event, TOAST types, pre-stroke mRS score 0~2, NIHSS scores at admission, intracranial arterial stenosis, extracranial arterial stenosis, intravenous thrombolysis and inpatient medication, which were statistically significant in the baseline characteristics comparison. In the third model, we further adjusted the laboratory test, including TG, LDL, HDL, TC, ALT, eGFR and hs-CRP.
Restricted cubic splines were presented as the graphical representation of the associations. The interaction of age, sex, BMI, TOAST types, baseline NIHSS scores and eGFR were analysed by the multivariate logistic model and multivariate Cox model.9 10 18 19 Statistical significance was determined as p values <0.05, two-sided. All statistical analyses were performed with SAS software, V.9.4 (SAS Institute, Cary, NC).
Meta-analysis
The meta-analysis was conducted following the Preferred Reporting in Systematic Reviews and Meta-Analyses statement and the Meta-analysis Of Observational Studies in Epidemiology guidelines (online supplemental table 8).20 21 We searched PubMed, Scopus and Embase up to 22 May 2020, using the following combination of search terms: (“albumin” OR “hypoalbuminemia”) AND (“stroke” OR “cerebral ischemia” OR “cerebral ischaemia” OR “cerebral infarction” OR “transient ischemic attack” OR “transient ischaemic attack” OR “TIA”) AND (“outcome” OR “functional” OR “dependency” OR “mortality” OR “prognosis”). Articles were eligible if (1) the subjects were patients with AIS or TIA, (2) the design was a prospective study, (3) the exposure was serum albumin level (either categorised or continuous), (4) the outcome was poor functional outcome or mortality, and (5) an effect estimate with a 95% CI was reported. Two reviewers (HZ and AW) examined the retrieved papers based on the inclusion criteria mentioned previously. Disagreements were resolved by discussion with a third senior reviewer (Y-JW). The most adjusted ORs or HRs were extracted. We used the Newcastle-Ottawa Scale, the funnel plots, Begg’s tests and Egger’s tests to assess the bias risk of included studies (online supplemental table 7). We performed a fixed-effect model for poor functional outcome and a random-effect model for mortality according to the test of heterogeneity. All analyses were performed using R software V.3.6.3 (R Foundation for Statistical Computing, Vienna, Austria). More details of statistical analysis are shown in online supplemental material.
Supplemental material
Results
Baseline characteristics
Among the 15 166 patients in the CNSR-Ⅲ, a total of 13 618 (89.8%) participants completed serum albumin measurement and 3-month and 1-year follow-up (online supplemental table 1). They were divided into four groups based on serum albumin levels according to the previous literature: <35 g/L, 35~39.9 g/L, 40~44.9 g/L and ≥45 g/L (online supplemental figure 1).22 Overall, 980 (7.2%) patients were complicated with hypoproteinemia (defined as serum albumin level <35 g/L) at admission.23 The demographics and clinical characteristics of the study population are shown in table 1. Compared with the higher serum albumin groups, participants in the lower groups were inclined to be older, had lower BMI, TC, LDL, HDL, TG, eGFR and ALT level, but higher hs-CRP level, higher proportion of large-artery atherosclerosis (LAA) and cardioembolism (CE) in TOAST types, higher proportion of intracranial arterial stenosis and extracranial arterial stenosis, higher percentage of receiving intravenous thrombolysis and anticoagulant agents, and lower percentage of receiving antihypertensive agents. Meanwhile, patients with low serum albumin were more likely to suffer from diabetes mellitus, stroke or TIA, coronary heart disease and atrial fibrillation at baseline, and be dependent before the onset, more severe at admission (table 1).
Baseline characteristics of patients according to serum albumin levels
Clinical outcomes
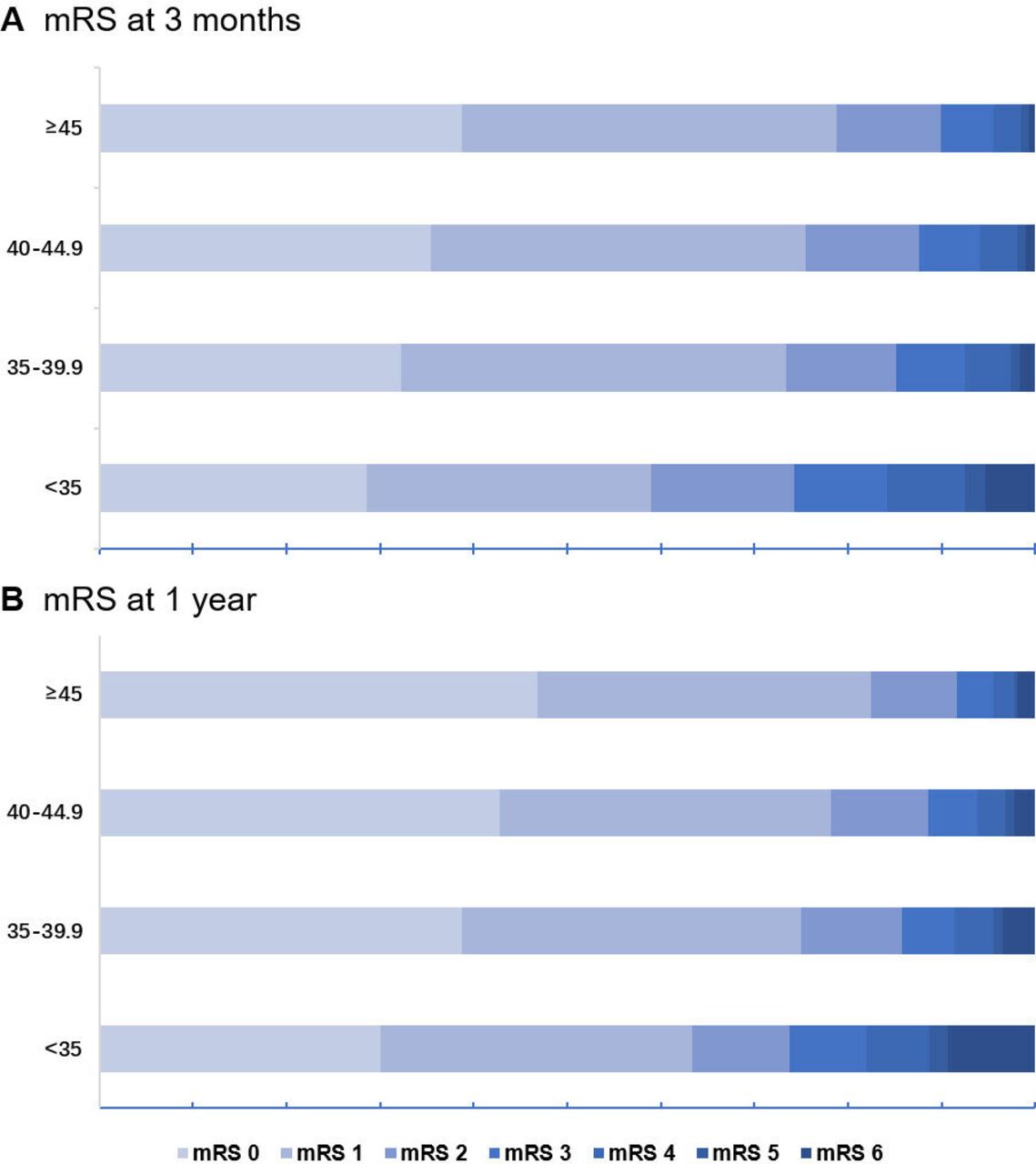
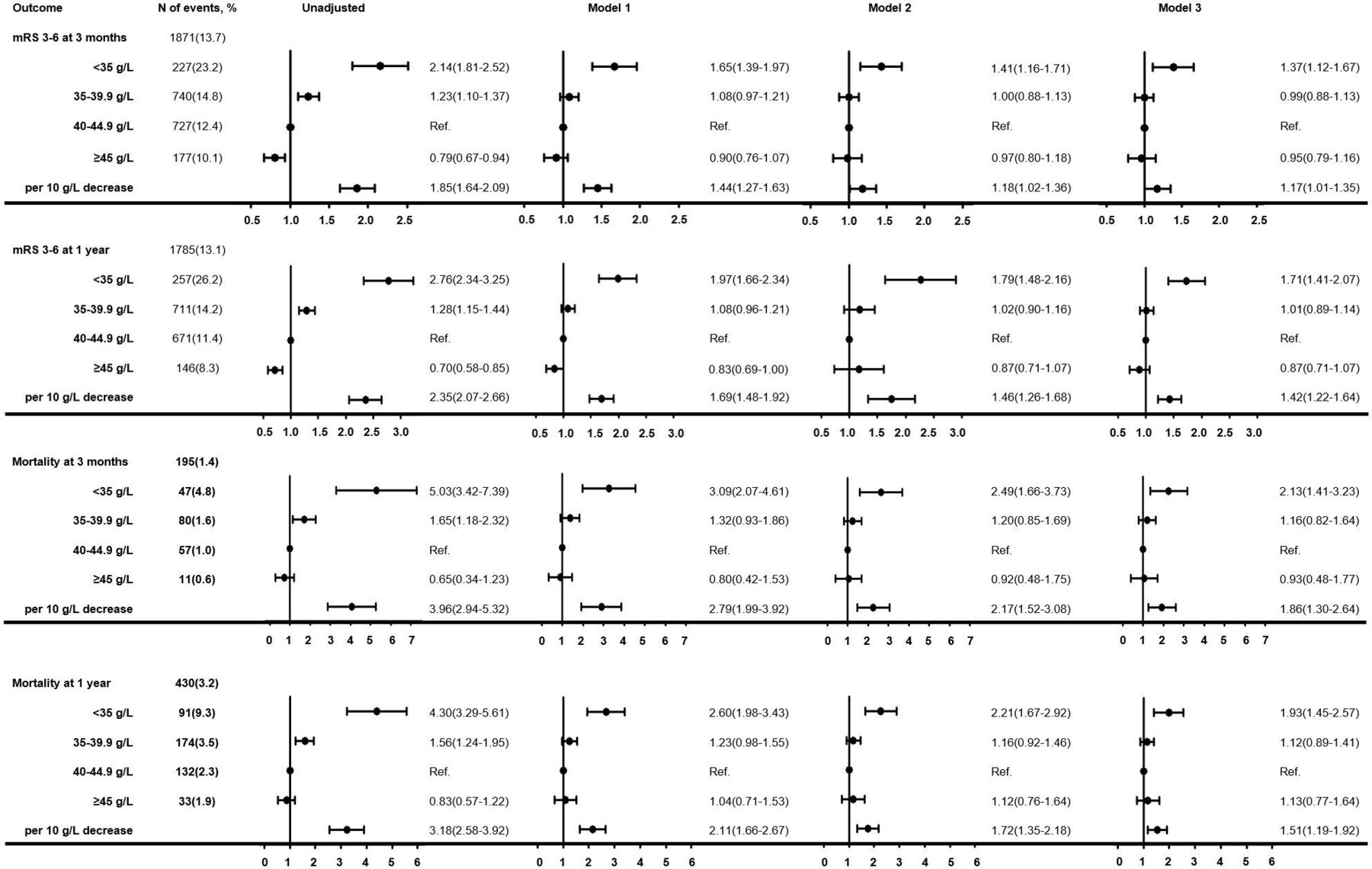
As shown in figure 1, the distribution of 3-month and 1-year mRS scores for four groups was significantly different (p<0.0001). During the 3-month follow-up period, 1871 (13.7%) patients had poor functional outcome and 195 (1.4%) patients died. Disability/died patients had lower serum albumin levels compared with independent patients (39.6±4.4 g/L vs 40.6±4.0 g/L, p<0.0001). For serum albumin level <35 g/L versus 40 to 44.9 g/L, crude OR for poor functional outcome was 2.14 (95% CI 1.81 to 2.52) and crude HR for mortality was 5.03 (95% CI 3.42 to 7.39). After adjustment for age, sex, BMI, medical history (hypertension, diabetes mellitus, stroke or TIA, coronary heart disease and atrial fibrillation), index event, TOAST types, pre-stroke mRS 0~2, NIHSS scores on admission, intracranial arterial stenosis, extracranial arterial stenosis, intravenous thrombolysis, inpatient medication, serum TG, TC, LDL, HDL, ALT, eGFR and hs-CRP level, the strong association still persisted (adjusted OR 1.37 (95% CI 1.12 to 1.67); adjusted HR 2.13 (95% CI 1.41 to 3.23)). In addition, the risk of poor functional outcome and mortality increased 17% and 86% for every 10 g/L decrease in serum albumin levels (adjusted OR 1.17 (95% CI 1.01 to 1.35); adjusted HR 1.86 (95% CI 1.30 to 2.64)) (figure 2).

Distribution of mRS score at (A) 3 months and (B) 1 year. mRS, modified Rankin Scale.
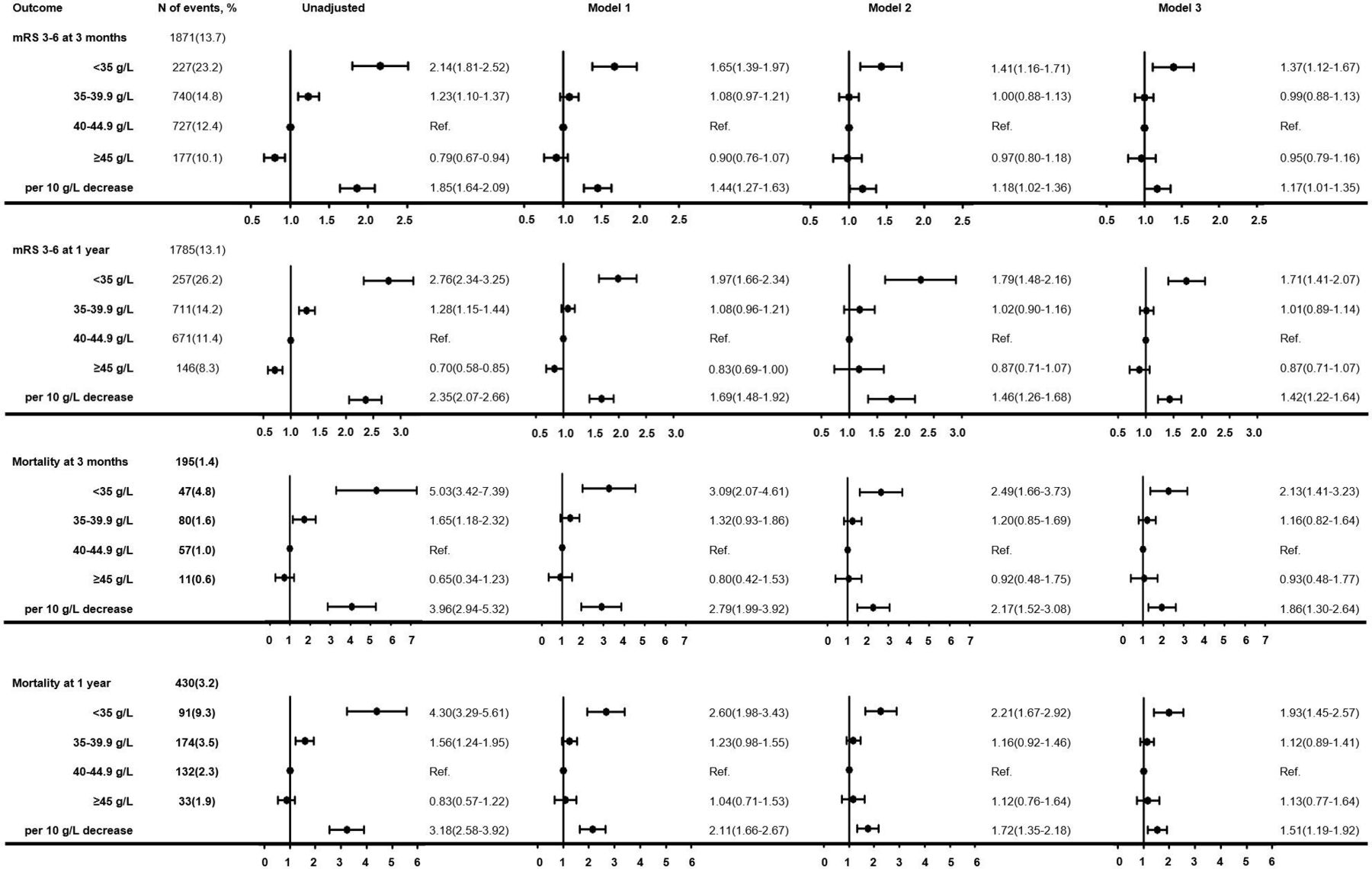
Association of serum albumin with clinical outcomes: HR/OR (95% CI). *Model 1: adjusted for age and sex. †Model 2: adjusted for covariables in model 1, plus BMI, medical history (hypertension, diabetes mellitus, stroke or TIA, coronary heart disease and atrial fibrillation/flutter), index event, TOAST types, NIHSS score on admission, pre-stroke mRS 0~2, intracranial arterial stenosis, extracranial arterial stenosis, intravenous thrombolysis and inpatient medication (antihypertensive agents, anticoagulant agents). ‡Model 3: adjusted for covariables in model 2, plus TG, TC, LDL, HDL, ALT, eGFR and CRP at admission. ALT, alanine aminotransferase; BMI, body mass index; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C reactive protein; LDL, low-density lipoprotein; mRS, modified Rankin Scale; NIHSS, National Institute of Health Stroke Scale; TC, total cholesterol; TG, triglyceride; TIA, transient ischaemic attack; TOAST, the Trial of Org 10172 in Acute Stroke Treatment.
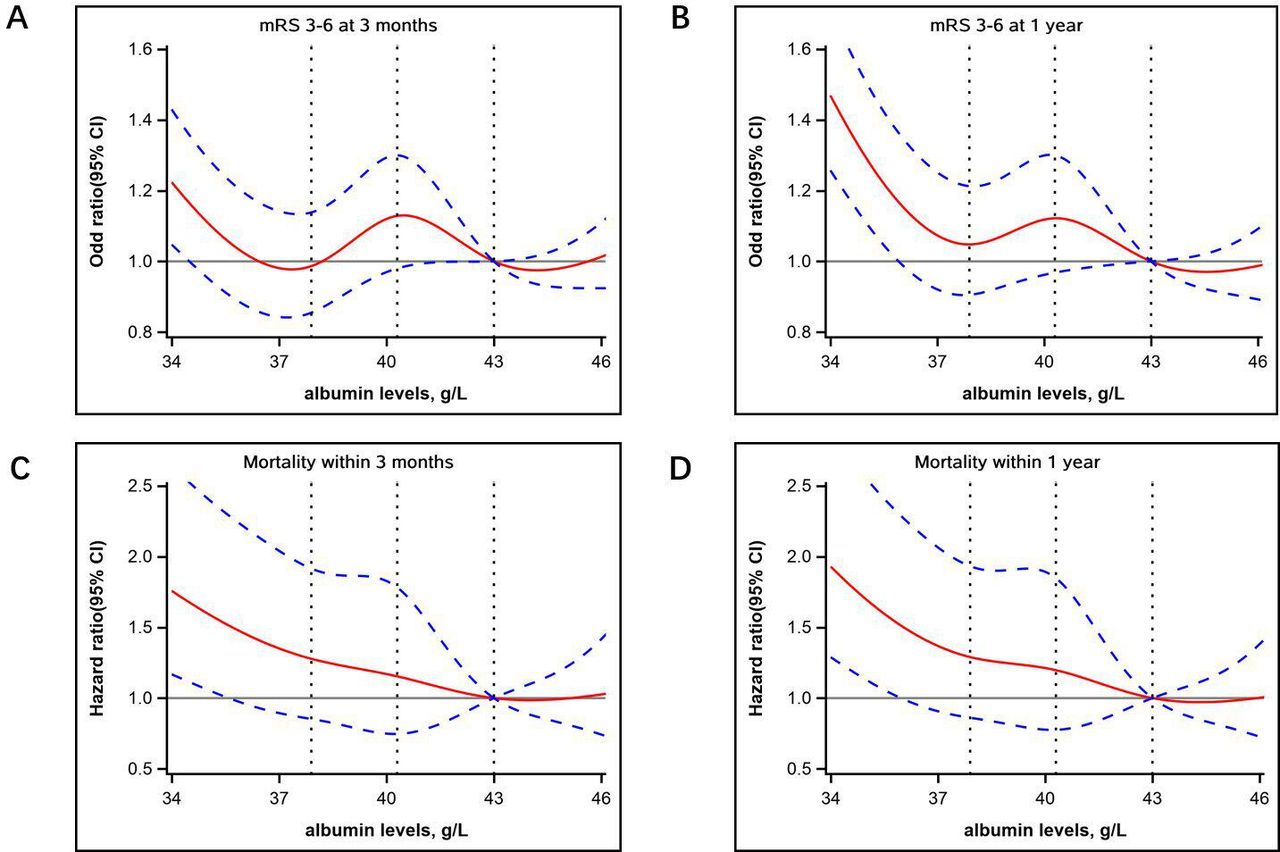
Furthermore, low serum albumin levels also independently predicted poor functional outcome and mortality at 1 year, whether it was a comparison in categorical variables or continuous variables (figure 2). As shown in figure 3, restricted cubic spline similarly confirmed the inverse association of decreased serum albumin levels with disability and mortality.

Spline models in the association between serum albumin and clinical outcomes The association with serum albumin level and poor functional outcome (mRS score of 3–6) at (A) 3 months and (B) 1 year. The association with serum albumin level and mortality at (C) 3 months and (D) 1 year. The red line indicates adjusted OR/HR, and the blue lines indicate the 95% CI. Data were fitted with a Cox regression model with adjustment for age, sex, BMI, medical history (hypertension, diabetes mellitus, stroke or transient ischaemic attack, coronary heart disease and atrial fibrillation/flutter), index event, TOAST types, pre-stroke mRS score 0~2, NIHSS scores on admission, intracranial arterial stenosis, extracranial arterial stenosis, intravenous thrombolysis, inpatient medication (antihypertensive agents, anticoagulant agents), serum TG, TC, LDL, HDL, ALT, eGFR and hs-CRP. ALT, alanine aminotransferase; BMI, body mass index; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C reactive protein; LDL, low-density lipoprotein; mRS, modified Rankin Scale; NIHSS, National Institute of Health Stroke Scale; TC, total cholesterol; TG, triglyceride; TOAST, the Trial of Org 10172 in Acute Stroke Treatment.
Subgroup analysis was stratified by age, sex, BMI, TOAST types, NIHSS score on admission and baseline eGFR. There were almost no variables that interacted with albumin and clinical outcome, except NIHSS score at admission ≤10 with 3-month poor functional outcome (adjusted OR 1.22 (95% CI 1.05 to 1.42); p for interaction=0.04) and 3-month mortality (adjusted HR 2.45 (95% CI 1.56 to 3.85); p for interaction=0.02) (online supplemental tables 2 and 3).
Meta-analysis
We identified 4357 relevant articles in initial. There was no meta-analysis of this issue conducted before. After removing 1781 duplicates and excluding 2531 references by title and abstract, 45 articles remained for the second evaluation. Based on the full text, we included six eligible studies in the final (online supplemental figure 2, tables 5 and 6).
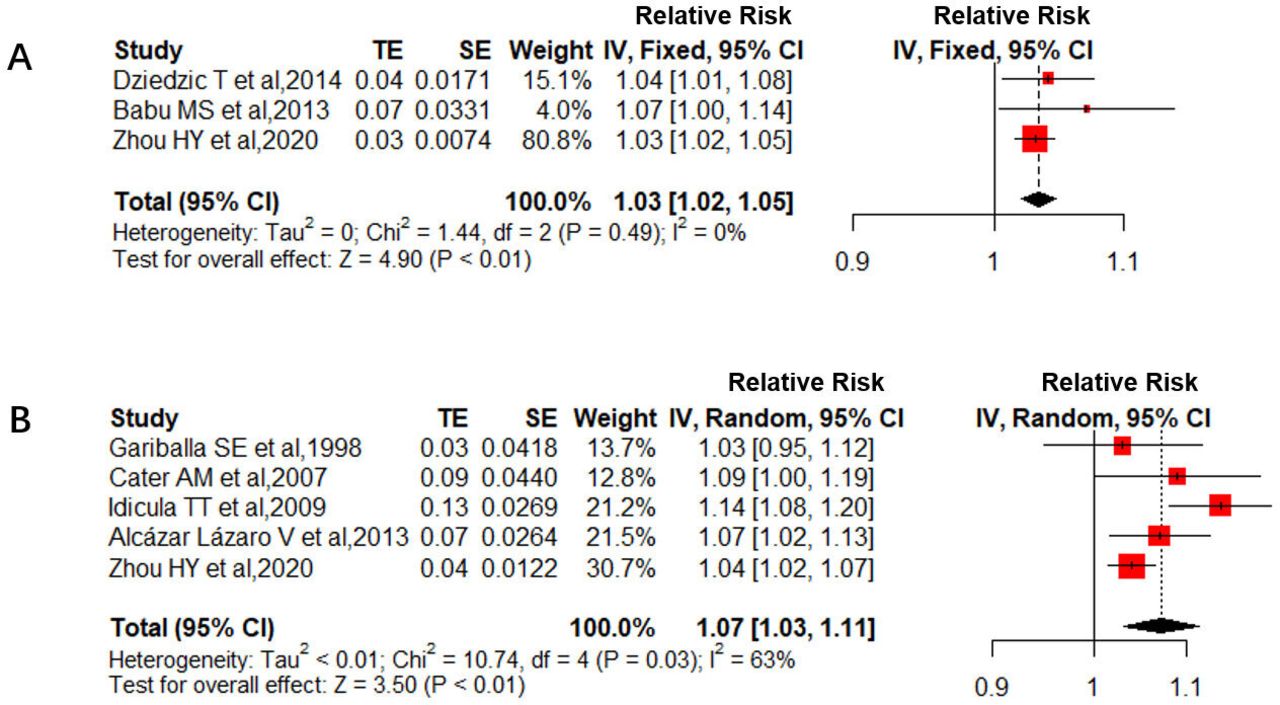
There were three studies (n=14 937) that reported the association of serum albumin with poor functional outcome. For per 1 g/L lower plasma albumin, risk ratio (RR pooled) of poor functional outcome obtained by a fixed-effect model was 1.03 (95% CI 1.02 to 1.05), without evidence of statistical heterogeneity (I2=0%; p for heterogeneity=0.49) and publication bias based on Begg’s tests (p=0.33) and Egger’s tests (p=0.24), whereas our research accounted for 80.8% of the weight (figure 4). Five studies (n=15 092) were included to explain the relationship between serum albumin and mortality. Due to the significance of statistical heterogeneity (I2=63%; p for heterogeneity=0.03), we used a random-effect model to calculate RR pooled of mortality (1.07 (95% CI 1.03 to 1.11)) (figure 4). No publication bias was observed according to Begg’s tests (p=0.48) and Egger’s tests (p=0.74). After excluding Idicula et al,10 which had fewer factors to adjusted HR value, there was no statistical heterogeneity (I2=0%; p for heterogeneity=0.58), and RR pooled of mortality was still significant (1.05 (95% CI 1.03 to 1.07)) (online supplemental figure 3). The funnel plots are shown in online supplemental figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of the meta-analysis showed relative risk and 95% CI of (A) poor functional outcome and (B) mortality in every 1 g/L decreased serum albumin. TE, treatment effect.
Discussion
In this prospective study, we confirmed that low serum albumin levels increased the risk of poor functional outcome and mortality in patients with AIS or TIA at 3 months and 1 year, especially in patients accompanying with hypoproteinemia. The results of the meta-analysis were additionally consistent.
In our population, hypoproteinemia accounted for only 7.2% of patients and varied from the previous data of 33.6%, which may be attributed to improved nutritional status and economic development, as well as the disparity in the inclusion criteria and sample size.7 Meanwhile, participants in our research were generally younger than in previous studies.8 9 Since recent publications reported that the incidence of hypoproteinemia in Chinese people over 65 years is 10.1%, and in the white Danish general population is 10.8%, ethnic differences of disease susceptibility cannot be excluded.22 24 Mild patients were more likely to be affected by albumin. We speculated that patients with severe illness may have more comorbidities or complications, which might mask the role of albumin.9
Previous research showed an association between low serum albumin and the incidence of CE and cryptogenic stroke, but not LAA.18 It was well established that low serum albumin levels were linked to many heart diseases, including atrial fibrillation, which was the main cause for CE,25 whereas in our study population, the proportion of CE and LAA both gradually increased with the decrease of serum albumin. Also, the average serum albumin level of patients with CE or LAA was all lower than that of other types (online supplemental table 4). This discrepancy may be partially explained by the different aetiological classification characteristics of patients with stroke in the East and the West.26 Even though our research may amplify the effect, there was some relevant evidence supporting the assumption that serum albumin was associated with LAA. Based on the prior basic medical studies, the weakening anti-inflammatory function, antioxidant effect and endothelial protection of low serum albumin might indirectly promote the development of atherosclerosis.27–29
We speculated that the powerful predictive function on poor functional outcome and mortality would be explained by three plausible pathophysiological mechanisms. First, because of a long circulatory half-life, serum albumin might serve as a biomarker of some pre-stroke pathological states, which seriously affect the prognosis, such as malnutrition.30 Nevertheless, we did not find the interaction between BMI and albumin, suggesting that there may be other likely diseases declining serum albumin levels and preventing the rehabilitation, such as kidney disease and cancer.19 31 Second, serum albumin deficiency may impair the balance of coagulation and anticoagulation. Early studies have shown that albumin is a cofactor mediating the binding of plasminogen to fibrin, and further participating in the interaction of tissue plasminogen activator.32 Also, serum albumin prevented arachidonic acid oxidation and inhibited thromboxane A2 synthesis, which is a potent stimulator of platelet aggregation.33 The decrease of serum albumin might weaken the anticoagulant effect and strengthen the coagulation function, and thrombus would be more likely to form.34 Besides, the excessive production for fibrinogen, and coagulation factors V and Ⅷ by the liver as compensation for hypoproteinemia might enlarge the coagulation pathway.35 Third, hypoalbuminemia increased the risk of stroke complications such as pneumonia, which significantly impaired survival status and functional recovery.36
In a recent subgroup analysis of the ALIAS trials, for patients with CE in the middle cerebral artery (NIHSS score ≥15), there was a trend to be effective when high-dose albumin therapy was started within 2 hours after onset, indicating that some specific subgroups might benefit from this treatment.37 Meanwhile, by careful fluid management and diuretic treatment, common complications included pulmonary oedema and heart failure after albumin infusion could be partially controlled.6 These remarkable findings indicated that a more precise and individualised application of albumin might be needed to re-examine the neuroprotection hypothesis. For patients with hypoproteinemia, positive therapy should be initiated as soon as possible. Also, the therapeutic options would be more effective by treating the underlying cause simultaneously, rather than mere albumin supplement.8 For patients with normal albumin, it might be more beneficial to take an appropriate dose of albumin infusion to specific subgroups of patients representative of pre-clinical settings while actively controlling complications.
Some prior studies have shown that high albumin level is associated with a better prognosis. However, it was based on comparison with low albumin level.10 Given the multiple physiological effects of albumin, there might be a ceiling effect in albumin therapy. More research is needed to find the sweet spot of serum albumin therapy. Furthermore, since albumin could pass through the blood–brain barrier, the strong adsorption function of albumin to transport relevant drugs to local damaged brain tissue will also have extraordinary effects on promoting functional recovery.38
This study has some limitations. First, only one period of serum albumin was measured, and there was no follow-up on the changes in albumin levels. Second, the serum albumin level was not tested immediately after the stroke. A previous study found that serum albumin levels might change during the first days after stroke, especially in patients with poor outcome.39 Therefore, our data may partially magnify the negative relationship between hypoalbuminemia and outcome. Third, serum albumin measurement of sub-centres was not uniform. In fact, the bromocresol green assay is a common method to measure albumin, but is affected by α1-globulin and α2-globulin, which might cause a positive bias, especially in severe hypoalbuminemia. Meanwhile, the bromocresol purple assay could avoid this effect.40 Therefore, our study may reduce the proportion of hypoalbuminemia, and weaken the correlation between low serum albumin level and poor prognosis. Fourth, there may be a selection bias when patients were enrolled. Some older patients with severe illness at the time of onset were more likely to refuse admission. However, they may be closely related to hypoalbuminemia. Fifth, despite no statistical bias, few studies were included in the meta-analysis, and the definition of poor functional outcome varied. More prospective studies are needed to validate the findings in the future.
Conclusions
In summary, low serum albumin level was a robust, independent predictor in poor functional outcome and mortality of patients with AIS or TIA. As a promising neuroprotective agent, serum albumin requires more further investigation.
Acknowledgments
We thank the staff and participants of the CNSR-III studies for their contribution.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @yilong
HZ and AW contributed equally.
Contributors Y-JW had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Y-JW designed the study. HZ, AW and XM collected the data. HZ and AW wrote the manuscript. HZ, AW and YZ completed the statistical analysis. JL, YJ, JJ, Y-LW, XZ and HL reviewed, edited and approved the final version.
Funding This work was supported by grant from National Key R&D Program of China (2018YFC1312903), grant from the National Natural Science Foundation of China (81870905), grant from Beijing Municipal Science & Technology Commission (Z181100001818001), grant from Beijing Municipal Administration of Hospitals Incubating Program (PX2020021) and grant from Beijing Excellent Talents Training Program (2018000021469G234).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Anonymised data are available to other researchers on request for the sole purpose of replicating procedures or reproducing the results by directly contacting the corresponding author and their institutions.