Article Text

Abstract
Background and purpose Approximately 15%–45% of patients with unruptured intracranial aneurysms have multiple intracranial aneurysms (MIAs). Determining which one is most likely to rupture is extremely important for treatment decision making for MIAs patients. This study aimed to develop and validate a nomogram to evaluate the per-aneurysm rupture risk of MIAs patients.
Methods A total of 1671 IAs from 700 patients with MIAs were randomly dichotomised into derivation and validation sets. Multivariate logistic regression analysis was used to select predictors and construct a nomogram model for aneurysm rupture risk assessment in the derivation set. The discriminative accuracy, calibration performance and clinical usefulness of this nomogram were assessed. We also developed a multivariate model for a subgroup of 158 subarachnoid haemorrhage (SAH) patients and compared its performance with the nomogram model.
Results Multivariate analyses identified seven variables that were significantly associated with IA rupture (history of SAH, alcohol consumption, female sex, aspect ratio >1.5, posterior circulation, irregular shape and bifurcation location). The clinical and morphological-based MIAs (CMB-MIAs) nomogram model showed good calibration and discrimination (derivation set: area under the curve (AUC)=0.740 validation set: AUC=0.772). Decision curve analysis demonstrated that the nomogram was clinically useful. Compared with the nomogram model, the AUC of multivariate model developed from SAH patients had lower value of 0.730.
Conclusions This CMB-MIAs nomogram for MIAs rupture risk is the first to be developed and validated in a large multi-institutional cohort. This nomogram could be used in decision-making and risk stratification in MIAs patients.
- aneurysm
- subarachnoid
- stroke
- complication
Data availability statement
Some or all data, models or code generated or used during the study are available from the corresponding author by request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Multiple intracranial aneurysms (MIAs) are encountered in approximately 15%–45% of patients with intracranial aneurysms (IAs).1–4 The Japanese ‘small unruptured IA verification study’ found that patients with MIAs are at a higher risk of IA growth and rupture.5 Compared with single IA cases, MIAs were also found to be associated with unfavourable outcomes after rupture.6 In addition, patient counselling in the elective setting is very challenging because good models for specifically predicting subarachnoid haemorrhage (SAH) in these patients are lacking; instead, information is extrapolated from varied data sets including patients with both single IA and MIAs. Moreover, the treatment strategy for patients with MIAs is typically complex and is driven by evaluation of rupture risks of each IA (particularly when considering endovascular management). Therefore, to prevent the catastrophic consequences of IA rupture, it is clinically important to identify and prophylactically treat the IA that is most likely to rupture.
Several studies characterised ruptured IAs in SAH patients with MIAs, and found that the aspect ratio (AR), irregular shape,2 size1 and size ratio (SR)4 could identify the ruptured IA. However, those studies only included MIAs patients with SAH and not those without. Although those studies may aid in identifying responsible IAs in these patients with SAH, they may not be adequately helpful in treatment decision making of MIAs patients without SAH, that is, whether to treat or manage conservatively and to identify the IA that should be treated. This may be attributed to the fact that decision making requires comprehensive consideration of the characteristics of both patients and IAs.
Significant demographic, clinical and morphological (CMB) differences are found between patients with single IA and MIAs,3 6 7 indicating that the underlying pathogenesis of MIAs may differ from that of single IA.8–10 Given the lack of analyses of large data samples, the true relevance of potential MIAs predictors remains unknown, and the existing scoring system is not suitable for these patients. One of the most popular models for predicting the IA rupture risk, the Population, Hypertension, Age, Size, Earlier SAH and Site (PHASES) score, was developed using 8382 participants from six prospective cohort studies to predict patient’s risk of IA rupture.11 However, the PHASES score only used the characteristics of the largest IA when evaluating MIAs patients, and data of other coexisting IA(s) were ignored. In addition, previous studies showed that one-quarter of the largest IAs did not rupture in patients with SAH and MIAs.1 2 Thus, it is necessary to develop a new method for assessing the rupture risk of each IA among MIAs patients to improve clinical decision making, especially in patients without SAH.
In this study, we aimed to identify the independent risk factors for IA rupture in a large multi-institutional cohort of MIAs patients. We also aimed to develop and validate a nomogram model for rupture risk assessment of each IA, and evaluate its clinical usefulness in aiding clinical decision making and improving ongoing treatment efforts.
Methods
Study population
We retrospectively obtained data regarding cerebrovascular images and medical records from a consecutive series of patients with at least two saccular IAs from three centres (Beijing Tiantan Hospital, Beijing Hospital and Peking University International Hospital) in China between September 2015 and December 2018. Aneurysms were divided into ruptured and unruptured groups depending on whether they were ruptured at admission. In patients with SAH, we only included those in whom the responsible IA could be identified; they included: (1) patients who underwent treatment by clipping in whom the ruptured IA was confirmed through microscopic visual assessment and (2) patients who underwent either endovascular or no treatment; in these cases, we included only those with a definitive haemorrhage pattern on computed tomographic images (localised to one IA). Examples of definitive haemorrhage patterns are provided in online supplemental figure S1. Patients with fusiform or dissecting IAs, other cerebrovascular diseases, IAs previously treated at other neurological centres, and incomplete clinical and imaging data were excluded.
Supplemental material
Clinical presentation
Data were collected regarding the following: age, sex, presence of hypertension (yes/no; diagnosed by the general practitioner before admission and requiring medical treatment), smoking, both current and previous (previously smoked regularly and quit at least 1 year before admission), alcohol consumption (yes/no; current or previous intake >5 drinks per day),12 presence of cardiovascular disease (yes/no; angina pectoris, myocardial infarction or peripheral vascular disease), and previous stroke (yes/no; transient ischaemic attack or stroke).
MIAs morphology
All patients in this study had digital subtraction angiography (DSA) images and three-dimensional (3D) reconstructions. All DSA angiograms and 3D reconstructions of the 1671 IAs were re-evaluated and measured by two researchers on a 0.1 mm scale; they were supervised by two senior neurointerventionists with 15 years of experience (online supplemental figure S2). The AR (dome height/neck width), SR (maximum IA height/average of the parent diameter), and bottleneck factors (dome width/neck width) were calculated. IAs were categorised as regular or irregular (with multiple lobes, daughter sacs or other types of wall protrusions). The inflow angle was defined as the angle from the parent artery into the IA, and the outflow angle was defined as that at which the IA flowed outward to the distal parent artery. The main branching angle was defined as the angle of the parent artery (in case of a sidewall IA) or that between the parent artery and the daughter branch most approaching 180° (in case of a bifurcation IA).2 All the associated angles were measured on a 1° scale (online supplemental figure S2). For bifurcation IAs, the branching to parent ratio was defined as the ratio of the sum of the diameters of the branch vessels to the diameter of the parent artery (in case of a sidewall IA, the branching to parent ratio was set to 1). The neck to parent ratio was defined as the ratio of the neck width to the parent artery diameter.
Statistical analyses
Continuous and categorical variables of patients’ baseline characteristics have been presented as means±SD and percentages, respectively. The 1671 IAs were randomly divided into two subsets with similar event rates, namely, the derivation subset (1171/1671, 70%) and the validation subset (500/1671, 30%). Mean imputation was used with low missing data; 20 factors with complete data (gender, age, SAH history, number of IAs, hypertension, diabetes, hypercholesterolaemia, heart diseases, history of stroke, smoking, drinking, size, neck, AR, branching to parent ratio, neck to parent ratio, SR, posterior circulation (PC, basilar tip, basilar-superior cerebellar artery, vertebral artery-posterior inferior cerebellar artery, or vertebrobasilar junction), irregular shape and bifurcation location) and three factors with less than 10% missing data (inflow angle (missing 31/1671, 1.9%), outflow angle (missing 31/1671, 1.9%) and branching angle (missing 35/1671, 2.1%)) were included in this study. Both, complete case and imputed data set analyses showed similar results.
Development and validation of the nomogram
Multivariate logistic regression analysis was performed for per-aneurysm rupture risk in MIAs patients using a forward stepwise method that included all variables with a p<0.20 on univariate analysis. After logistic regression analysis and risk factor calculation, we ranked nomogram variables using their p values and effect values to generate the nomogram model. Collinearity of combinations of variables in the derivation set was evaluated by variation inflation factors (VIF, with values <2 being considered non-significant). Overall performance was determined using the Brier score, ranging from 0 (excellent prediction) to 1 (worst prediction). Nomogram discrimination was assessed using the C-statistic to calculate sensitivity and specificity for prediction at each cut-off point. The C-statistic represents the area under the receiver operating characteristic curve (AUC); values of 0.5 and 1.0 indicate no and perfect ability to discriminate between patients with or without IAs, respectively. Calibration was assessed using the Hosmer-Lemeshow test and calibration curves. The decision curve analysis (DCA) was then used to determine the clinical net benefit associated with the use of the novel model in comparison to the unadjusted logistic models of other independent risk factors. The reference of DCA was calculated by treating all IAs, while treating none was set as zero-net benefit. For any given probability threshold, the risk model with the greater net benefit would be the preferred model.
In the present study, we also developed a multivariate model for a subgroup of 400 MIAs in 158 SAH patients, and compared its performance in discrimination and calibration based on all 1671 IAs in 700 patients; p<0.05 was considered statistically significant. All calculations were performed using SPSS V.25.0 and R software packages. The major R software packages used in this study are shown in online supplemental table S1.
Results
Study population
The database review from September 2015 to December 2018 in three centres identified 782 consecutive MIAs patients. After exclusion, a total of 1671 IAs were analysed from 700 consecutive patients with MIAs (1171 IAs in the derivation set and 500 IAs in the validation set). The flowchart of this study is shown in online supplemental figure S3. The baseline characteristics and univariable analysis results between the ruptured and unruptured groups of 1671 MIAs are summarised in online supplemental table S2. The characteristics of the patients and IAs in the derivation and validation cohorts have been compared in online supplemental table S3. No significant differences were noted between the derivation and validation sets. For all 1671 MIAs, the proportions of ruptured IAs were 8.9%, 10.8% and 9.5% in the derivation set, validation set, and entire cohort, respectively.
Univariate and multivariate analyses
The results of univariate analysis are shown in table 1. The following variables were significant in the derivation cohort: a history of SAH, size, AR, branching and neck to parent ratio, SR, PC, irregular shape, bifurcation location, inflow angle and branching angle. The results of univariate analysis for 158 SAH patients with 400 MIAs are shown in online supplemental table S4.
Univariate analysis between unruptured and ruptured groups in the derivation and validation set
Multivariable logistic regression including all 1671 MIAs revealed that seven variables: SAH history (OR, 5.094; 95% CI 2.848 to 8.929; p<0.001)), alcohol consumption (OR, 2.022; 95% CI 1.016 to 3.920; p=0.040), female sex (OR 1.856; 95% CI 1.053 to 3.395; p=0.038), AR >1.5 (OR 2.375; 95% CI 1.507 to 3.698; p<0.001), PC (OR 2.772; 95% CI 1.561 to 4.460; p<0.001), irregular shape (OR 1.883; 95% CI 1.225 to 2.897; p=0.004) and bifurcation location (OR 1.762; 95% CI 1.118 to 2.745; p=0.013) were significantly associated with MIAs rupture risk (table 2). The VIF of these factors in the derivation cohort were all <2, indicating non-significant collinearity of combinations of variables. The results of multivariable logistic regression only for MIAs patients with SAH (model 2) are shown in table 2.
Multivariate analysis of all 1671 multiple aneurysms in 700 patients and 400 multiple aneurysms in 158 patients who presented with SAH
Nomogram development and validation
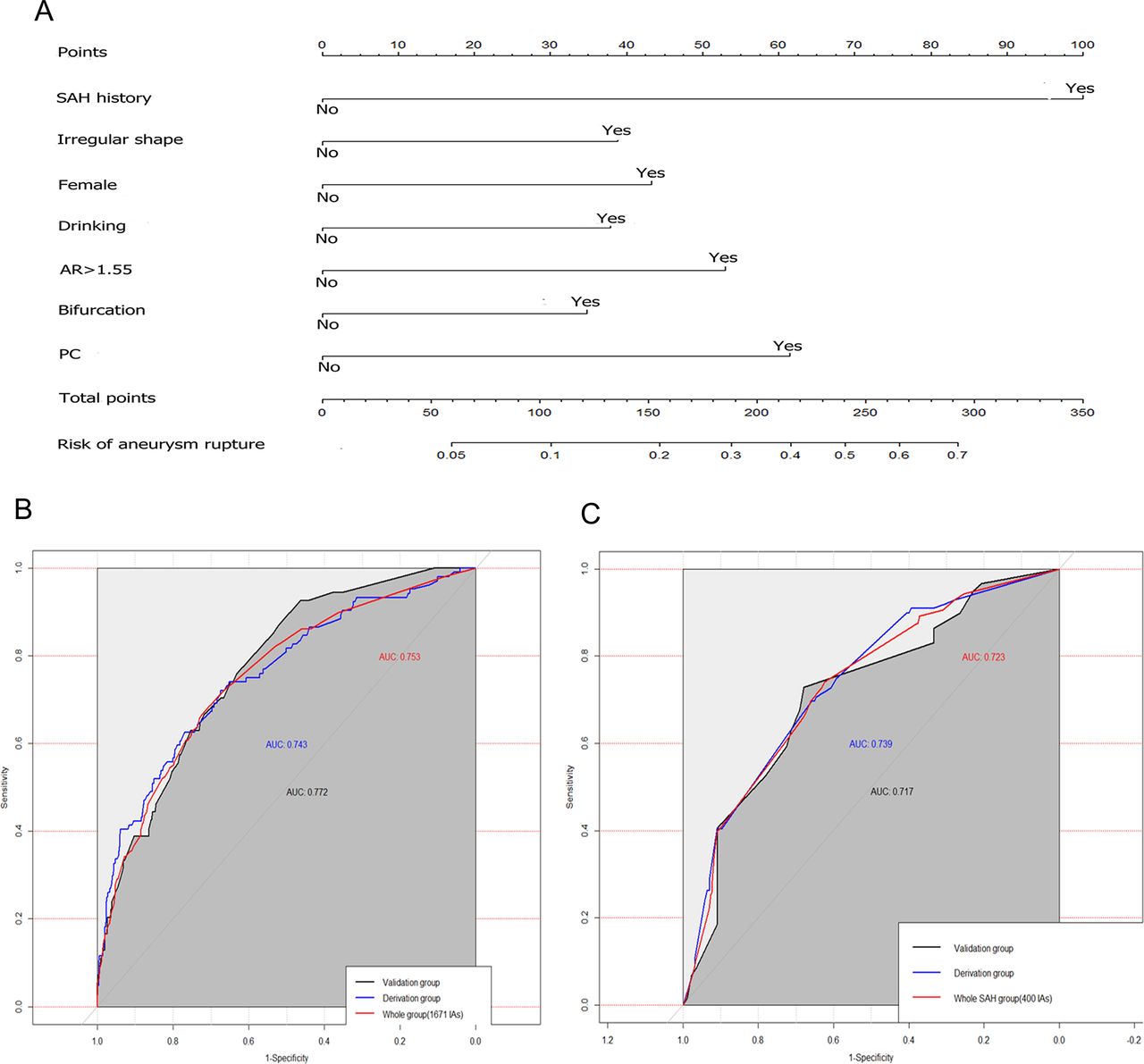
A CMB-based MIAs nomogram was constructed incorporating seven independent risk factors (figure 1A). The calibration curve of the CMB-MIAs nomogram (figure 2A) and the Hosmer-Lemeshow test (p=0.900) showed good calibration in the derivation cohort. An AUC of 0.743 (95% CI 0.690 to 0.796) showed good discrimination (figure 1B), and a Brier score of 0.073 showed good overall performance (table 3). The favourable calibration was also confirmed in the validation set (figures 1B and 2B) (p value of the Hosmer-Lemeshow test, 0.543; AUC=0.772 (95% CIs 0.686 to 0.858); Brier score=0.085). There was a good match between the predicted and observed probabilities of IA rupture (figure 2C,D). Thus, our nomogram performed well in both derivation and validation sets.

Distribution of survey respondents by country, region, occupation and by hospital context. AR, aspect ratio; AUC, area under the curve; PC, posterior circulation; SAH, subarachnoid haemorrhage.

Calibration curves of the CMB-MIAs nomogram in the derivation (A) and validation (B) set. The predicted probabilities and the actual observed probability of aneurysm rupture were divided into ten groups to create a bar chart for in the derivation (C) and validation (D) set. CMB, clinical and morphological; MIA, multiple intracranial aneurysms.
Evaluation of discrimination and calibration abilities of the models
Performance of the model for 400 MIAs in 158 SAH patients
Compared with the C-statistic of the model including all 1671 MIAs, the C-statistic of the model including 158 SAH patients had lower AUC values of 0.739 (95% CI 0.677 to 0.801) in the derivation group, 0.717 (95% CI 0. 632 to 0.802) in the validation group (table 3 and figure 1C), and 0.730 (95% CI 0.683 to 0.782) in the total group. The Hosmer-Lemeshow test comparing predicted and observed rates of IA rupture showed good calibration, with values of 3.574 (p=0.893) and 9.950 (p=0.269) for the derivation and validation groups, respectively. The calibration curves of the derivation and validation groups are shown in online supplemental figure S4. The Brier scores of the derivation and validation groups were 0.199 and 0.207, respectively (table 3).
Clinical usefulness of the nomogram
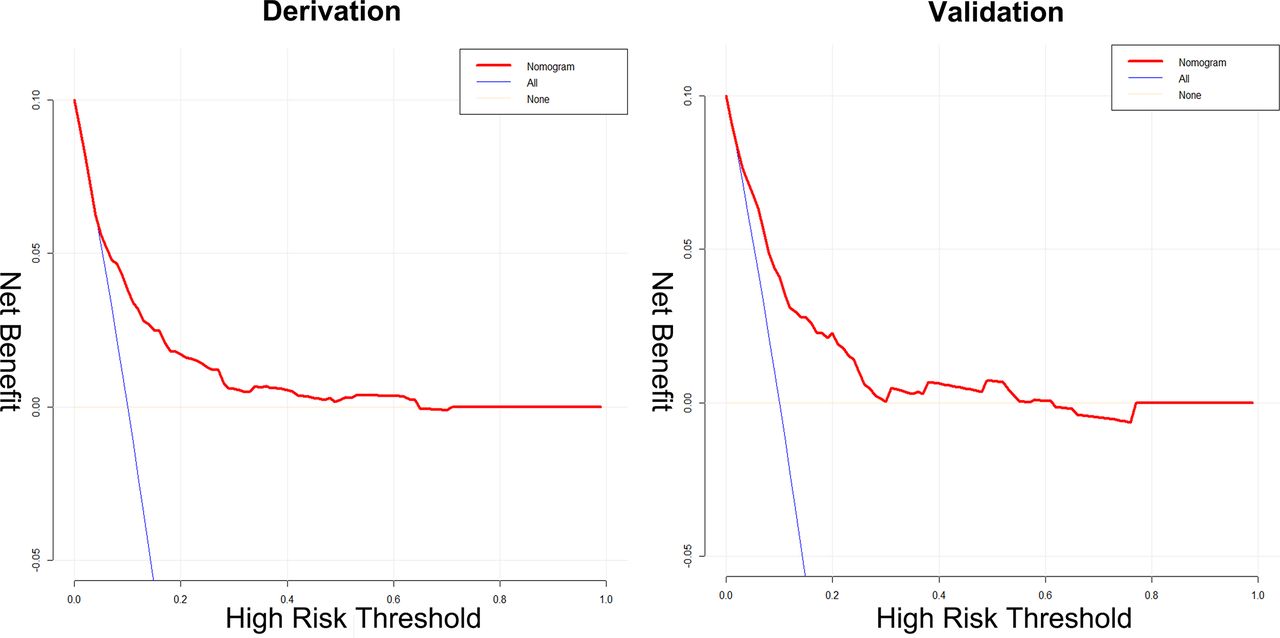
When the probability of IA rupture generated by the nomogram was between 0.10 and 0.65, DCA revealed that the CMB-MIAs nomogram conferred more benefit than either the treat-all or treat-none strategy in the validation and derivation groups (figure 3).
{kind=link}
{kind=link}
{kind=link}
Decision curve analysis of CMB-MIAs nomogram in derivation and validation cohort.
Discussion
We developed and validated an evaluation tool based on 1671 MIAs from a multicentre database to evaluate rupture risks of individual IAs in patients with MIAs. Our CMB-MIAs nomogram comprised seven readily available independent risk factors of IA rupture. The categorical variables by order of decreasing multivariate predictive effect were: SAH history, PC, AR >1.5, alcohol consumption, irregular shape, female sex and bifurcation location. To the best of our knowledge, this study is the first to attempt to establish a reliable nomogram for evaluating rupture risks of each IA in MIAs patients to improve informed decision making.
The presence of MIAs represents a greater risk than that of a single IA due to the higher complication rate associated with both IA rupture and treatment, which may involve complex management issues.13 14 The management of MIAs remains particularly challenging owing to variations in anatomical distribution, difficulties in determining IAs at higher risk of rupture and poor overall outcomes in cases of SAH.15 The treat-all or treat-none strategies can be ineffective or expensive. Thus, it is essential to identify IAs that are most likely to rupture.16 17
Major efforts have been made to stratify IAs based on rupture risk assessment. The most widely used methods include morphological analysis,4 18 clinical factor assessment1 19 and scoring systems,11 20 21 which are mainly based on clinical risk factors and morphological features. However, the existing scoring system is not suitable for MIAs. Although the PHASES11 and Earlier SAH, Location, Age, Population, Size, Shape21 scores are almost identical in terms of predictors, both use characteristics of the largest IA to categorise MIAs patients21 and may, therefore, be unsuitable for comparing coexisting IAs. For cases with MIAs, the unruptured IA treatment score20 evaluates each IA separately; however, most of the study population comprised patients with single IA. There are already some prediction models for evaluating the risk of rupture in those with IAs, including MIAs. Tominari et al built a prediction model for 3-year rupture risk of IAs in Japanese patients, by including 6606 IAs in 5651 patients.22 They also considered each IA as a unit of analysis; in this study, we applied this score to evaluate the rupture risk of 1671 MIAs. The results showed that the AUC of their model for the 1671 MIAs in this cohort was 0.577; this was worse than that of our model (AUC=0.753). This may be attributed to the fact that although the study included a large sample of IAs, only 13.7% of derivation data and 12.7% of validation data were from MIAs patients; therefore, their model may be more suitable for single IA patients. In addition, this study may have selection bias. Some unruptured IAs with a high risk of rupture were treated and not included in the follow-up cohort. This necessitates the development of a prediction model specific for MIAs.
To date, several studies have focused on identifying risk factors for MIAs rupture.1 2 4 8 23 However, the populations were limited to MIAs patients with SAH, and the variables analysed were limited to IA morphological characteristics. These studies mainly intended to accurately identify ruptured IAs in SAH patients with MIAs. As we pooled individual patient data from three larger centres in China, we were able to analyse clinical risk factors and morphological features of IAs in MIAs patients with or without SAH; we were also able to calculate the absolute risks of individual IA rupture. In addition, we developed a multivariate model for SAH patients with MIAs (model 2). In this model, the AUC in the derivation and validation groups were 0.739 and 0.717, respectively; these results were worse than those of the model including all MIAs patients.
Risk scores are more reliable if they include already well-established risk factors for IA rupture.11 Most risk factors included in our model are known to cause IA rupture; these included the following: history of SAH,11 24 female sex,25 alcohol consumption,26 27 bifurcation location,28 29 location of PC,19 AR30 and IA shape.18 19 DCA evaluates whether a model is useful in clinical decisions and identifies the model leading to the best decision.31 In the present study, when the threshold probabilities were between 10% and 65%, DCA showed that the nomogram was more beneficial than either the treat-all or treat-none strategy (figure 3). These results indicate the clinical benefits of using the CMB-MIAs nomogram.
We found that IA size and number,12 and smoking status were not associated with IA rupture when other risk factors were considered. This does not imply that these factors are not important for MIAs rupture in isolation; it indicates that these factors were not significantly associated with IA rupture in addition to the seven predictors used. Aneurysm size was ranked the most important risk factor; physicians widely accept that larger IAs are more dangerous than smaller ones.32 However, a large cohort study of patients with IA SAH and MIAs2 revealed that the largest IA had not ruptured in 36 (29%) of 124 MIAs patients. Interestingly, for SAH patients with MIAs, IA size was significantly associated with IA rupture; the risk of IA rupture increased with size in the range of 3–15 mm, (online supplemental figure S5A). This suggests that IA size may help identify ruptured IAs in SAH patients; however, this is not necessarily applicable to all MIAs patients, and especially in those with IAs with irregular shapes (online supplemental figure S6). A previous study revealed that in MIAs patients, each IA is not associated with an increased risk of rupture; however, these patients are subject to the cumulative risk from all individual IAs.19 Similarly, we found that the IA number is not associated with an increased risk of rupture. In addition, compared with patients with three or more IAs, those with two IAs demonstrated more ruptures (online supplemental figure S5B). Regarding smoking status, we only had data regarding the time of IA detection, and not for the intensity and duration of smoking or passive smoking. The association between smoking and MIA rupture requires further in-depth research, with more detailed questionnaires or prospective studies. We found that hypertension was not a significant factor on univariate analysis in both, derivation and validation cohorts. However, statistical differences were observed between ruptured and unruptured groups in the entire cohort. This may be explained by the fact that the results of randomisation caused a slight change in the distribution of this subgroup. However, we believe that this will not significantly impact the results of multivariate because factors with p<0.2 have been incorporated into the multivariate analysis. The SR,4 in/outflow angle,1 2 branching angle1 and neck width30 are widely used morphological indexes for IA stratification. Nevertheless, these factors were not significantly associated with IA rupture in our study.
Strengths and limitations of the present study
An important strength of this study is that it included a large number of MIAs patients with high-quality angiograms; this adequate sample number enabled the development of a multivariable prediction model for MIAs. Second, the inclusion of patients from three different centres improved the validity of our results. Third, the risk factors included in our prediction model are easy to retrieve from outpatient clinics; this will improve its utility in daily clinical practice.
Nevertheless, our study also has certain limitations. First, the retrospective nature of our study inevitably introduced bias, which may have affected our analysis. Prospective multicentre validation is needed to acquire high-level evidence for further clinical application. Second, although our nomogram exhibited favourable discriminatory and calibration ability regarding predictive value and net benefit in the derivation and validation cohort, it should be noted that our model was developed using data from patients treated at Chinese institutions. Thus, caution is needed when generalising our results to other countries and ethnicities. Third, our study did not include other factors that may be associated with aneurysm rupture, such as blood pressure levels, family histories and imaging indicators such as haemodynamic analysis and vascular wall enhancement on MRI.33 Fourth, morphological measurements may change during and after rupture. A large-scale prospective cohort study including unruptured MIAs is needed to investigate the CMB risk factors of both unruptured IAs that eventually rupture and those that do not. Finally, we excluded patients with MIAs in whom the ruptured IA could not be identified; this may have caused selection bias.
Conclusions
Using a large multicentre cohort, we first devised and validated a nomogram, that is simple to use, for clinically evaluating the per-aneurysm rupture risk of patients with MIAs. Data on the seven independent factors included this nomogram are easy to obtain; these include: SAH history, alcohol consumption, sex, AR >1.5, PC, irregular shape and bifurcation location. With favourable calibration and discrimination, this nomogram may be useful for decision making and risk stratification in patients with MIAs.
Data availability statement
Some or all data, models or code generated or used during the study are available from the corresponding author by request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the institutional research ethics boards of Beijing Tiantan Hospital, Beijing Hospital, and Peking University International Hospital.
Acknowledgments
We thank Yuesong Pan from the China National Clinical Research Center for Neurological Diseases, for analysis and interpretation of data.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
XF and XT contributed equally.
AL and DW contributed equally.
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors DW and AL conceived and designed the study. FP, HN, YZ and WJ collected the data. PQ, JL, YZ and ZW were responsible for quality control. XF and XT conceived of the project, analysed the data and wrote the paper. All authors helped organised and carried out the research. All authors read and approved the final manuscript.
Funding This work was supported by the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (No. 2019TX320002) and the Natural Science Foundation of China (No. 81771233).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.